You might also like
- HIRARC For CONSTRUCTIONDocument12 pagesHIRARC For CONSTRUCTIONpalanitharan95% (59)
- Outpatient Care Facility: Assessment ChecklistDocument12 pagesOutpatient Care Facility: Assessment ChecklistHosam Gomaa0% (2)
- HICPAC Sample Audit Tool: Reprocessing Flexible EndoscopesDocument3 pagesHICPAC Sample Audit Tool: Reprocessing Flexible EndoscopesHosam Gomaa100% (1)
- SHEA Position Paper: I C H EDocument17 pagesSHEA Position Paper: I C H EIFRS SimoNo ratings yet
- 44 2 159Document19 pages44 2 159Nicole MariaNo ratings yet
- Clin Infect Dis.-2007-Dellit-159-77Document19 pagesClin Infect Dis.-2007-Dellit-159-77Melo PerezNo ratings yet
- Principi 2016Document8 pagesPrincipi 2016RaffaharianggaraNo ratings yet
- Cosgrove 2011Document16 pagesCosgrove 2011Dr. AveesNo ratings yet
- Antimicrobialstewardship Approachesinthe Intensivecareunit: Sarah B. Doernberg,, Henry F. ChambersDocument22 pagesAntimicrobialstewardship Approachesinthe Intensivecareunit: Sarah B. Doernberg,, Henry F. ChambersecaicedoNo ratings yet
- GPP No. 4 Antimicrobial StewardshipDocument1 pageGPP No. 4 Antimicrobial StewardshipKara PamittanNo ratings yet
- Antibiotics 11 00308Document17 pagesAntibiotics 11 00308Beatrice BănicăNo ratings yet
- Pattern of Researches Done On Antimicrobial Resistance in EthiopiaDocument16 pagesPattern of Researches Done On Antimicrobial Resistance in EthiopiaandualemNo ratings yet
- Antimicrobial StewardshipDocument7 pagesAntimicrobial StewardshipJohn TusselNo ratings yet
- Antimicrobial Stewardship Programs: Interventions and Associated OutcomesDocument14 pagesAntimicrobial Stewardship Programs: Interventions and Associated OutcomesGlory Claudia KarundengNo ratings yet
- Antibiotic PolicyDocument35 pagesAntibiotic PolicyArpita Garg100% (2)
- Antimicrobial Stewardship: Attempting To Preserve A Strategic ResourceDocument7 pagesAntimicrobial Stewardship: Attempting To Preserve A Strategic Resourcem1k0eNo ratings yet
- Antibiotic Stewardship in Critical Care: Ian Johnson MBCHB Frca and Victoria Banks Mbbs BSC Frca Fficm EdicDocument6 pagesAntibiotic Stewardship in Critical Care: Ian Johnson MBCHB Frca and Victoria Banks Mbbs BSC Frca Fficm EdicRavi KumarNo ratings yet
- ANA CDC AntibioticStewardship WhitePaperDocument14 pagesANA CDC AntibioticStewardship WhitePaperAndestaNo ratings yet
- ANA CDC Whitepaper AntibiotikDocument14 pagesANA CDC Whitepaper AntibiotikKomite PPI RSUDPCNo ratings yet
- Antimicrobial StewardshipDocument7 pagesAntimicrobial StewardshipMehwish MughalNo ratings yet
- Prof Hinky - STRATEGI PPI DLM PPRA 170324Document36 pagesProf Hinky - STRATEGI PPI DLM PPRA 170324m_amroellahNo ratings yet
- Implementing An Antibiotic Stewardship Program Guidelines by The Infectious Diseases Society of America and The Society For Healthcare Epidemiology of AmericaDocument27 pagesImplementing An Antibiotic Stewardship Program Guidelines by The Infectious Diseases Society of America and The Society For Healthcare Epidemiology of AmericaEnrique AlonsoNo ratings yet
- Interprofessional CollaboratioDocument16 pagesInterprofessional CollaboratioAnggito AbimanyuNo ratings yet
- Impact of Different Antimicrobial StewardshipDocument11 pagesImpact of Different Antimicrobial StewardshipAyush KumarNo ratings yet
