You might also like
- Chronic PharyngitisDocument1 pageChronic PharyngitisHannah Angelu CabadingNo ratings yet
- Tonsillitis and AdenoiditisDocument12 pagesTonsillitis and AdenoiditisHannah Angelu CabadingNo ratings yet
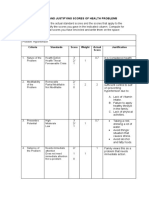
- C.2 Computing and Justifying Score of Health ProblemsDocument3 pagesC.2 Computing and Justifying Score of Health ProblemsHannah Angelu Cabading100% (1)
- Chronic PharyngitisDocument1 pageChronic PharyngitisHannah Angelu CabadingNo ratings yet
- Questions: Answer: Being A PHN Is Not As Simple As Some People Believe It Entails A Great Deal ofDocument1 pageQuestions: Answer: Being A PHN Is Not As Simple As Some People Believe It Entails A Great Deal ofHannah Angelu CabadingNo ratings yet
- Balcos, Andrea A.: Post Partum Exercises DefinitionDocument4 pagesBalcos, Andrea A.: Post Partum Exercises DefinitionHannah Angelu CabadingNo ratings yet
- ESSENTIAL INTRAPARTUM NEWBORN CARE (Assisting and Handling Delivery)Document4 pagesESSENTIAL INTRAPARTUM NEWBORN CARE (Assisting and Handling Delivery)Hannah Angelu CabadingNo ratings yet
- Breathing Techniques During Labor (Lamaze Method) : Procedure Rationale Rating RemarksDocument4 pagesBreathing Techniques During Labor (Lamaze Method) : Procedure Rationale Rating RemarksHannah Angelu CabadingNo ratings yet
- Immediate Newborn CareDocument5 pagesImmediate Newborn CareHannah Angelu Cabading50% (2)
- Cigarette Smoking: What It Is & What It'S NotDocument12 pagesCigarette Smoking: What It Is & What It'S NotHannah Angelu CabadingNo ratings yet
- IVF Drug StudyDocument5 pagesIVF Drug StudyHannah Angelu CabadingNo ratings yet
- MCN RLE Sitz Bath Procedure ChecklistDocument3 pagesMCN RLE Sitz Bath Procedure ChecklistHannah Angelu Cabading100% (1)
- NCP Dengue CabadingDocument3 pagesNCP Dengue CabadingHannah Angelu CabadingNo ratings yet
- Case Analysis Format Final DraftDocument53 pagesCase Analysis Format Final DraftHannah Angelu CabadingNo ratings yet
- Case Study Chapter 30Document2 pagesCase Study Chapter 30Hannah Angelu CabadingNo ratings yet
- Drug Study MetoprololDocument2 pagesDrug Study MetoprololHannah Angelu CabadingNo ratings yet
- Drug Study Module 4Document6 pagesDrug Study Module 4Hannah Angelu CabadingNo ratings yet
- AsepsisDocument4 pagesAsepsisHannah Angelu CabadingNo ratings yet
- NCM 61 Pharmacology - Digital Scrapbook-: By: Hannah Angelu S. Cabading Bsn2DDocument35 pagesNCM 61 Pharmacology - Digital Scrapbook-: By: Hannah Angelu S. Cabading Bsn2DHannah Angelu CabadingNo ratings yet
- Topic: Purpose:: Central Mindanao University College of Nursing Musuan, Maramag, BukidnonDocument3 pagesTopic: Purpose:: Central Mindanao University College of Nursing Musuan, Maramag, BukidnonHannah Angelu CabadingNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Education Model Based On Gamification Through Exclusive Breastfeeding Quartet Card Game To Improve Behavior and Self-Efficacy of Breastfeeding MothersDocument6 pagesEducation Model Based On Gamification Through Exclusive Breastfeeding Quartet Card Game To Improve Behavior and Self-Efficacy of Breastfeeding MothersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pharmaceutical and Health Care AssociationDocument47 pagesPharmaceutical and Health Care AssociationKenneth FabiaNo ratings yet
- Postpartum Teaching PlanDocument3 pagesPostpartum Teaching Plan6bigstar991% (11)
- Baby Food in Vietnam AnalysisDocument3 pagesBaby Food in Vietnam AnalysisAbdcNo ratings yet
