You might also like
- Oxford Handbook of Expedition and Wilderness Medicine Oxford Medical Handbooks 3E Dec 6 2023 - 0198867018 - Oxford University Press Chris Johnson Full ChapterDocument68 pagesOxford Handbook of Expedition and Wilderness Medicine Oxford Medical Handbooks 3E Dec 6 2023 - 0198867018 - Oxford University Press Chris Johnson Full Chapterluis.ruppert131100% (5)
- Faust Anesthesiology Review PDFDocument2 pagesFaust Anesthesiology Review PDFAnna0% (7)
- Normal and Pathological Bronchial Semiology: A Visual ApproachFrom EverandNormal and Pathological Bronchial Semiology: A Visual ApproachPierre Philippe BaldeyrouNo ratings yet
- Basic Mode of Mechanical VentilationDocument53 pagesBasic Mode of Mechanical VentilationJihanitaNo ratings yet
- Covid y TraqueostomíaDocument9 pagesCovid y TraqueostomíaCatalina Muñoz VelasquezNo ratings yet
- Noninvasive Ventilation in Acute Respiratory Failure in AdultsDocument12 pagesNoninvasive Ventilation in Acute Respiratory Failure in AdultsferrevNo ratings yet
- Covid-19: Negative Pressure Rooms: Anmf Evidence BriefDocument5 pagesCovid-19: Negative Pressure Rooms: Anmf Evidence BriefninesuNo ratings yet
- Managing The Respiratory Care of Patients With COVID-19Document17 pagesManaging The Respiratory Care of Patients With COVID-19ManuelNo ratings yet
- KTP 1 RespiratoryDocument5 pagesKTP 1 RespiratoryMarisa TullochNo ratings yet
- Oxygenation and Ventilation in ERDocument61 pagesOxygenation and Ventilation in ERVarun PatelNo ratings yet
- Center For Physiotherapy and Rehabilitation Science Jamia Millia IslamiaDocument16 pagesCenter For Physiotherapy and Rehabilitation Science Jamia Millia IslamiaummiNo ratings yet
- Recommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionDocument5 pagesRecommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionConnor StephensonNo ratings yet
- Adult and Paediatric Oral/nasal-Pharyngeal SuctioningDocument13 pagesAdult and Paediatric Oral/nasal-Pharyngeal SuctioningRuby Dela RamaNo ratings yet
- COPD Acute Management ABCDEDocument11 pagesCOPD Acute Management ABCDESSNo ratings yet
- Cobis: Management of Airway Burns and Inhalation InjuryDocument6 pagesCobis: Management of Airway Burns and Inhalation InjuryTanitNo ratings yet
- Respiratory Tract InfectionsDocument26 pagesRespiratory Tract InfectionsyousefismailrootNo ratings yet
- CRT HintDocument47 pagesCRT HintEloisa Marie ReyesNo ratings yet
- Use of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaDocument10 pagesUse of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaLingga AniNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsEVINo ratings yet
- Respiratory Support For Adult Patients With COVID-19Document7 pagesRespiratory Support For Adult Patients With COVID-19SekarNo ratings yet
- Review: Stefano Nava, Nicholas HillDocument10 pagesReview: Stefano Nava, Nicholas HillLuis CortezNo ratings yet
- Pediatric Respiratory OverviewDocument4 pagesPediatric Respiratory OverviewPaul Saquido CapiliNo ratings yet
- Guidelines For The Management of Tracheal Intubation in Critically Ill AdultsDocument26 pagesGuidelines For The Management of Tracheal Intubation in Critically Ill AdultsFemiko Panji AprilioNo ratings yet
- Walls 8093 CH 01Document7 pagesWalls 8093 CH 01Adriana MartinezNo ratings yet
- The ABCDE ApproachDocument4 pagesThe ABCDE Approachazmar3No ratings yet
- Niv in Pediatric Patients - Book - GarciaDocument62 pagesNiv in Pediatric Patients - Book - GarciaMary ElizabethNo ratings yet
- Resuscitation GuidelinesDocument5 pagesResuscitation GuidelinesGemmith GosanesNo ratings yet
