You might also like
- Chapter 455 Retinoblastoma Retinoblastoma Charles B. Pratt: PathologyDocument4 pagesChapter 455 Retinoblastoma Retinoblastoma Charles B. Pratt: PathologyEbook Kedokteran Bahan KuliahNo ratings yet
- Reti No Blast OmaDocument54 pagesReti No Blast OmaSaviana Tieku100% (1)
- Retinoblastoma InglesDocument5 pagesRetinoblastoma InglesVlady BordaNo ratings yet
- Reti No Blast OmaDocument15 pagesReti No Blast OmaditaNo ratings yet
- Ocular Melanoma - StatPearls - NCBI BookshelfDocument6 pagesOcular Melanoma - StatPearls - NCBI BookshelfAnneAyushaNo ratings yet
- Common Conjunctival LesionsDocument4 pagesCommon Conjunctival LesionsSri AgustinaNo ratings yet
- 247 2011 Article 2201 PDFDocument13 pages247 2011 Article 2201 PDFArdianNo ratings yet
- Recent Advances in Retinoblastoma Management and GeneticsDocument12 pagesRecent Advances in Retinoblastoma Management and GeneticsDr Pranesh BalasubramaniamNo ratings yet
- Indian J Pediatr - Retinoblastoma: A ReviewDocument8 pagesIndian J Pediatr - Retinoblastoma: A ReviewVlady BordaNo ratings yet
- Masquerade SyndromeDocument69 pagesMasquerade Syndromerohitaswa100% (1)
- Retinoblastoma: An Overview: Review ArticleDocument6 pagesRetinoblastoma: An Overview: Review ArticledechastraNo ratings yet
- Jurnal Pendahuluan MutaDocument23 pagesJurnal Pendahuluan MutaMuta MimahNo ratings yet
- Tugas Besar: Makalah Retinoblastoma Modul Hematologi OnkologiDocument7 pagesTugas Besar: Makalah Retinoblastoma Modul Hematologi OnkologiKartikaSariNo ratings yet
- RetinoblastomaDocument24 pagesRetinoblastomaAzrinaNoor100% (1)
- Orbital Pathology: W. Müller-Forell, S. PitzDocument38 pagesOrbital Pathology: W. Müller-Forell, S. PitzArif Rahman WardhaniNo ratings yet
- Retinopathy of Prematurity & Retinoblastoma: Salinas & EstellaDocument23 pagesRetinopathy of Prematurity & Retinoblastoma: Salinas & Estellaallenh016No ratings yet
- Orbital Pathology, EJR 2004Document38 pagesOrbital Pathology, EJR 2004Mauricio FrancoNo ratings yet
- Uji PKDocument3 pagesUji PKRosmazila MohamadNo ratings yet
- (10920684 - Neurosurgical Focus) Tuberculum Sellae MeningiomasDocument6 pages(10920684 - Neurosurgical Focus) Tuberculum Sellae MeningiomasputriNo ratings yet
- Neoplasia OcularDocument18 pagesNeoplasia OcularRaul DiazNo ratings yet
- Baseline Evaluation and Management of RetinoblastomaDocument19 pagesBaseline Evaluation and Management of RetinoblastomaSiddharth KatyalNo ratings yet
- Retinal DetachmentDocument21 pagesRetinal Detachmentณัช เกษมNo ratings yet
- ICO Cases AnswerDocument128 pagesICO Cases AnswerAmr AbdulradiNo ratings yet
- Retinal Detachment Diagnosis and TreatmentDocument6 pagesRetinal Detachment Diagnosis and TreatmentDeasy Arindi PutriNo ratings yet
- Tumor of The EyeDocument40 pagesTumor of The EyeGustiAngriAngalanNo ratings yet
- ManagementDocument3 pagesManagementElison J PanggaloNo ratings yet
- Retinal DetachmentDocument8 pagesRetinal DetachmentJohanLazuardiNo ratings yet
- Imaging Findings of Intraventricular and Ependymal LesionsDocument16 pagesImaging Findings of Intraventricular and Ependymal Lesionsanggi abNo ratings yet
- B.2. 0Document7 pagesB.2. 0Bahna LucianNo ratings yet
- Retina/Vitreous: Question 1 of 130Document51 pagesRetina/Vitreous: Question 1 of 130safasayedNo ratings yet
- Case Presentation: DR Tariq Masood TMO Radiology Department, HMCDocument82 pagesCase Presentation: DR Tariq Masood TMO Radiology Department, HMCg1381821No ratings yet
- Reti No Blast OmaDocument11 pagesReti No Blast OmaNiluh Ita PasyantiNo ratings yet
