You might also like
- R 03 Lifting and Shifting Work Permit (1)Document3 pagesR 03 Lifting and Shifting Work Permit (1)PRIYESH . K. PRIYANNo ratings yet
- Work at Heights PermitDocument4 pagesWork at Heights PermitFerdinand M. TurbanosNo ratings yet
- Confined Space Work PermitDocument2 pagesConfined Space Work PermitHariharan MuthukrishananNo ratings yet
- Cold Work PermitDocument3 pagesCold Work Permitnakul kushwahaNo ratings yet
- Work at Height Permit Form-2020Document2 pagesWork at Height Permit Form-2020Ebrahsm Elshenawy100% (1)
- Electrially Energized Area Entry PermitDocument1 pageElectrially Energized Area Entry PermitShahrukh Faizan AhmedNo ratings yet
- DIAL WORK PERMIT NewDocument5 pagesDIAL WORK PERMIT NewAkshay PotekarNo ratings yet
- General Work PermitDocument2 pagesGeneral Work PermitJareem PeesNo ratings yet
- Height Work SopDocument3 pagesHeight Work SopDhaneswar SwainNo ratings yet
- Format - Permit To Work 13.02.06 HSE OCP 01 F-01 R1Document4 pagesFormat - Permit To Work 13.02.06 HSE OCP 01 F-01 R1Gaurav Srivats100% (1)
- Electrical and Lifting Safety RequirementsDocument8 pagesElectrical and Lifting Safety RequirementsAnonymous kWfNFb100% (1)
- URC EHS 39 Lifting and Shifting Work PermitDocument2 pagesURC EHS 39 Lifting and Shifting Work PermitBala VelmuruganNo ratings yet
- Heigh Work Pemit - BlueDocument2 pagesHeigh Work Pemit - BlueAravind Babu Dasari100% (6)
- StudentStudymet581161 4Document4 pagesStudentStudymet581161 4CM VendhenNo ratings yet
- HSE Site Instruction For Contractor FormDocument1 pageHSE Site Instruction For Contractor FormAsif HussainNo ratings yet
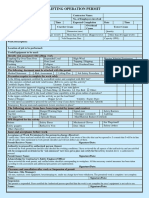
- Lifting Operation PermitDocument2 pagesLifting Operation PermitFMU KSA100% (2)
- Work at Heights PermitDocument4 pagesWork at Heights Permitrashid zamanNo ratings yet
- 3a - Sample Permit To Work TemplateDocument2 pages3a - Sample Permit To Work TemplateRavikant PandeyNo ratings yet
- Work in Confined Spaces - Take 5 Rev C FinalDocument2 pagesWork in Confined Spaces - Take 5 Rev C FinalVicky Ji100% (1)
- Excavation Safety ChecklistDocument2 pagesExcavation Safety Checklistsindarth raveendrakrishnanNo ratings yet
- 4A dm253461 Project Premobilization Safety Meeting Checklist PDFDocument19 pages4A dm253461 Project Premobilization Safety Meeting Checklist PDFRheNo ratings yet
- Excavation Work PermitDocument2 pagesExcavation Work Permitmuhammad.younisNo ratings yet
- Permit To Work FormatDocument1 pagePermit To Work FormatManager TrainingNo ratings yet
- Ocd Earthquake Drill Evaluation FormDocument1 pageOcd Earthquake Drill Evaluation FormAnonymous OJJ0qs2cjT100% (3)
- HAZARD CHECKLIST For (Workplace) Date . / / . Electrical Hazards Yes/ No To What Action Is Needed?Document5 pagesHAZARD CHECKLIST For (Workplace) Date . / / . Electrical Hazards Yes/ No To What Action Is Needed?Food TaxiNo ratings yet
- Lifting and Shifting of Heavy ObjectsDocument5 pagesLifting and Shifting of Heavy ObjectsChaitanya MyneniNo ratings yet
- OHSEC Permit System Rev 03Document91 pagesOHSEC Permit System Rev 03Avietcs MeiNo ratings yet
- Save Work Method of StatementDocument11 pagesSave Work Method of Statementpaansaeng50% (4)
- Wah PTWDocument1 pageWah PTWIvan NguyenNo ratings yet
- Contractor Environ & Safety FormDocument6 pagesContractor Environ & Safety Formsieged_rj3165No ratings yet
- Work at Height PermitDocument2 pagesWork at Height PermitYounis Khan81% (16)
- Field Inspection Report ExampleDocument35 pagesField Inspection Report Examplejinyuan7450% (4)
- Ig2-Latest Format AugustDocument24 pagesIg2-Latest Format AugustFaizan AliNo ratings yet
- Toolbox Meeting FormDocument2 pagesToolbox Meeting FormBenjamin Aregbesola100% (3)
- 02 - 07 Electrical Work PermitDocument1 page02 - 07 Electrical Work Permitmaxuya200150% (2)
- Sabic ExamDocument9 pagesSabic ExamSyed Ahmed manzoor100% (3)
- Halliburton Energy Services Hot Work PermitDocument48 pagesHalliburton Energy Services Hot Work PermitMed Hillel Elarouci67% (3)