- Antibiotics: Antibiotics and Antimicrobials Resistance: Mechanisms and New Strategies To Fight Resistant BacteriaDocument3 pagesAntibiotics: Antibiotics and Antimicrobials Resistance: Mechanisms and New Strategies To Fight Resistant BacteriaFernamdo GarciaNo ratings yet
- Importance of Infection Control PracticesDocument5 pagesImportance of Infection Control Practicesapi-3760696No ratings yet
- Antimicrobial Selection For The Equ 2021 Veterinary Clinics of North AmericaDocument34 pagesAntimicrobial Selection For The Equ 2021 Veterinary Clinics of North AmericaJuan Pardo CarrascoNo ratings yet
- ( (6) ) Jurnal CAPDocument9 pages( (6) ) Jurnal CAP6p5v5dvpffNo ratings yet
- 4.AMS Uso ATM De-Escalar 2020Document56 pages4.AMS Uso ATM De-Escalar 2020christian mezaNo ratings yet
- Antimicrobial StewardshipDocument19 pagesAntimicrobial StewardshipFelipe VicenteñoNo ratings yet
- Journal of Infection and ChemotherapyDocument13 pagesJournal of Infection and ChemotherapydrnguyenbvtkNo ratings yet
- Pharmacist Role in Infection ControlDocument3 pagesPharmacist Role in Infection ControlDaniel MesaNo ratings yet
- Frieri 2016Document10 pagesFrieri 2016Adil AnwarNo ratings yet
- AMR Action Plan - Role of AcademiaDocument55 pagesAMR Action Plan - Role of AcademiaShonit SharmaNo ratings yet
- JurnalDocument10 pagesJurnalIkaNo ratings yet
- Laude 2020Document9 pagesLaude 2020Heryanti PusparisaNo ratings yet
- Antibiotics 10 00550 v3Document20 pagesAntibiotics 10 00550 v3asdfasdNo ratings yet
- Antibiotics 10 00550 v3Document20 pagesAntibiotics 10 00550 v3HARDIYANTI TAKDIRNo ratings yet
- AAE Position StatementDocument5 pagesAAE Position StatementCarlos San MartinNo ratings yet
- Determinants Impacting The Use of Antibiotics Among Patients Visiting The Dental Clinic at Kampala International University Teaching Hospital in Bushenyi-Ishaka Municipality, WesteDocument15 pagesDeterminants Impacting The Use of Antibiotics Among Patients Visiting The Dental Clinic at Kampala International University Teaching Hospital in Bushenyi-Ishaka Municipality, WesteKIU PUBLICATION AND EXTENSIONNo ratings yet
- Dapus 2 8101-20729-3-PBDocument10 pagesDapus 2 8101-20729-3-PBLidya DiandraNo ratings yet
- General Practitioner Antimicrobial Stewardship Programme Study (GAPS) : Protocol For A Cluster Randomised Controlled TrialDocument9 pagesGeneral Practitioner Antimicrobial Stewardship Programme Study (GAPS) : Protocol For A Cluster Randomised Controlled TrialAlexandrahautaNo ratings yet
- Antimicrobial ResistanceDocument4 pagesAntimicrobial ResistanceDip Ayan MNo ratings yet
- The Pharmacist's Role in Preventing Antibiotic Resistance: Abstract and IntroductionDocument5 pagesThe Pharmacist's Role in Preventing Antibiotic Resistance: Abstract and IntroductionDeginaraNo ratings yet
- Role of The Pharmacist in Antimicrobial Stewardship: Rachel Fortin, Pharmd, BcpsDocument2 pagesRole of The Pharmacist in Antimicrobial Stewardship: Rachel Fortin, Pharmd, BcpsSih AtiiNo ratings yet
- Criterios Carat PDFDocument6 pagesCriterios Carat PDFGabrielaMirallesNo ratings yet
- AntibioticsDocument14 pagesAntibioticsBBD BBDNo ratings yet
- Principles of Initiating Antimicrobial Therapy and Empiric PrescribingDocument20 pagesPrinciples of Initiating Antimicrobial Therapy and Empiric Prescribingciaran100% (1)
