You might also like
- NCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDocument5 pagesNCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDud AccNo ratings yet
- General History and Physical Examination FormDocument2 pagesGeneral History and Physical Examination FormQueen Hera100% (1)
- Pediatric Assessment 1 12 PDFDocument11 pagesPediatric Assessment 1 12 PDFJackieNate Ortiz100% (1)
- 2014 Group Case StudyDocument42 pages2014 Group Case StudyBrian100% (1)
- Essential Oils and Supplements For Strokes: StrokeDocument4 pagesEssential Oils and Supplements For Strokes: StrokeEmese Földesi100% (1)
- Pediatric History OutlineDocument12 pagesPediatric History OutlineDawn MarcoNo ratings yet
- FP Form1 V3.0 2016Document3 pagesFP Form1 V3.0 2016Lorenz Joey Ricarte100% (2)
- Pentacam GuidelineDocument43 pagesPentacam GuidelineEvelyn SepulvedaNo ratings yet
- Gordon S Functional Health Pattern Assessment ToolDocument17 pagesGordon S Functional Health Pattern Assessment Toolmiss RN96% (45)
- Diet and Its TypesDocument11 pagesDiet and Its Typesanita100% (1)
- My Other Bag’s a Prada: Quick and Dirty Tips for Surviving an Ileostomy: Quick and Dirty Tips for Surviving, #2From EverandMy Other Bag’s a Prada: Quick and Dirty Tips for Surviving an Ileostomy: Quick and Dirty Tips for Surviving, #2No ratings yet
- Sample TranscriptDocument2 pagesSample TranscriptTejas Shah67% (3)
- Night BeforeDocument3 pagesNight BeforeChris MoffettNo ratings yet
- Gordon S Functional Health Pattern Assessment TooL: EdisonDocument13 pagesGordon S Functional Health Pattern Assessment TooL: EdisonEdison Olad Dangkeo, RN,RM67% (3)
- Health Screening and Assessment Form - SampleDocument3 pagesHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Gordons Functional Health Pattern Assessment Tool (Bano, R.)Document3 pagesGordons Functional Health Pattern Assessment Tool (Bano, R.)ojay880% (1)
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYClaire FNo ratings yet
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYNorjetalexis CabreraNo ratings yet
- PatienthistoryformenglishDocument4 pagesPatienthistoryformenglishRuriko IkusawaNo ratings yet
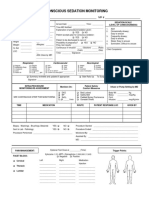
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Neuropreceptorial ChecklistDocument33 pagesNeuropreceptorial ChecklistAlloiBialba0% (1)
- Pediatric History Taking Chart PDFDocument2 pagesPediatric History Taking Chart PDFHerlene Lyneth ZalamedaNo ratings yet
- History TakingDocument6 pagesHistory Takingdharti daveNo ratings yet
- Health Survey FormDocument3 pagesHealth Survey FormJazel SanchezNo ratings yet
- Worksheets InepDocument12 pagesWorksheets InepReina SamsonNo ratings yet
- MayelinBenedictoRodriguez ClientForms 042922Document5 pagesMayelinBenedictoRodriguez ClientForms 042922Cosmo Salón & SpaNo ratings yet
- Pediatric AssessmentDocument6 pagesPediatric AssessmentChu BagunuNo ratings yet
- Hasil Pemeriksaan Kesehatan: I. General Data / Data PribadiDocument3 pagesHasil Pemeriksaan Kesehatan: I. General Data / Data PribadiAoeliaZulkarneinNo ratings yet
- OB Patho Assessment Tool EditedDocument6 pagesOB Patho Assessment Tool EditedDarren RobertoNo ratings yet
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
- Cuadernillo: Lengua, Literatura Y Sus Tecnologías. Lengua Extranjera "Inglés" Plan Común SemanaDocument3 pagesCuadernillo: Lengua, Literatura Y Sus Tecnologías. Lengua Extranjera "Inglés" Plan Común SemanaIsabel GodoyNo ratings yet
- FNCPDocument5 pagesFNCPCarina QuibinitNo ratings yet
- CRT 7Document8 pagesCRT 7api-643868511No ratings yet