- Non-Invasive Positive Pressure Ventilation (Nippv)Document4 pagesNon-Invasive Positive Pressure Ventilation (Nippv)docsandyy78No ratings yet
- C 8 F 0 CF 2 F 9 C 13052842 DDocument11 pagesC 8 F 0 CF 2 F 9 C 13052842 DDewi Ji YongNo ratings yet
- AABIP Statement On Bronchoscopy COVID - 3 12 2020 Statement Plus 3 19 2020 Updates V3Document5 pagesAABIP Statement On Bronchoscopy COVID - 3 12 2020 Statement Plus 3 19 2020 Updates V3garinda almadutaNo ratings yet
- Anaesthesia and Caring For Patients During The COVID-19 OutbreakDocument8 pagesAnaesthesia and Caring For Patients During The COVID-19 OutbreakMuhammad RenaldiNo ratings yet
- Care of Newborn On Respiratory SupportDocument40 pagesCare of Newborn On Respiratory SupportsyedNo ratings yet
- Intubacion OrotraquealDocument20 pagesIntubacion OrotraquealEsteban TapiaNo ratings yet
- April 21st 2020 Muhc Code BlueDocument20 pagesApril 21st 2020 Muhc Code BlueS DNo ratings yet
- Intjprevmed6133-2704195 004504Document6 pagesIntjprevmed6133-2704195 004504Ade HabibieNo ratings yet
- 1 s2.0 S0733862722000384 MainDocument13 pages1 s2.0 S0733862722000384 Maincoca12451No ratings yet
- Et IndicationDocument20 pagesEt IndicationmisterlatteNo ratings yet
- Noninvasive VentilationDocument6 pagesNoninvasive VentilationEma MagfirahNo ratings yet
- Invasive and Noninvasive Pediatric Mechanical Ventilation: Ira M Cheifetz MD FAARCDocument17 pagesInvasive and Noninvasive Pediatric Mechanical Ventilation: Ira M Cheifetz MD FAARCAhmed Rizk AhmedNo ratings yet
- Tracheostomy Management During The COVID-19 PandemicDocument3 pagesTracheostomy Management During The COVID-19 Pandemicika lestariNo ratings yet
- COVID 19. 4 - 13 KashmerDocument42 pagesCOVID 19. 4 - 13 KashmerIshfaq GanaiNo ratings yet
- Care of The Ventilated ChildDocument5 pagesCare of The Ventilated ChildBrahadheeswaran KannanNo ratings yet
- Define The Acute Respiratory Distress ?: - Exudative - Proliferative - Fibrotic 1) ExudativeDocument6 pagesDefine The Acute Respiratory Distress ?: - Exudative - Proliferative - Fibrotic 1) ExudativenuraNo ratings yet
- Vent v1 Tom Extubation 001-EnDocument4 pagesVent v1 Tom Extubation 001-EnMuhammad AleemNo ratings yet
- Critical Care SuctioningDocument5 pagesCritical Care SuctioningChinta Nabila 조롱 수없는No ratings yet
- Airway Management and Common ConditionsDocument34 pagesAirway Management and Common Conditionsrigo montejoNo ratings yet
- ABCDE Approach To Emergency ManagementDocument20 pagesABCDE Approach To Emergency Managementluq9fifNo ratings yet
- 2022 Nasal Pyriform Aperture StenosisDocument2 pages2022 Nasal Pyriform Aperture StenosisNicolien van der PoelNo ratings yet
- Pediatric Advanced Life Support: Pedscases Podcast ScriptsDocument7 pagesPediatric Advanced Life Support: Pedscases Podcast ScriptsNoviNo ratings yet
- HELMETDocument11 pagesHELMETAndré MoutellaNo ratings yet
- JBLNPairwayDocument39 pagesJBLNPairwayjmscribblerNo ratings yet
- Fresh H1N1 Guidelines 1 - 1-18Document15 pagesFresh H1N1 Guidelines 1 - 1-18Shahid IqbalNo ratings yet
- 02a - PPE - Summary and Rationale For RecommendationsDocument2 pages02a - PPE - Summary and Rationale For RecommendationsMohammedNo ratings yet
- Rapid Sequence Intubation: BackgroundDocument8 pagesRapid Sequence Intubation: Backgroundmarsh86No ratings yet
- E868 FullDocument10 pagesE868 FullCalvin AffendyNo ratings yet
- Mechanism of Pulmonary Ventilation and Management of CovidDocument11 pagesMechanism of Pulmonary Ventilation and Management of CovidAubrey Unique EvangelistaNo ratings yet
- Airway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongDocument9 pagesAirway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongErwinRamadhaniNo ratings yet
