You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
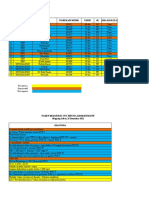
- Mapping Sabtu, 25 Desember 2021Document3 pagesMapping Sabtu, 25 Desember 2021Suis MionooNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
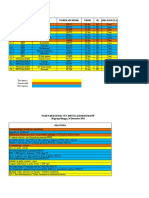
- Mapping Minggu, 26 Desember 2021Document3 pagesMapping Minggu, 26 Desember 2021Suis MionooNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
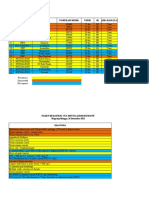
- Mapping Senin, 27 Desember 2021Document3 pagesMapping Senin, 27 Desember 2021Suis MionooNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pone 0233641Document15 pagesPone 0233641Suis MionooNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Mapping Jum'at, 24 Desember 2021Document4 pagesMapping Jum'at, 24 Desember 2021Suis MionooNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- An Anth 2016Document32 pagesAn Anth 2016Suis MionooNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Abruptio Placenta Retrospective Study: Maternal and Fetal OutcomeDocument4 pagesAbruptio Placenta Retrospective Study: Maternal and Fetal OutcomeSuis MionooNo ratings yet
- Case ReportDocument9 pagesCase ReportSuis MionooNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Pos Ok Hova 2012Document1 pagePos Ok Hova 2012Suis MionooNo ratings yet
- fef9d16481553837049874e411a5556eDocument17 pagesfef9d16481553837049874e411a5556eSuis MionooNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Diagnostics: Pyonephrosis Ultrasound and Computed Tomography Features: A Pictorial ReviewDocument12 pagesDiagnostics: Pyonephrosis Ultrasound and Computed Tomography Features: A Pictorial ReviewSuis MionooNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Research Open Access: Samoni Et Al. Critical Care (2016) 20:95 DOI 10.1186/s13054-016-1269-6Document8 pagesResearch Open Access: Samoni Et Al. Critical Care (2016) 20:95 DOI 10.1186/s13054-016-1269-6Suis MionooNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hill 2020Document2 pagesHill 2020Suis MionooNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- MCN 13157Document8 pagesMCN 13157Suis MionooNo ratings yet
- Nutrients: of Mice and Men-The Physiology, Psychology, and Pathology of OverhydrationDocument14 pagesNutrients: of Mice and Men-The Physiology, Psychology, and Pathology of OverhydrationSuis MionooNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- A Buddhist Approach To Stress Management: About Free Download BooksDocument31 pagesA Buddhist Approach To Stress Management: About Free Download BooksRonal JimNo ratings yet
- JPM 12 01580 - 2022Document10 pagesJPM 12 01580 - 2022mihail.boldeanuNo ratings yet
- Spirit Release TherapyDocument12 pagesSpirit Release Therapyravik38100% (6)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lesson 13 The Aspect of Gene TherapyDocument3 pagesLesson 13 The Aspect of Gene TherapyJamesMarniel AludoNo ratings yet
- Glaucoma Management Approach: Simple Literature ReviewDocument4 pagesGlaucoma Management Approach: Simple Literature ReviewElrach CorpNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Hypertension Concept MapDocument1 pageHypertension Concept Mapjyd parreñoNo ratings yet
- LUPALS Sexual Health and Contraception QuizDocument107 pagesLUPALS Sexual Health and Contraception QuizShan PatelNo ratings yet
- VTEDocument45 pagesVTEABREHAM BUKULONo ratings yet
- Tuberculosis NclexDocument3 pagesTuberculosis NclexMarinill SolimanNo ratings yet
- Alendronate SodiumDocument16 pagesAlendronate SodiumasdwasdNo ratings yet
- Slaber Jaga Senin 3 Mei 2021Document7 pagesSlaber Jaga Senin 3 Mei 2021Louis MailuhuNo ratings yet
- Diabetic Ketoacidosis: When To Suspect? How To Confirm?Document5 pagesDiabetic Ketoacidosis: When To Suspect? How To Confirm?Memory LastNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Long COVID or post-COVID-19 Syndrome Putative Pathophysiology, Risk FactorsDocument18 pagesLong COVID or post-COVID-19 Syndrome Putative Pathophysiology, Risk FactorsVane SchulzeNo ratings yet
- Metabolic Syndrome Thesis PDFDocument5 pagesMetabolic Syndrome Thesis PDFafknawjof100% (2)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Wa0027Document20 pagesWa0027Ahmed ElshiekhNo ratings yet
- ThesisofAhmedMusheerAl KhdriDocument159 pagesThesisofAhmedMusheerAl KhdriRex DullitNo ratings yet
- Cvboard - Study Strong PlannerDocument45 pagesCvboard - Study Strong PlannerZaina TNo ratings yet
- NURSING-CARE-PLAN-Lung-Cancerxxx 2Document3 pagesNURSING-CARE-PLAN-Lung-Cancerxxx 2Caroline ChaNo ratings yet
- AHA ACLS Megacode ScenariosDocument6 pagesAHA ACLS Megacode ScenariosVitor Hugo G Correia86% (7)
- 011ho10079 - Altatoyota Usa ProofDocument1 page011ho10079 - Altatoyota Usa ProofjoynahidNo ratings yet
- CHN Lec - Unit 1 and 2Document4 pagesCHN Lec - Unit 1 and 2Bryan MedranoNo ratings yet
- Symptom Management Obstruksi BowelDocument5 pagesSymptom Management Obstruksi BowelPutri Mega PetasiNo ratings yet
- Q4 English 8 - Module 3Document31 pagesQ4 English 8 - Module 3Sarahglen Ganob Lumanao100% (1)
- Chlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisDocument6 pagesChlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisjohnturpoNo ratings yet
- FBS - Forest HealthDocument52 pagesFBS - Forest HealthJoyce GomezNo ratings yet
- Screening For Cervical Cancer - UpToDateDocument40 pagesScreening For Cervical Cancer - UpToDateEvelin AlmeidaNo ratings yet
- "Customer Toward Preference Various Toothpaste Brand''Document74 pages"Customer Toward Preference Various Toothpaste Brand''bond9999985% (20)
- Nutrition and You 4Th Edition Blake Solutions Manual Full Chapter PDFDocument22 pagesNutrition and You 4Th Edition Blake Solutions Manual Full Chapter PDFinlawbast.ileir100% (9)
- Immature Schistosoma ReflexDocument2 pagesImmature Schistosoma Reflexpramod kumarNo ratings yet
- Liên T (26-7) PDFDocument4 pagesLiên T (26-7) PDFNhi LêNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)