- Antibiogram Toolkit 1Document30 pagesAntibiogram Toolkit 1EppySajaNo ratings yet
- Pharmacy: Antibiotic Stewardship in Community Pharmacies: A Scoping ReviewDocument11 pagesPharmacy: Antibiotic Stewardship in Community Pharmacies: A Scoping Reviewfarooq shikhNo ratings yet
- The Pharmacist - S Role in Preventing Antibiotic Resistance PDFDocument8 pagesThe Pharmacist - S Role in Preventing Antibiotic Resistance PDFalfox2000No ratings yet
- Prevention and Containment of Antimicrobial Resistance: Sixty-Third Session Bangkok, Thailand 7-10 September 2010Document17 pagesPrevention and Containment of Antimicrobial Resistance: Sixty-Third Session Bangkok, Thailand 7-10 September 2010gabriela_mariangela5929No ratings yet
- New Insight To Antibiotic ResistanceDocument25 pagesNew Insight To Antibiotic Resistancefatma omarNo ratings yet
- Thu 2012Document5 pagesThu 2012Nadila Hermawan PutriNo ratings yet
- Antibiotics or No Antibiotics That Is The Question PDFDocument20 pagesAntibiotics or No Antibiotics That Is The Question PDFJorge Ariel Viveros BlancoNo ratings yet
- AMIHAN, Ashley Mae - FA5 - CaseAnalysisDocument2 pagesAMIHAN, Ashley Mae - FA5 - CaseAnalysisAshley AmihanNo ratings yet
- Use of Antibiotic Therapy For Pediatric Dental Patients: Latest RevisionDocument4 pagesUse of Antibiotic Therapy For Pediatric Dental Patients: Latest Revisionnona aryanNo ratings yet
- Antimicrobial Stewardship and The Infection Control PractitionerDocument17 pagesAntimicrobial Stewardship and The Infection Control Practitionersilvia_guerra_1No ratings yet
- WHO Advocates 12 Key Interventions To Promote More Rational UseDocument4 pagesWHO Advocates 12 Key Interventions To Promote More Rational UseAsfa MarediaNo ratings yet
- Antibiotic Stewardship TING MING YEW P18090781Document20 pagesAntibiotic Stewardship TING MING YEW P18090781Ming Yew TingNo ratings yet
- Immunotherapy in Resistant Cancer: From the Lab Bench Work to Its Clinical PerspectivesFrom EverandImmunotherapy in Resistant Cancer: From the Lab Bench Work to Its Clinical PerspectivesJorge Morales-MontorNo ratings yet
- Campbell Systematic Reviews - 2021 - Chirgwin - Interventions Promoting Uptake of Water Sanitation and Hygiene WASHDocument79 pagesCampbell Systematic Reviews - 2021 - Chirgwin - Interventions Promoting Uptake of Water Sanitation and Hygiene WASHHosam GomaaNo ratings yet
- 1 s2.0 S2090123216000229 MainDocument10 pages1 s2.0 S2090123216000229 MainHosam GomaaNo ratings yet
- Countering Anti-Vaccination Rumors On TwitterDocument107 pagesCountering Anti-Vaccination Rumors On TwitterHosam GomaaNo ratings yet
- c5 Utility PlanDocument1 pagec5 Utility PlanHosam GomaaNo ratings yet
- Training Manual For State & District Surveillance Officers: Integrated Disease Surveillance ProjectDocument12 pagesTraining Manual For State & District Surveillance Officers: Integrated Disease Surveillance ProjectHosam GomaaNo ratings yet
- Fdi024 Evidence-Based Public Health What Does It Offer Developing CountriesDocument7 pagesFdi024 Evidence-Based Public Health What Does It Offer Developing CountriesHosam GomaaNo ratings yet
- Venkataramanan Et Al 2018 Community Led Total Sanitation A Mixed Methods Systematic Review of Evidence and Its QualityDocument17 pagesVenkataramanan Et Al 2018 Community Led Total Sanitation A Mixed Methods Systematic Review of Evidence and Its QualityHosam GomaaNo ratings yet
