You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ventriculoperitoneal ShuntDocument5 pagesVentriculoperitoneal ShunttameemNo ratings yet
- MedulloblastomaDocument35 pagesMedulloblastomatameemNo ratings yet
- CraniosynostosisDocument54 pagesCraniosynostosistameemNo ratings yet
- Langen&formatpdfDocument6 pagesLangen&formatpdftameemNo ratings yet
- 1 SSAhandbook FINAL Lowres - PDF - Spine Society of AustraliaDocument119 pages1 SSAhandbook FINAL Lowres - PDF - Spine Society of AustraliatameemNo ratings yet
- Exam Application OnliDocument1 pageExam Application OnlitameemNo ratings yet
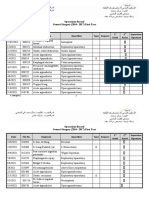
- Operations Record General Surgery (2016 - 2017) First YearDocument2 pagesOperations Record General Surgery (2016 - 2017) First YeartameemNo ratings yet
- Patients and MethodsDocument6 pagesPatients and MethodstameemNo ratings yet
- Surg LogBook Summary June 2019Document15 pagesSurg LogBook Summary June 2019tameem100% (1)
- Qdoc - Tips Skullbase-SurgeryDocument128 pagesQdoc - Tips Skullbase-SurgerytameemNo ratings yet
- Questionnaire: Personal DataDocument2 pagesQuestionnaire: Personal DatatameemNo ratings yet
- Neurology India 49 (94) : 94. Retrieved 2008-01-2014: "Contre-Coup Extradural Haematoma: A Short Report"Document3 pagesNeurology India 49 (94) : 94. Retrieved 2008-01-2014: "Contre-Coup Extradural Haematoma: A Short Report"tameemNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Case Study NCM 109 ApacibleDocument9 pagesCase Study NCM 109 ApacibleJade CentinoNo ratings yet
- Atlas of Mandibular and Maxillary Reconstruction With The FibulaDocument115 pagesAtlas of Mandibular and Maxillary Reconstruction With The FibulaOmar VillamizarNo ratings yet
- Latest IMM GuidelinesDocument14 pagesLatest IMM GuidelinesUsama1987No ratings yet
- Bone Void Fillers - JAAOS - Journal of The American Academy of Orthopaedic SurgeonsDocument5 pagesBone Void Fillers - JAAOS - Journal of The American Academy of Orthopaedic SurgeonsmuklisrivaiNo ratings yet
- Necrotizing Fasciitis Is A Rapidly Progressive Inflammatory Infection of The FasciaDocument5 pagesNecrotizing Fasciitis Is A Rapidly Progressive Inflammatory Infection of The FasciaMANASA AswathNo ratings yet
- Meta 4 - de Jong DM - 2022Document13 pagesMeta 4 - de Jong DM - 2022matheus.verasNo ratings yet
- Intestinal Atresia and StenosisDocument7 pagesIntestinal Atresia and StenosisMichael NafarinNo ratings yet
- NOTES 1st Sem P FDocument6 pagesNOTES 1st Sem P FReaNo ratings yet
- Mrs. Jincy Jiji AbrahamDocument5 pagesMrs. Jincy Jiji AbrahamSandeep ShahNo ratings yet
- Kan Et Al-2018-Periodontology 2000Document17 pagesKan Et Al-2018-Periodontology 2000Van nguyen hongNo ratings yet
- D500 BrochureDocument8 pagesD500 BrochureArbjan RusiNo ratings yet
- Frenectomy PDFDocument6 pagesFrenectomy PDFzinniaNo ratings yet
- Sky Ridge Medical Center Is The First in Colorado Open Dedicated Center For Robotics SurgeryDocument3 pagesSky Ridge Medical Center Is The First in Colorado Open Dedicated Center For Robotics SurgeryPR.comNo ratings yet
- الماف الذهبي ١ 2021 Corrected by Yes We CanDocument47 pagesالماف الذهبي ١ 2021 Corrected by Yes We CanlinahouhouNo ratings yet
- EMT Appendix 2 Medications and Skills MatrixDocument7 pagesEMT Appendix 2 Medications and Skills MatrixtrooperstuartNo ratings yet
- Perioperative Nursing Care 1Document17 pagesPerioperative Nursing Care 1Ardi CrisnaNo ratings yet
- Clinical Clues To The Causes of Large Pericardial EffusionsDocument7 pagesClinical Clues To The Causes of Large Pericardial EffusionsDewinsNo ratings yet
- Benign Salivary Gland Tumors - StatPearls - NCBI BookshelfDocument20 pagesBenign Salivary Gland Tumors - StatPearls - NCBI BookshelfMadhura Shekatkar100% (1)
- BlepharoplastyDocument2 pagesBlepharoplastyClara Verlina100% (1)
- Birthing Positions - HandoutDocument1 pageBirthing Positions - Handoutpooja singhNo ratings yet
- 10 1002@aorn 12696Document7 pages10 1002@aorn 12696Salim RumraNo ratings yet
- Allomax Surgical Graft Technique GuideDocument32 pagesAllomax Surgical Graft Technique Guidedr_kumananNo ratings yet
- 2015-Accuracy of Subthalamic Nucleus Targeting by T2, FLAIRDocument8 pages2015-Accuracy of Subthalamic Nucleus Targeting by T2, FLAIRPaul RodrigoNo ratings yet
- Reconstruction of The MPFLDocument12 pagesReconstruction of The MPFLhardboneNo ratings yet
- Vnus ClosurefastDocument2 pagesVnus ClosurefastBertha DuránNo ratings yet
- Dag Mas Reg TunnelingDocument3 pagesDag Mas Reg TunnelingBalaji V RNo ratings yet
- VIVA - TarrifDocument1 pageVIVA - TarrifSrinivas VadtheNo ratings yet
- Schematic Pathophysiology CVADocument10 pagesSchematic Pathophysiology CVAheiyu100% (5)
- Emergency Neurological Life Support - Traumatic Brain InjuryDocument13 pagesEmergency Neurological Life Support - Traumatic Brain Injurybrian leonardo gonzalez gomezNo ratings yet
- Cardiac Surgery Basic KnowledgeDocument28 pagesCardiac Surgery Basic KnowledgeGinwong100% (1)