- Data SCC From InternetDocument3 pagesData SCC From InternetristaniatauhidNo ratings yet
- Acquired Retinoschisis OCT FindingsDocument6 pagesAcquired Retinoschisis OCT FindingsSebaNo ratings yet
- A Case Report of Pilocytic Astrocytoma Mimicking Meningioma On ImagingDocument4 pagesA Case Report of Pilocytic Astrocytoma Mimicking Meningioma On ImagingIndra PrimaNo ratings yet
- Orbital Cellulitis: Causes, Symptoms and TreatmentDocument42 pagesOrbital Cellulitis: Causes, Symptoms and Treatmentmuhammad iqbalNo ratings yet
- Basal Cell Carcinoma: General FeaturesDocument5 pagesBasal Cell Carcinoma: General FeaturesSel ViaNo ratings yet
- Ba So CelularDocument13 pagesBa So CelularMihaela BubulacNo ratings yet
- August 2013 Ophthalmic PearlsDocument3 pagesAugust 2013 Ophthalmic PearlsEdi Saputra SNo ratings yet
- PROPTOSISDocument26 pagesPROPTOSISAhmad fayazNo ratings yet
- Frontal Sinus CholesteatomaDocument6 pagesFrontal Sinus CholesteatomaasiyazaidiaNo ratings yet
- common ophthalmic problem in childrenDocument68 pagescommon ophthalmic problem in childrenJoel ChongNo ratings yet
- Background: Frequency United StatesDocument5 pagesBackground: Frequency United StatesMohammadAwitNo ratings yet
- LEUKOKORIADocument3 pagesLEUKOKORIAFahlevie EpinNo ratings yet
- AAO Network CorneaDocument60 pagesAAO Network CorneaLydia Angelia YanitaNo ratings yet
- Update On Pterygium Therapy: Jay C. Bradley, MD David L. Mccartney, MD January Grand RoundsDocument28 pagesUpdate On Pterygium Therapy: Jay C. Bradley, MD David L. Mccartney, MD January Grand RoundsEnjiNo ratings yet
- Close Print: (Courtesy of R Bates - Fig. A A Pearson - Figs B and C)Document5 pagesClose Print: (Courtesy of R Bates - Fig. A A Pearson - Figs B and C)Primita Ayu DamayantiNo ratings yet
- Pterygium EmedicineDocument9 pagesPterygium EmedicineThomas SmithNo ratings yet
- Retinoblastoma and Management - A Post-Graduate Pocket Book Manjandavida FPDocument18 pagesRetinoblastoma and Management - A Post-Graduate Pocket Book Manjandavida FPSyeda F AmbreenNo ratings yet
- Complications Associated With Cataract SurgeryDocument24 pagesComplications Associated With Cataract SurgeryEvenjelina EveNo ratings yet
- Central Retinal Vein Occlusion and Branch Retinal Vein OcclusionDocument5 pagesCentral Retinal Vein Occlusion and Branch Retinal Vein OcclusionPOPPYNo ratings yet
- A Seminar Presentation On: University of Calabar Teaching Hospital Dept. of Ophthalmology Optometry UnitDocument32 pagesA Seminar Presentation On: University of Calabar Teaching Hospital Dept. of Ophthalmology Optometry UnitHogan ObiNo ratings yet
- MyopiaDocument11 pagesMyopiablueiceNo ratings yet
- Wa0024Document18 pagesWa0024Marlin 08No ratings yet
- Congenital Cataracts Causes, Symptoms and TreatmentDocument2 pagesCongenital Cataracts Causes, Symptoms and TreatmentKuchai BaruNo ratings yet
- Advances in RRD TreatmentDocument8 pagesAdvances in RRD TreatmentFathirNo ratings yet
- Leukocoria of Dermatology Sana'a UniversityDocument22 pagesLeukocoria of Dermatology Sana'a Universitylyricsmusica389No ratings yet
- Primary Retinal Detachment: Clinical PracticeDocument9 pagesPrimary Retinal Detachment: Clinical PracticeAdita DitaNo ratings yet
- Cranio Pha Ryn Gio MaDocument3 pagesCranio Pha Ryn Gio MaSerious LeoNo ratings yet
- Case No. 2: "HI LILY, HI LO"Document1 pageCase No. 2: "HI LILY, HI LO"Peter GirasolNo ratings yet
- PDR Case OpthaDocument1 pagePDR Case OpthaPeter GirasolNo ratings yet