- Vaccine Hesitancy Outbreaks' Using Epidemiological Modeling of The Spread of Ideas To Understand The Effects of Vaccine Related Events On Vaccine HesitancyDocument25 pagesVaccine Hesitancy Outbreaks' Using Epidemiological Modeling of The Spread of Ideas To Understand The Effects of Vaccine Related Events On Vaccine HesitancyHosam GomaaNo ratings yet
- Misinformation, Believability, and Vaccine Acceptance Over 40 Countries Takeaways From The Initial Phase of The COVID-19 InfodemicDocument35 pagesMisinformation, Believability, and Vaccine Acceptance Over 40 Countries Takeaways From The Initial Phase of The COVID-19 InfodemicHosam GomaaNo ratings yet
- Checklist ChapterDocument11 pagesChecklist ChapterHosam GomaaNo ratings yet
- El Araby Infection ControlDocument1 pageEl Araby Infection ControlHosam GomaaNo ratings yet
- Eztest Steam: Geobacillus StearothermophilusDocument6 pagesEztest Steam: Geobacillus StearothermophilusHosam GomaaNo ratings yet
- List of 8 Enpact Employees - Find Emails & Phones - SignalHireDocument3 pagesList of 8 Enpact Employees - Find Emails & Phones - SignalHireHosam Gomaa0% (1)
- Quality Specialist: Health Care Specialist's Application FormDocument1 pageQuality Specialist: Health Care Specialist's Application FormHosam GomaaNo ratings yet
- 4419 Operational Risk SpecialistDocument2 pages4419 Operational Risk SpecialistHosam GomaaNo ratings yet
- Infection - Control - Coordinator Job DescriptionDocument64 pagesInfection - Control - Coordinator Job DescriptionHosam GomaaNo ratings yet
- 4204 Head, Financial, Strategic & Governance Risk JUNE 30, 2021Document2 pages4204 Head, Financial, Strategic & Governance Risk JUNE 30, 2021Hosam GomaaNo ratings yet
- 4418 Strategic & Governance Risk SpecialistDocument2 pages4418 Strategic & Governance Risk SpecialistHosam GomaaNo ratings yet
- AADNS - Infection Preventionist Job DescriptionDocument3 pagesAADNS - Infection Preventionist Job DescriptionHosam GomaaNo ratings yet
- 4420 Project Risk SpecialistDocument2 pages4420 Project Risk SpecialistHosam GomaaNo ratings yet
- General Infection Control Audit Checklist - SafetyCultureDocument21 pagesGeneral Infection Control Audit Checklist - SafetyCultureHosam Gomaa100% (1)
- Infection Control Guidelines: Ahmed AnwarDocument73 pagesInfection Control Guidelines: Ahmed AnwarHosam GomaaNo ratings yet
- Field Guide To Antibiotic StewardshipDocument30 pagesField Guide To Antibiotic StewardshipHosam GomaaNo ratings yet
- Facility Infection Control Assessment FormDocument6 pagesFacility Infection Control Assessment FormHosam GomaaNo ratings yet
- 02.culture Media Infection Control 26Document26 pages02.culture Media Infection Control 26Hosam GomaaNo ratings yet
- 03.CDC Standard Precautions 22Document22 pages03.CDC Standard Precautions 22Hosam GomaaNo ratings yet
- Mitanin Study FINALDocument37 pagesMitanin Study FINALAshok DadasNo ratings yet
- Lecture 1. Introduction To Dental Public HealthDocument26 pagesLecture 1. Introduction To Dental Public HealthHaneen Al-HajjNo ratings yet
- OH&SDocument19 pagesOH&SDwin RoscoNo ratings yet
- Decontamination Methods For 3M Filtering Facepiece Respirators Such As N95 RespiratorsDocument4 pagesDecontamination Methods For 3M Filtering Facepiece Respirators Such As N95 RespiratorsNirmala M. KarimatannisaNo ratings yet