- Hazard PagesDocument2 pagesHazard PagesShafique AsifNo ratings yet
- Demolition Method, ITP and Risk AssessmentDocument28 pagesDemolition Method, ITP and Risk Assessmentjones100% (5)
- Cold Work permit-WHITEDocument2 pagesCold Work permit-WHITEAravind Babu Dasari100% (1)
- Swms TemplateDocument8 pagesSwms Templateracing.phreakNo ratings yet
- Earthquake Drill Evaluation Form: Part I-General Evaluation: 1 2 3 4 5 Comments and ObservationsDocument2 pagesEarthquake Drill Evaluation Form: Part I-General Evaluation: 1 2 3 4 5 Comments and ObservationsJance Xavier Cabahug Vaflor100% (4)
- Job Safety Analysis FormDocument4 pagesJob Safety Analysis FormMohammed NayeemuddinNo ratings yet
- Block Work MSDocument19 pagesBlock Work MSjonesNo ratings yet
- Site survey workDocument24 pagesSite survey workShehzad MeharNo ratings yet
- LIFTING PERMITDocument2 pagesLIFTING PERMITsindarth raveendrakrishnan100% (1)
- Sitespecificsafetyplanmaster 150620153514 Lva1 App6891Document30 pagesSitespecificsafetyplanmaster 150620153514 Lva1 App6891Steven SengNo ratings yet
- Method Statement SampleDocument3 pagesMethod Statement SampleAmrith RajNo ratings yet
- Method of StatementDocument3 pagesMethod of StatementUmit CengNo ratings yet
- EPACK HSE MANAGEMENT SYSTEM AUDITDocument3 pagesEPACK HSE MANAGEMENT SYSTEM AUDITJyotiranjan RoutNo ratings yet
- Excavation Permit FormDocument2 pagesExcavation Permit FormazozinlcNo ratings yet
- Risk Awareness PollutionDocument32 pagesRisk Awareness PollutionReda HmrNo ratings yet
- Lifting & Erection Work ChecklistDocument1 pageLifting & Erection Work ChecklistSreejith SureshNo ratings yet
- 17 - Pressure Testing Permit (A4)Document1 page17 - Pressure Testing Permit (A4)Jianping KeNo ratings yet
- PTW-AUDIT-CHECKLISTDocument3 pagesPTW-AUDIT-CHECKLISTNabi AkramNo ratings yet
- Daily Checklist For SWPDocument2 pagesDaily Checklist For SWPtfpl hseNo ratings yet
- Successful Instrumentation and Control Systems Design, Second EditionFrom EverandSuccessful Instrumentation and Control Systems Design, Second EditionRating: 4.5 out of 5 stars4.5/5 (10)
- Method of Procedure (Mop) : 1. DescriptionDocument13 pagesMethod of Procedure (Mop) : 1. DescriptionRCGNo ratings yet
- Materials Transfer Form (MTF) : Logistics Team To Ensure Logistics-RFQ (L-RFQ) Is Properly Filled OutDocument1 pageMaterials Transfer Form (MTF) : Logistics Team To Ensure Logistics-RFQ (L-RFQ) Is Properly Filled OutRCGNo ratings yet
- Basic Functionality Test - Airscale: Web Browsing (Facebook)Document23 pagesBasic Functionality Test - Airscale: Web Browsing (Facebook)RCGNo ratings yet
- Certification: Department of HealthDocument2 pagesCertification: Department of HealthRCGNo ratings yet
- Lingat, Alvin (EXT-NSB - PH/Taguig City) : Please Below Guidelines On How To Register New User Site ForgeDocument6 pagesLingat, Alvin (EXT-NSB - PH/Taguig City) : Please Below Guidelines On How To Register New User Site ForgeRCGNo ratings yet
- Method of Procedure (Mop) : 1. DescriptionDocument10 pagesMethod of Procedure (Mop) : 1. DescriptionRCGNo ratings yet
- Advance Engineering TSSR for KINUSK MigrationDocument51 pagesAdvance Engineering TSSR for KINUSK MigrationRCGNo ratings yet
- Indoor Ground Photos: Additional Bbu BoardsDocument107 pagesIndoor Ground Photos: Additional Bbu BoardsRCGNo ratings yet
- Method of Procedure (Mop) : 1. DescriptionDocument10 pagesMethod of Procedure (Mop) : 1. DescriptionRCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- Method of Procedure (Mop) : 1. DescriptionDocument10 pagesMethod of Procedure (Mop) : 1. DescriptionRCGNo ratings yet
- Jessa Socias Cantilado: Brgy - Busay, Cebu City, Cebu 6000 Contact Numbers: 09300757504/09174654395Document2 pagesJessa Socias Cantilado: Brgy - Busay, Cebu City, Cebu 6000 Contact Numbers: 09300757504/09174654395RCGNo ratings yet
