You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Assessment of Gait: Karl Luigi L Lorilla, PTRPDocument27 pagesAssessment of Gait: Karl Luigi L Lorilla, PTRPJyrra NeriNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TRAINING PLAN 4-Way Split Version 2Document6 pagesTRAINING PLAN 4-Way Split Version 2adam100% (1)
- Self Massage TechniquesDocument24 pagesSelf Massage TechniquesI.S.100% (4)
- Range of Motion Procedure Checklist-1Document2 pagesRange of Motion Procedure Checklist-1api-288919673100% (2)
- Musculoskeletal Anatomy and PhysiologyDocument26 pagesMusculoskeletal Anatomy and PhysiologyAmy92% (13)
- Strength and Conditioning For Fencing.13Document6 pagesStrength and Conditioning For Fencing.13gregory tzortziadis100% (1)
- Parte 1 Bridgman's Complete Guide To Drawing From LifeDocument172 pagesParte 1 Bridgman's Complete Guide To Drawing From LifePatricia MilozziNo ratings yet
- Modalities and Physical Agents For The Rehab ProfessionalDocument6 pagesModalities and Physical Agents For The Rehab ProfessionalJyrra NeriNo ratings yet
- Kaltenbornmanualmobilizationsrs 150329041247 Conversion Gate01Document35 pagesKaltenbornmanualmobilizationsrs 150329041247 Conversion Gate01차성기No ratings yet
- PRIMITIVE REFLEX - FiorentinoDocument20 pagesPRIMITIVE REFLEX - FiorentinoLAMODAYAHOO.COMNo ratings yet
- Clinical Assessment of Musculoskeletal System-Handbook For MDocument36 pagesClinical Assessment of Musculoskeletal System-Handbook For MElqowiyyaNo ratings yet
- Tom Bisio - Ba Gua Nei Gong Marrow Washing Nei GongDocument111 pagesTom Bisio - Ba Gua Nei Gong Marrow Washing Nei GongIsidro Castaño Marquez75% (4)
- Finding Your Maximum Flexibility in YogaDocument10 pagesFinding Your Maximum Flexibility in Yogaadaminindia26No ratings yet
- BOOTY BY BRET MONTH 19 - January/February 2020: Week 1: Day 1 Set 1 Set 2 Set 3Document8 pagesBOOTY BY BRET MONTH 19 - January/February 2020: Week 1: Day 1 Set 1 Set 2 Set 3Diana CiupeiNo ratings yet
- Amputations Objectives: - AMBROISE PARE-created MoreDocument3 pagesAmputations Objectives: - AMBROISE PARE-created MoreJyrra NeriNo ratings yet
- Le Orthopedic Conditions: Ankle - Ankle SprainDocument9 pagesLe Orthopedic Conditions: Ankle - Ankle SprainJyrra NeriNo ratings yet
- Car CIA 2010Document26 pagesCar CIA 2010Jyrra NeriNo ratings yet
- Terminologies: Foot Condition - Achilles TendinitsDocument6 pagesTerminologies: Foot Condition - Achilles TendinitsJyrra NeriNo ratings yet
- Foot & Ankle International: Achilles TendinitisDocument7 pagesFoot & Ankle International: Achilles TendinitisJyrra NeriNo ratings yet
- Types of Traction: Erika Marie Rejas BSPT4Document6 pagesTypes of Traction: Erika Marie Rejas BSPT4Jyrra NeriNo ratings yet
- Capsular Ligament: Shoulder Anaphy-Jyrra NeriDocument6 pagesCapsular Ligament: Shoulder Anaphy-Jyrra NeriJyrra NeriNo ratings yet
- Chapter 12: The Back: Vertebral ColumnDocument7 pagesChapter 12: The Back: Vertebral ColumnJyrra NeriNo ratings yet
- Wed 2/16 - Review and Q&A Session Mon 2/21 - Midterm 1 Study Guide Is On Canvas Final Exam: 5/10, 2:30-5, CKB 204Document28 pagesWed 2/16 - Review and Q&A Session Mon 2/21 - Midterm 1 Study Guide Is On Canvas Final Exam: 5/10, 2:30-5, CKB 204Revanth VejjuNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Arthrography of Shoulder PDFDocument12 pagesArthrography of Shoulder PDFTanya GoriNo ratings yet
- A Guide To Flat Feet Children's Physiotherapy ServiceDocument2 pagesA Guide To Flat Feet Children's Physiotherapy ServiceEngineer ZAKARIANo ratings yet
- Btec Diploma in SportDocument2 pagesBtec Diploma in Sportapi-26052253No ratings yet
- IndianJPhysTherRes1279-7599768 210637Document10 pagesIndianJPhysTherRes1279-7599768 210637mNo ratings yet
- How Do We Walk?: Sujay Galen PT PHD FheaDocument52 pagesHow Do We Walk?: Sujay Galen PT PHD FheaColleen JohnsonNo ratings yet
- O' Level Biology Notes: 2020-01-27 Mr. F.Moyo - 0733214032Document21 pagesO' Level Biology Notes: 2020-01-27 Mr. F.Moyo - 0733214032Dion MunyanyiNo ratings yet
- Module 7 - 09Document18 pagesModule 7 - 09john frits gerard mombayNo ratings yet
- Reverse Lunge With Single-Arm Kettlebell Overhead PressDocument5 pagesReverse Lunge With Single-Arm Kettlebell Overhead PressSheril MarekNo ratings yet
- Exercitii ReabilitareDocument5 pagesExercitii ReabilitareGabriela Istrati-StanciugelNo ratings yet
- Toni Radić - Kuvar Sudnjeg DanaDocument19 pagesToni Radić - Kuvar Sudnjeg DanaĪzīdor Ĉech0% (1)
- Activity and Exercise PatternDocument20 pagesActivity and Exercise PatternRaquel M. MendozaNo ratings yet
- Hamstring Weakness After Surgery For Anterior Cruciate InjuryDocument4 pagesHamstring Weakness After Surgery For Anterior Cruciate InjuryAdrien VaillatNo ratings yet
- Open and Closed Kinetic Chain ExercisesDocument4 pagesOpen and Closed Kinetic Chain ExercisesJaymin BhattNo ratings yet
- Shoulder DislocationDocument13 pagesShoulder DislocationSahoo PRASANTANo ratings yet
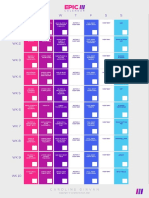
- EPIC III Program GuideDocument1 pageEPIC III Program GuideYAREN OZCANNo ratings yet
- OCSI Product CatalogDocument24 pagesOCSI Product CatalogP JNo ratings yet