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDocument29 pagesForm "D" Report of Practical Experience: Nursing Clinical Practice IAnderson RebaNo ratings yet
- Prenatal Nutrition and Immunization: Demographics OB HistoryDocument19 pagesPrenatal Nutrition and Immunization: Demographics OB HistorynivraeNo ratings yet
- Assessment Tool On Neurological System: Baseline DataDocument21 pagesAssessment Tool On Neurological System: Baseline DataK HepsibaNo ratings yet
- Live @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsDocument5 pagesLive @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsJoy SalvadorNo ratings yet
- Paediatrics History + Examination Format-2Document4 pagesPaediatrics History + Examination Format-2Salim KhaleelNo ratings yet
- Para Lab Module 1 NotesDocument4 pagesPara Lab Module 1 NotesJoyce LeeNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document21 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "allen zacariasNo ratings yet
- GordonsDocument2 pagesGordonsAngelica OctotNo ratings yet
- Primary Skin Care Patient History and Physical ExaDocument2 pagesPrimary Skin Care Patient History and Physical ExaNur kahnNo ratings yet
- Commed Template Family Report 2 1Document18 pagesCommed Template Family Report 2 1Ge NavNo ratings yet
- Ateneo Higher Education Health Services Office Ateneo de Naga University Ateneo Avenue, Bagumbayan Sur, Naga CityDocument2 pagesAteneo Higher Education Health Services Office Ateneo de Naga University Ateneo Avenue, Bagumbayan Sur, Naga CityKatherine VerceluzNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document6 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruNo ratings yet
- Pediatric Intake Form SampleDocument10 pagesPediatric Intake Form SampleТравма ЮніверсумNo ratings yet
- Nursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718Document14 pagesNursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718jelaNo ratings yet
- Health Declaration Form - A1 Whole Page - ADocument1 pageHealth Declaration Form - A1 Whole Page - AMARCK JOHN EUSTAQUIONo ratings yet
- Health AssessmentDocument12 pagesHealth Assessmentjmzxmdy597No ratings yet
- Exercise 2 - FP Form 1 A and B (1) TDocument2 pagesExercise 2 - FP Form 1 A and B (1) TJohn Alfred TanNo ratings yet
- Preguntas A Paciente Antes Del Tratamiento Mucositis OnsDocument2 pagesPreguntas A Paciente Antes Del Tratamiento Mucositis OnsSilvia DaphnaNo ratings yet
- 8.) Health-and-Medical-Profile Template Ver.2Document4 pages8.) Health-and-Medical-Profile Template Ver.2SocialWelfare SilangNo ratings yet
- Patients Profile RegaladoDocument5 pagesPatients Profile RegaladoAngelo ArabejoNo ratings yet
- Outline For Patient InterviewDocument2 pagesOutline For Patient InterviewMavic VillanuevaNo ratings yet
- LenghwiseDocument2 pagesLenghwiseAnna Margarett Mutia CaballarNo ratings yet
- COVID-19 DECLARATION FORM HCW Version 4 2021 (BI) NewDocument1 pageCOVID-19 DECLARATION FORM HCW Version 4 2021 (BI) NewNorliza Che DaudNo ratings yet
- LTTC CWD IE TemplateDocument6 pagesLTTC CWD IE TemplateClaire De VeraNo ratings yet
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- Operation Ugly Truth Nurse Firsthand account of the NYC Pandemic 2020From EverandOperation Ugly Truth Nurse Firsthand account of the NYC Pandemic 2020No ratings yet
- Living Without Fear During Covid-19 (and Other Difficult Times)From EverandLiving Without Fear During Covid-19 (and Other Difficult Times)No ratings yet
- B1M5C1 Concept MapDocument1 pageB1M5C1 Concept MapPeter GirasolNo ratings yet
