You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Development and Psychometric Properties of The Children's Assertive Behavior ScaleDocument11 pagesDevelopment and Psychometric Properties of The Children's Assertive Behavior ScaleSemut BarbarNo ratings yet
- Palmar Erythema: and Joseph C. English IIIDocument10 pagesPalmar Erythema: and Joseph C. English IIISemut BarbarNo ratings yet
- Urinary Tract InfectionsDocument6 pagesUrinary Tract InfectionsSemut BarbarNo ratings yet
- The Triple Compression Stress Test For Diagnosis of Tarsal Tunnel SyndromeDocument4 pagesThe Triple Compression Stress Test For Diagnosis of Tarsal Tunnel SyndromeSemut BarbarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Patho Safe Insert 04-2020V2Document3 pagesPatho Safe Insert 04-2020V2Luciano LopezNo ratings yet
- Prevent Complications in Lap CholecystectomyDocument23 pagesPrevent Complications in Lap CholecystectomyShashidhara PuttarajNo ratings yet
- Uk Guidelines SarcomaDocument21 pagesUk Guidelines Sarcomachu_chiang_3No ratings yet
- Hypertention and HypotentionDocument46 pagesHypertention and HypotentionAmanuel MaruNo ratings yet
- What Is An Ear InfectionDocument4 pagesWhat Is An Ear Infectionapi-236387116No ratings yet
- DERMA SPMC LeprosyDocument9 pagesDERMA SPMC LeprosyNicole Alexandra KhoNo ratings yet
- Drug StudyDocument4 pagesDrug StudyAilah Mae Dela Cruz0% (1)
- Analise Dinamica Sorriso - Mudanças Com A IdadeDocument2 pagesAnalise Dinamica Sorriso - Mudanças Com A IdadeCatia Sofia A PNo ratings yet
- Icd-10 Oktober 2021Document9 pagesIcd-10 Oktober 2021Nia KurniawatiNo ratings yet
- Hypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumDocument5 pagesHypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumMelodia Turqueza GandezaNo ratings yet
- Negative Inspiratory Pressure As A Predictor of Weaning Mechanical VentilationDocument3 pagesNegative Inspiratory Pressure As A Predictor of Weaning Mechanical VentilationamonlisaNo ratings yet
- Small Animal Surgery Internship - Proposed Program Description (2021)Document4 pagesSmall Animal Surgery Internship - Proposed Program Description (2021)Shubham HarishNo ratings yet
- Non Kepi Vaccines RevisedDocument28 pagesNon Kepi Vaccines Revisedokwadha simionNo ratings yet
- No. Name Position Monday Administration: Alternative Work Arrangement Jose C. Payumo Jr. Memorial High SchoolDocument35 pagesNo. Name Position Monday Administration: Alternative Work Arrangement Jose C. Payumo Jr. Memorial High SchoolJeremy Desoyo TorresNo ratings yet
- Lymphatic SystemDocument70 pagesLymphatic SystemNang Maizana Megat Yahya100% (1)
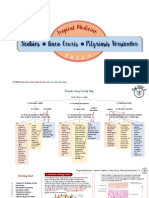
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Document11 pagesScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiNo ratings yet
- Information 13 00059 v2Document18 pagesInformation 13 00059 v2hendranatjNo ratings yet
- Essential Notes in Pain MedicineDocument737 pagesEssential Notes in Pain MedicineRichard Pertwee100% (5)
- Gordon's 11 Functional Health Patterns AssessmentDocument2 pagesGordon's 11 Functional Health Patterns Assessmentmtuckrn84% (37)
- Australian Dental Journal - 2015 - Ettinger - Treatment Planning Concepts For The Ageing PatientDocument15 pagesAustralian Dental Journal - 2015 - Ettinger - Treatment Planning Concepts For The Ageing PatientLorri - Ann LamontNo ratings yet
- Central Venous CatheterDocument5 pagesCentral Venous Catheterasmaa_gamal14No ratings yet
- Behandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Document217 pagesBehandlingstudier - Overblik Over Planlagte Og Igangværende Studier Af Lægemidler Til Behandling Af COVID-19Ishan ShahNo ratings yet
- Sample: Extract 1: Questions 31-36Document5 pagesSample: Extract 1: Questions 31-36Jorge VegaNo ratings yet
- Research Project ProposalDocument8 pagesResearch Project ProposalAthena Irish LastimosaNo ratings yet
- Intracellular AccumulationsDocument19 pagesIntracellular AccumulationsWajiha106No ratings yet
- AsthmaDocument46 pagesAsthmaHafiz Muhammad AeymonNo ratings yet
- Antimalarial DrugsDocument33 pagesAntimalarial DrugsPinakin Dhirajlal Jadav100% (1)
- Umblical Cord AbnormalitiesDocument54 pagesUmblical Cord AbnormalitiesKeerti Patel100% (5)
- Blood Collection TubesDocument1 pageBlood Collection TubesMohammad Atiq100% (1)
- Nephrectomy Nov16Document7 pagesNephrectomy Nov16Devanshi JoshiNo ratings yet