- Managing Mechanical VentilationDocument7 pagesManaging Mechanical VentilationArden QuiambaoNo ratings yet
- Dissertation On PneumoniaDocument7 pagesDissertation On PneumoniaCustomWrittenPaperLittleRock100% (1)
- Management of Rare Causes of Pediatric Chronic Respiratory FailureDocument16 pagesManagement of Rare Causes of Pediatric Chronic Respiratory FailureISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Endotracheal TubeDocument19 pagesEndotracheal TubeSarvess Muniandy100% (1)
- Mepivacaine Vs BupivacaineDocument11 pagesMepivacaine Vs Bupivacainetia astrianaNo ratings yet
- Draeger E-Catalog Product - March 2023Document51 pagesDraeger E-Catalog Product - March 2023IrenNo ratings yet
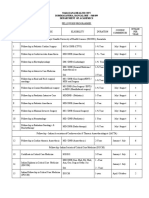
- Narayana Health City Bommasandra, Bangalore - 560 099 Department of AcademicsDocument2 pagesNarayana Health City Bommasandra, Bangalore - 560 099 Department of AcademicsEthan AmalNo ratings yet
- Hospital List District WiseDocument34 pagesHospital List District WiseArki100% (1)
- The COMFORT Behavior ScaleDocument5 pagesThe COMFORT Behavior ScaleLina Mahayaty SembiringNo ratings yet
- Local AnestheticsDocument44 pagesLocal Anestheticsblack pink in ur area 21No ratings yet
- Low Dose KetamineDocument4 pagesLow Dose KetamineAshiyan IrfanNo ratings yet
- Pengetahuan Penata Anestesi Tentang Kompetensi Pembimbing Klinik KeperawatanDocument7 pagesPengetahuan Penata Anestesi Tentang Kompetensi Pembimbing Klinik KeperawatanNaomi FriscaNo ratings yet
- 2017 Annual ReportDocument20 pages2017 Annual ReportCentral High School FoundationNo ratings yet
- Tintinalli - Chapter 37 Procedural Sedation and Analgesia in AdultsDocument11 pagesTintinalli - Chapter 37 Procedural Sedation and Analgesia in AdultsPgmee KimsNo ratings yet
- ANZCA Curriculum v1 10 May 2021Document311 pagesANZCA Curriculum v1 10 May 2021ghg sddNo ratings yet
- Hoja AnestesiaDocument9 pagesHoja AnestesiaCAMILO ANDRES MANTILLANo ratings yet
- Policy ScheduleDocument6 pagesPolicy ScheduleKaif AhmedNo ratings yet
- Chapter 2 The Medical Assistant and The Health Care TeamDocument30 pagesChapter 2 The Medical Assistant and The Health Care TeamAaron Wallace50% (2)
- List of Doctors Parans Update v4.0Document9 pagesList of Doctors Parans Update v4.0Franz CantaraNo ratings yet
- Anaesthesia For Neurosurgery-PIIS1472029919302656Document6 pagesAnaesthesia For Neurosurgery-PIIS1472029919302656james Wilson09No ratings yet
- Jurnal 5Document11 pagesJurnal 5Widya WibelNo ratings yet
- Anesthesia Control System With Multi Sen PDFDocument5 pagesAnesthesia Control System With Multi Sen PDF1020-Santhosh kumar. JNo ratings yet
- Gender M F Marital Status: Rizal Medical CenterDocument21 pagesGender M F Marital Status: Rizal Medical CentermaKitten08No ratings yet
- AlgorithmNeonatal Resuscitation 200615Document1 pageAlgorithmNeonatal Resuscitation 200615Ratna TambaNo ratings yet
- Nitrat Levophed: Rumus ..... Cc/jamDocument8 pagesNitrat Levophed: Rumus ..... Cc/jamRufiahNo ratings yet
- Recognized Ho So ListDocument77 pagesRecognized Ho So Listdp663668No ratings yet
- TM 6Document13 pagesTM 6Tya DwiNo ratings yet
- Ebp PresentationDocument30 pagesEbp Presentationapi-708254576No ratings yet
- Initial Resuscitation Algorithm For ChildrenDocument2 pagesInitial Resuscitation Algorithm For ChildrenDalia GomNo ratings yet
- Piper BerryDocument1 pagePiper Berryapi-459073199No ratings yet
- Anesthesia For Healthy Rabbits - Veterinary Anesthesia Update - VINDocument8 pagesAnesthesia For Healthy Rabbits - Veterinary Anesthesia Update - VINCristian FloreaNo ratings yet