- Case No. 2: "HI LILY, HI LO"Document1 pageCase No. 2: "HI LILY, HI LO"Peter GirasolNo ratings yet
- PDR Case OpthaDocument1 pagePDR Case OpthaPeter GirasolNo ratings yet
- Ophtha NotesDocument4 pagesOphtha NotesPeter GirasolNo ratings yet
- Cdu-Cm PDR Iii Surgery Department: Facilitator: Dr. Abellana, Fritz Student: Girasol, Peter Paul BDocument4 pagesCdu-Cm PDR Iii Surgery Department: Facilitator: Dr. Abellana, Fritz Student: Girasol, Peter Paul BPeter GirasolNo ratings yet
- Schwartz's Surgery 11e Chapter 17 The Breast AnatomyDocument4 pagesSchwartz's Surgery 11e Chapter 17 The Breast AnatomyPeter GirasolNo ratings yet
- Block3Module1 Girasol PeterDocument2 pagesBlock3Module1 Girasol PeterPeter GirasolNo ratings yet
- F.L., A 20 Years Old Man: Auditory Hallucination and Paranoid DelusionDocument1 pageF.L., A 20 Years Old Man: Auditory Hallucination and Paranoid DelusionPeter GirasolNo ratings yet
- B1M5C1 Concept MapDocument1 pageB1M5C1 Concept MapPeter GirasolNo ratings yet
- Parkinson's Disease (PD) EpidemiologyDocument1 pageParkinson's Disease (PD) EpidemiologyPeter GirasolNo ratings yet
- B1M5C1 (Kaplan 11ed Chapter 7) Schizophrenia Schizoaffective Disorder Schizophreniform Disorder Delusional Disorder Brief Psychotic DisorderDocument20 pagesB1M5C1 (Kaplan 11ed Chapter 7) Schizophrenia Schizoaffective Disorder Schizophreniform Disorder Delusional Disorder Brief Psychotic DisorderPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map (Updated) PDFDocument1 page5A-Girasol-B6M3C3 Concept Map (Updated) PDFPeter GirasolNo ratings yet
- B1M5C1 Concept MapDocument1 pageB1M5C1 Concept MapPeter GirasolNo ratings yet
- Block3Module2 Girasol PeterDocument2 pagesBlock3Module2 Girasol PeterPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map (Updated) PDFDocument1 page5A-Girasol-B6M3C3 Concept Map (Updated) PDFPeter GirasolNo ratings yet
- Block3Module1 Girasol PeterDocument2 pagesBlock3Module1 Girasol PeterPeter GirasolNo ratings yet
- NEURO - Retdem: A. Testing For Corneal Reflex (CN5 & CN7 Test)Document1 pageNEURO - Retdem: A. Testing For Corneal Reflex (CN5 & CN7 Test)Peter GirasolNo ratings yet
- 5A-Girasol-B6M3C2 Concept MapDocument1 page5A-Girasol-B6M3C2 Concept MapPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C1 Concept MapDocument1 page5A-Girasol-B6M3C1 Concept MapPeter GirasolNo ratings yet
- Oup5.2019 - Data Processing and Analysis DataDocument24 pagesOup5.2019 - Data Processing and Analysis DataPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C1 Concept MapDocument1 page5A-Girasol-B6M3C1 Concept MapPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C2 Concept MapDocument1 page5A-Girasol-B6M3C2 Concept MapPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map PDFDocument1 page5A-Girasol-B6M3C3 Concept Map PDFPeter GirasolNo ratings yet
- (Format B.) Title of The ResearchDocument7 pages(Format B.) Title of The ResearchPeter GirasolNo ratings yet
- 5A-Girasol-B6M3C3 Concept Map PDFDocument1 page5A-Girasol-B6M3C3 Concept Map PDFPeter GirasolNo ratings yet
- Stress and Coping Among Resident Doctors: October 2011Document21 pagesStress and Coping Among Resident Doctors: October 2011Claudiu TeodorescuNo ratings yet
- Stress and Coping Among Resident Doctors: October 2011Document21 pagesStress and Coping Among Resident Doctors: October 2011Peter GirasolNo ratings yet
- Determinants of Job Satisfaction Among Physicians in Public HospitalsDocument15 pagesDeterminants of Job Satisfaction Among Physicians in Public HospitalsAmirahShalehaNo ratings yet