- Postpartum Game Report: Self-Debriefing QuestionsDocument2 pagesPostpartum Game Report: Self-Debriefing QuestionsLouwella RamosNo ratings yet
- NLE Pediatric Nursing Pentagon ReviewerDocument65 pagesNLE Pediatric Nursing Pentagon Reviewerarcci balinas0% (1)
- BibliographyDocument6 pagesBibliographyPiyush DuttaNo ratings yet
- ATI PN Maternal Newborn NotesDocument13 pagesATI PN Maternal Newborn NotesDiamond Blackwell100% (6)
- First-Time Motherhood and Exclusive Breastfeeding Practice in Some Health Facilities in The Bushenyi DistrictDocument14 pagesFirst-Time Motherhood and Exclusive Breastfeeding Practice in Some Health Facilities in The Bushenyi DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Antenatal Info Booklet Intuitive BirthDocument32 pagesAntenatal Info Booklet Intuitive Birthapi-223713414No ratings yet
- XaxaxDocument3 pagesXaxaxDarren BalbasNo ratings yet
- LactationDocument24 pagesLactationJenyl Bajado100% (1)
- NTG in NCM 120 Decent Work Topic 2 Laws Affecting Nursing Practice in The PHDocument20 pagesNTG in NCM 120 Decent Work Topic 2 Laws Affecting Nursing Practice in The PHAntonette GrivialdeNo ratings yet
- Case 1 2 Nestle The Infant Formula ControversyDocument4 pagesCase 1 2 Nestle The Infant Formula ControversyboulevardkhoaNo ratings yet
- Mother's Class BFDocument55 pagesMother's Class BFriz04_fortitudessa5178No ratings yet
- Infant and Young Child Feeding Practices, Dietary Diversity and Their Association With Nutritional Status of Nomadic Children Under 5 Years of AgeDocument8 pagesInfant and Young Child Feeding Practices, Dietary Diversity and Their Association With Nutritional Status of Nomadic Children Under 5 Years of AgeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Attitude 0F Nursing Mothers Towards Exclusive Breast Feeding Among Maried Women Aged 18-45 YearsDocument47 pagesAttitude 0F Nursing Mothers Towards Exclusive Breast Feeding Among Maried Women Aged 18-45 YearsUsman Ahmad TijjaniNo ratings yet
- Student's Booklet - ReproductionDocument8 pagesStudent's Booklet - ReproductionRafa Rguez PerezNo ratings yet
- MNC Res 7. EO 51Document3 pagesMNC Res 7. EO 51ann29No ratings yet
- Evidance Based Dalam Kebidanan: Tugas IndividuDocument10 pagesEvidance Based Dalam Kebidanan: Tugas Individufalery nikitaNo ratings yet
- Complete Guide To Pediatric NusringDocument135 pagesComplete Guide To Pediatric NusringSANKARNo ratings yet
- Ineffective Breastfeeding - NCPDocument10 pagesIneffective Breastfeeding - NCPJullian PloyaNo ratings yet
- Pedia Case StudyDocument13 pagesPedia Case StudyAaron SalvadorNo ratings yet
- BreastfeedingDocument96 pagesBreastfeedingFayrouz EssawiNo ratings yet
- Wickes 1953 Part VDocument8 pagesWickes 1953 Part VTanya CassidyNo ratings yet
- Effectiveness of Different Massage Techniques For Breastfeeding Mothers To Increase Milk Production: A Systematic ReviewDocument17 pagesEffectiveness of Different Massage Techniques For Breastfeeding Mothers To Increase Milk Production: A Systematic ReviewdriveamadeaNo ratings yet
- Infant & Young Child Feeding in Emergencies: (IYCF E) andDocument59 pagesInfant & Young Child Feeding in Emergencies: (IYCF E) andRhea GaiaNo ratings yet
- Nestle and Its Unethical PracticesDocument8 pagesNestle and Its Unethical PracticesFiza Ali100% (1)
- Herbals and BreastfeedingDocument8 pagesHerbals and BreastfeedingArshad SyahaliNo ratings yet
- Lp1 ReviewerDocument17 pagesLp1 ReviewerNiña Ricci MtflcoNo ratings yet