- B1M5C1 Concept MapDocument1 pageB1M5C1 Concept MapPeter GirasolNo ratings yet
- Schwartz's Surgery 11e Chapter 17 The Breast AnatomyDocument4 pagesSchwartz's Surgery 11e Chapter 17 The Breast AnatomyPeter GirasolNo ratings yet
- Cdu-Cm PDR Iii Surgery Department: Facilitator: Dr. Abellana, Fritz Student: Girasol, Peter Paul BDocument4 pagesCdu-Cm PDR Iii Surgery Department: Facilitator: Dr. Abellana, Fritz Student: Girasol, Peter Paul BPeter GirasolNo ratings yet
- B1M5C1 Concept MapDocument1 pageB1M5C1 Concept MapPeter GirasolNo ratings yet
- B1M5C1 Concept MapDocument1 pageB1M5C1 Concept MapPeter GirasolNo ratings yet
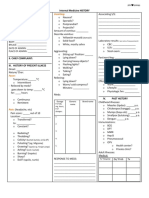
- Vomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Document4 pagesVomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Peter GirasolNo ratings yet
- Neurological exam testsDocument1 pageNeurological exam testsPeter GirasolNo ratings yet
- Block3Module2 Girasol PeterDocument2 pagesBlock3Module2 Girasol PeterPeter GirasolNo ratings yet
- Block3Module1 Girasol PeterDocument2 pagesBlock3Module1 Girasol PeterPeter GirasolNo ratings yet
- Block3Module1 Girasol PeterDocument2 pagesBlock3Module1 Girasol PeterPeter GirasolNo ratings yet
- F.L., A 20 Years Old Man: Auditory Hallucination and Paranoid DelusionDocument1 pageF.L., A 20 Years Old Man: Auditory Hallucination and Paranoid DelusionPeter GirasolNo ratings yet
- Schizophrenia and Related Disorders ComparisonDocument20 pagesSchizophrenia and Related Disorders ComparisonPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C1 Concept MapDocument1 page5A-Girasol-B6M3C1 Concept MapPeter GirasolNo ratings yet
- Parkinson's Disease Epidemiology Facts: Causes, Symptoms & PrevalenceDocument1 pageParkinson's Disease Epidemiology Facts: Causes, Symptoms & PrevalencePeter GirasolNo ratings yet
- Oup5.2019 - Data Processing and Analysis DataDocument24 pagesOup5.2019 - Data Processing and Analysis DataPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C2 Concept MapDocument1 page5A-Girasol-B6M3C2 Concept MapPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map (Updated) PDFDocument1 page5A-Girasol-B6M3C3 Concept Map (Updated) PDFPeter GirasolNo ratings yet
- (Format B.) Title of The ResearchDocument7 pages(Format B.) Title of The ResearchPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map PDFDocument1 page5A-Girasol-B6M3C3 Concept Map PDFPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C2 Concept MapDocument1 page5A-Girasol-B6M3C2 Concept MapPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map (Updated) PDFDocument1 page5A-Girasol-B6M3C3 Concept Map (Updated) PDFPeter GirasolNo ratings yet
- Stress and Coping Among Resident Doctors: October 2011Document21 pagesStress and Coping Among Resident Doctors: October 2011Claudiu TeodorescuNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map PDFDocument1 page5A-Girasol-B6M3C3 Concept Map PDFPeter GirasolNo ratings yet
- Stress and Coping Among Resident Doctors: October 2011Document21 pagesStress and Coping Among Resident Doctors: October 2011Peter GirasolNo ratings yet
- 5A-Girasol-B6M3C1 Concept MapDocument1 page5A-Girasol-B6M3C1 Concept MapPeter GirasolNo ratings yet
- Job Satisfaction Work Stress and Turnover IntentioDocument11 pagesJob Satisfaction Work Stress and Turnover IntentioPeter GirasolNo ratings yet
- Determinants of Job Satisfaction Among Physicians in Public HospitalsDocument15 pagesDeterminants of Job Satisfaction Among Physicians in Public HospitalsAmirahShalehaNo ratings yet