- Bëst in Test.: Smart PhilippinesDocument7 pagesBëst in Test.: Smart PhilippinesRCGNo ratings yet
- Letter (Cpa)Document2 pagesLetter (Cpa)RCGNo ratings yet
- Bacolod Application LetterDocument1 pageBacolod Application LetterRCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- Karen Angelica Bonganciso: ObjectiveDocument1 pageKaren Angelica Bonganciso: ObjectiveRCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- 867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)Document205 pages867520048641798-20 - 12 - 2018-11 - 17 - 24 (Band Lock L700)RCGNo ratings yet
- Online test series analysis reportDocument17 pagesOnline test series analysis reportchetan kapoorNo ratings yet
- 3152-4 Data SheetDocument2 pages3152-4 Data SheetPhuongNguyenDinhNo ratings yet
- Vernacular Terms in Philippine ConstructionDocument3 pagesVernacular Terms in Philippine ConstructionFelix Albit Ogabang IiiNo ratings yet
- PV380 Operations ManualDocument20 pagesPV380 Operations ManualCarlosNo ratings yet
- Glossary of Permafrost and Ground-Ice IPA 2005Document159 pagesGlossary of Permafrost and Ground-Ice IPA 2005NatitaGonzàlezDíazNo ratings yet
- Filed & Entered: SBN 143271 SBN 165797 SBN 259014Document8 pagesFiled & Entered: SBN 143271 SBN 165797 SBN 259014Chapter 11 DocketsNo ratings yet
- ES Model Question Paper With Solution KeyDocument10 pagesES Model Question Paper With Solution Keyvidhya_bineeshNo ratings yet
- Robert K Boscarato and Matthew Skaggs Corprate Credit Book Draft 1.Document70 pagesRobert K Boscarato and Matthew Skaggs Corprate Credit Book Draft 1.Robert BoscaratoNo ratings yet
- Professional Education ReviewerDocument22 pagesProfessional Education ReviewerJustine WicoNo ratings yet
- ID Strategi Integrated Marketing Communication Imc Untuk Meningkatkan Loyalitas AngDocument17 pagesID Strategi Integrated Marketing Communication Imc Untuk Meningkatkan Loyalitas AngAiman AzhariNo ratings yet
- B1 UDO Trace LogDocument14 pagesB1 UDO Trace LogCh M KashifNo ratings yet
- Studies of Land Restoration On Spoil Heaps From Brown Coal MiningDocument11 pagesStudies of Land Restoration On Spoil Heaps From Brown Coal MiningeftychidisNo ratings yet
- Literature Review On Waste Management in NigeriaDocument9 pagesLiterature Review On Waste Management in NigeriajzneaqwgfNo ratings yet
- Regional Campus The English and Foreign Languages UniversityDocument2 pagesRegional Campus The English and Foreign Languages UniversitySidra KhanNo ratings yet
- HistoryDocument20 pagesHistoryAlexandru RomînuNo ratings yet
- Uconnect User GuideDocument113 pagesUconnect User GuidetamilarasansrtNo ratings yet
- Rate of ChangeDocument22 pagesRate of ChangeTrisha MariehNo ratings yet
- V200 User ManualDocument171 pagesV200 User ManualuriahskyNo ratings yet
- C42135AA Beckman Coulter ClearLLab 10C Casebook PDFDocument586 pagesC42135AA Beckman Coulter ClearLLab 10C Casebook PDFHam Bone100% (1)
- KPW FSO Yetagun Presentation 250713Document36 pagesKPW FSO Yetagun Presentation 250713muhamadrafie1975No ratings yet
- IJPC 13 4 Hormone Replacement TherapyDocument92 pagesIJPC 13 4 Hormone Replacement TherapyMatiasNo ratings yet
- Food, Family, and FriendshipsDocument256 pagesFood, Family, and FriendshipsBianca PradoNo ratings yet
- SAP ABAP Interview Questions and AnswersDocument8 pagesSAP ABAP Interview Questions and AnswersKarthi ThirumalaisamyNo ratings yet
- Desantis, AlanDocument18 pagesDesantis, AlanOreillerNo ratings yet
- Diosdado MacapagalDocument13 pagesDiosdado MacapagalMermie ArmentaNo ratings yet
- FS Jack: Information GuideDocument12 pagesFS Jack: Information GuideGemma gladeNo ratings yet
- Studentwise Final Placement DetailsLast 3 YearsDocument18 pagesStudentwise Final Placement DetailsLast 3 YearsAmitNo ratings yet
- OTISLINE QuestionsDocument5 pagesOTISLINE QuestionsArvind Gupta100% (1)
- Business PolicyDocument17 pagesBusiness PolicyManish SinghNo ratings yet
- Photon BrochureDocument1 pagePhoton Brochureshwetha281889242No ratings yet