- Job Satisfaction Work Stress and Turnover IntentioDocument11 pagesJob Satisfaction Work Stress and Turnover IntentioPeter GirasolNo ratings yet
- Prenatal Care: Williams ObstetricsDocument43 pagesPrenatal Care: Williams Obstetricsgayon09No ratings yet
- Module 3-4: Writing Argumentative Essay - Page - 1Document28 pagesModule 3-4: Writing Argumentative Essay - Page - 1Jan Den Saul DalanNo ratings yet
- 2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Document63 pages2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Andy DazNo ratings yet
- Nursing Care Plan Surgical PDFDocument2 pagesNursing Care Plan Surgical PDFDanielle Audrey100% (2)
- 09 Apr 2021: UPSC Exam Comprehensive News Analysis: A. GS 1 Related B. GS 2 RelatedDocument12 pages09 Apr 2021: UPSC Exam Comprehensive News Analysis: A. GS 1 Related B. GS 2 RelatedArpita Sen BhattacharyaNo ratings yet
- The Effects of Covid 19 To BusinessesDocument3 pagesThe Effects of Covid 19 To BusinessesMark PadernalNo ratings yet
- A. Obesity Is A Huge Problem in Many Western Countries and One Which NowDocument6 pagesA. Obesity Is A Huge Problem in Many Western Countries and One Which NowĐỗ Thị Thuý NgaNo ratings yet
- Antihypertensive Drugs - Classification and SynthesisDocument14 pagesAntihypertensive Drugs - Classification and SynthesisCường NguyễnNo ratings yet
- CBME Time Table Phase - II 2022Document36 pagesCBME Time Table Phase - II 2022IrfanNo ratings yet
- COVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare ProfessionalsDocument3 pagesCOVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare Professionalsvarshasharma05No ratings yet
- RF LatexDocument1 pageRF LatexDinesh SreedharanNo ratings yet
- Women Health and SanitationDocument15 pagesWomen Health and SanitationPratima MukherjeeNo ratings yet
- Language and Students With Mental RetardationDocument22 pagesLanguage and Students With Mental Retardationmat2489100% (4)
- HLTH 301 - Plo 2 ArtifactDocument6 pagesHLTH 301 - Plo 2 Artifactapi-625564017No ratings yet
- PSI INDIA - Will Balbir Pasha Help Fight AIDS: Target AudienceDocument2 pagesPSI INDIA - Will Balbir Pasha Help Fight AIDS: Target AudienceShambhawi SinhaNo ratings yet
- Health StatisticsDocument43 pagesHealth Statisticsramanand chaudharyNo ratings yet
- Emergency Procedures and Primary Care in Physical Therapy: A Practice ManualDocument32 pagesEmergency Procedures and Primary Care in Physical Therapy: A Practice ManualBushra MehwishNo ratings yet
- Tiered Response AgreementDocument3 pagesTiered Response AgreementThe Hamilton SpectatorNo ratings yet
- Chronic Sialadenitis With Sialolithiasis Associated With Parapharyngeal Fistula and TonsillolithDocument4 pagesChronic Sialadenitis With Sialolithiasis Associated With Parapharyngeal Fistula and TonsillolithguleriamunishNo ratings yet
- The LipomaDocument35 pagesThe Lipomaسوما الشمريNo ratings yet
- Cataract Refract Surg, 35 (2), 273-276.: NISITA SURYANTO, Prof. Dr. Suhardjo, SU., SP.M (K) . Dr. Hartono, SP.M (K)Document4 pagesCataract Refract Surg, 35 (2), 273-276.: NISITA SURYANTO, Prof. Dr. Suhardjo, SU., SP.M (K) . Dr. Hartono, SP.M (K)peachandmintsNo ratings yet
- Saunders Lumbar TractionDocument12 pagesSaunders Lumbar TractionIra AdventiaNo ratings yet
- Scoring Systems in Anesthesia and PACUDocument16 pagesScoring Systems in Anesthesia and PACUmissyaaaaNo ratings yet
- The Powerful Impact of StressDocument19 pagesThe Powerful Impact of StressMichael Angelo SeñaNo ratings yet
- Bacteria Resistance To Antibiotics Science Fair ProjectDocument3 pagesBacteria Resistance To Antibiotics Science Fair ProjectZaina ImamNo ratings yet