- SOYER Bend Testing Device BP-1Document2 pagesSOYER Bend Testing Device BP-1abdulla_alazzawiNo ratings yet
- Book Notes - The Life Changing Magic of Tidying Up PDFDocument6 pagesBook Notes - The Life Changing Magic of Tidying Up PDFAilyn Bagares AñanoNo ratings yet
- Nature and Purpose of CommunicationDocument17 pagesNature and Purpose of CommunicationEdmond Dantès100% (4)
- Hps40 Tech Doc ScreenDocument20 pagesHps40 Tech Doc ScreenAnonymous oyUAtpKNo ratings yet
- Fruit-Gathering by Tagore, Rabindranath, 1861-1941Document46 pagesFruit-Gathering by Tagore, Rabindranath, 1861-1941Gutenberg.orgNo ratings yet
- Connect 4 UML Class DiagramDocument1 pageConnect 4 UML Class DiagramDuy Nguyễn Văn NhậtNo ratings yet
- BOM RMCC Parking-Shed Rev2Document15 pagesBOM RMCC Parking-Shed Rev2Ephrem Marx AparicioNo ratings yet
- Giáo Trình LPTD 2Document40 pagesGiáo Trình LPTD 2Hưng Trịnh TrọngNo ratings yet
- TaxonomyDocument56 pagesTaxonomyKrezia Mae SolomonNo ratings yet
- Insert - Elecsys Anti-HBs II - Ms - 05894816190.V2.EnDocument4 pagesInsert - Elecsys Anti-HBs II - Ms - 05894816190.V2.EnyantuNo ratings yet
- Basic of Seismic RefractionDocument43 pagesBasic of Seismic Refractionfitriah wulandariNo ratings yet
- Sublime Union: A Womans Sexual Odyssey Guided by Mary Magdalene (Book Two of The Magdalene Teachings) Download Free BookDocument4 pagesSublime Union: A Womans Sexual Odyssey Guided by Mary Magdalene (Book Two of The Magdalene Teachings) Download Free Bookflavia cascarinoNo ratings yet
- Barcode BasicsDocument3 pagesBarcode Basicsnikhilbajpai_88No ratings yet
- Lesson Plan in ESPDocument4 pagesLesson Plan in ESPkaren daculaNo ratings yet
- Ultra FXDocument17 pagesUltra FXmanikumar0No ratings yet
- Engine Rear Oil Seal PDFDocument3 pagesEngine Rear Oil Seal PDFDIEGONo ratings yet
- SAP MM ReportsDocument59 pagesSAP MM Reportssaprajpal95% (21)
- The Essential Guide To Data in The Cloud:: A Handbook For DbasDocument20 pagesThe Essential Guide To Data in The Cloud:: A Handbook For DbasInes PlantakNo ratings yet
- FND Global and FND Profile PDFDocument4 pagesFND Global and FND Profile PDFSaquib.MahmoodNo ratings yet
- Get TRDocDocument209 pagesGet TRDoc10131No ratings yet
- SDRRM Earthquake Drill TemplateDocument3 pagesSDRRM Earthquake Drill TemplateChristian Bonne MarimlaNo ratings yet
- TC-21FJ30LA: Service ManualDocument33 pagesTC-21FJ30LA: Service ManualRajo Peto alamNo ratings yet
- CENELEC RA STANDARDS CATALOGUEDocument17 pagesCENELEC RA STANDARDS CATALOGUEHamed AhmadnejadNo ratings yet
- Workbook. Unit 3. Exercises 5 To 9. RESPUESTASDocument3 pagesWorkbook. Unit 3. Exercises 5 To 9. RESPUESTASRosani GeraldoNo ratings yet
- Basic Computer Quiz - MCQ on Components, Generations & HistoryDocument7 pagesBasic Computer Quiz - MCQ on Components, Generations & Historyprem sagar100% (2)
- (Leon 2021) Pengaruh Financial Distress, Laverage Terhadap Konservatisme Akuntansi Pada Perusahaan Manfaktur Sektor Konsumsi 2016-2019Document24 pages(Leon 2021) Pengaruh Financial Distress, Laverage Terhadap Konservatisme Akuntansi Pada Perusahaan Manfaktur Sektor Konsumsi 2016-2019PUTRI AYU HASTUTINo ratings yet
- Al-Jahiz (781-869) : ZoologyDocument25 pagesAl-Jahiz (781-869) : ZoologyJA QuibzNo ratings yet
- Enzyme KineticsDocument13 pagesEnzyme KineticsMohib100% (1)
- Cse 3003: Computer Networks: Dr. Sanket Mishra ScopeDocument56 pagesCse 3003: Computer Networks: Dr. Sanket Mishra ScopePOTNURU RAM SAINo ratings yet
- Hele 4 PPT - 2nd QT - Week 1Document47 pagesHele 4 PPT - 2nd QT - Week 1jerico juarezNo ratings yet