- VaccineDocument1 pageVaccine羅啟豪No ratings yet
- Melliene Semblante's AbstractDocument2 pagesMelliene Semblante's AbstractCMU - College of Forestry and Environmental ScienceNo ratings yet
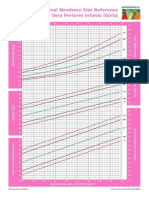
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- Water, Sanitation and Hygiene (Wash) Programme: Iom in ActionDocument2 pagesWater, Sanitation and Hygiene (Wash) Programme: Iom in ActionAhmedNo ratings yet
- OBGYN II Important QsDocument10 pagesOBGYN II Important QsDwivith ReddyNo ratings yet
- Analytical Exposition TextDocument4 pagesAnalytical Exposition TextNisa GhaisaniNo ratings yet
- CE 312 - Sewage Disposal in Unsewered Areas PDFDocument9 pagesCE 312 - Sewage Disposal in Unsewered Areas PDFkennysawegNo ratings yet
- ARP ESSER State PlanDocument64 pagesARP ESSER State PlaninforumdocsNo ratings yet
- A History of Caesarean Section: From Ancient World To The Modern EraDocument5 pagesA History of Caesarean Section: From Ancient World To The Modern EraGeorgiana DNo ratings yet
- History of Emergency Medical ServicesDocument8 pagesHistory of Emergency Medical Servicesapi-310488610No ratings yet
- Obstetrics - GynaecologyDocument137 pagesObstetrics - GynaecologyCiel100% (1)
- Gravidity and ParityDocument11 pagesGravidity and ParityShahad HakimuddinNo ratings yet
- PowepoinntDocument7 pagesPowepoinntapi-319343807No ratings yet
- Faktor-Faktor Yang Memengaruhi Kegagalan Inisiasi Menyusui Dini Pada Ibu Post Sectio Caesarea Di Rumah Sakit Tentara Binjai Tahun 2018Document14 pagesFaktor-Faktor Yang Memengaruhi Kegagalan Inisiasi Menyusui Dini Pada Ibu Post Sectio Caesarea Di Rumah Sakit Tentara Binjai Tahun 2018Salma AzzahraNo ratings yet
- Government of Rajasthan Finance Department Rules DivisionDocument2 pagesGovernment of Rajasthan Finance Department Rules DivisionSadanand PariharNo ratings yet
- Klasifikasi IMT WHODocument10 pagesKlasifikasi IMT WHOSubli MuhammadNo ratings yet
- The Use of Control ChartsDocument16 pagesThe Use of Control ChartsjcintpaNo ratings yet
- PRISMADocument5 pagesPRISMAGhany Hendra WijayaNo ratings yet
- Epidemiological Study of Bloody Diarrhoea Among Children in Baghdad, IraqDocument9 pagesEpidemiological Study of Bloody Diarrhoea Among Children in Baghdad, IraqInternational Medical PublisherNo ratings yet
- Trade Entrepreneur Engineering Pte LTD: Safe Work Procedure Title: Personal Protective EquipmentDocument7 pagesTrade Entrepreneur Engineering Pte LTD: Safe Work Procedure Title: Personal Protective EquipmentRachel NoraNo ratings yet
- Health-Declaration-Checklist 2Document1 pageHealth-Declaration-Checklist 2Beverly Trangia100% (2)
- Et 2011 Edhs PDFDocument450 pagesEt 2011 Edhs PDFhilegge7491No ratings yet
- Community-Based Approach For Dengue Prevention and Control in Sta. Cruz, Laguna, PhilippinesDocument7 pagesCommunity-Based Approach For Dengue Prevention and Control in Sta. Cruz, Laguna, PhilippinesBella LifindraNo ratings yet
- Cot 2 Health 6 - Lesson PlanDocument10 pagesCot 2 Health 6 - Lesson PlanAnna Clarissa TapallaNo ratings yet
- MCMC Presc A 02264 20240227 023546 0000Document1 pageMCMC Presc A 02264 20240227 023546 0000cleofeleighclarkNo ratings yet