You might also like
- Trauma and Its ComplicationsDocument80 pagesTrauma and Its Complicationsjoe BouGhazaliNo ratings yet
- Management of Life-Threatening Electrolyte and Metabolic DisturbancesDocument27 pagesManagement of Life-Threatening Electrolyte and Metabolic Disturbanceserwilli5No ratings yet
- Selected Skeletal Muscles 10 BlankDocument6 pagesSelected Skeletal Muscles 10 BlankPrabhjot BaghaNo ratings yet
- Bio 102 Handout Muscular SysDocument3 pagesBio 102 Handout Muscular Sysgjsup100% (1)
- Disasters and Mass Casualty Incidents: The Nuts and Bolts of Preparedness and Response to Protracted and Sudden Onset EmergenciesFrom EverandDisasters and Mass Casualty Incidents: The Nuts and Bolts of Preparedness and Response to Protracted and Sudden Onset EmergenciesMauricio LynnNo ratings yet
- Initial Assessment and Management: Presented by Fayez Abillama, MDDocument53 pagesInitial Assessment and Management: Presented by Fayez Abillama, MDDaniel GhosseinNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Weakness B WDocument62 pagesWeakness B WKhan A RehNo ratings yet
- Causes Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As AnDocument22 pagesCauses Obstruction Causes CSF To Build Up in The Brain. If The Cause Is Congenital, Symptoms Such As Anmhelandie100% (1)
- ShockDocument21 pagesShockNyakie MotlalaneNo ratings yet
- Microcirculation as Related to ShockFrom EverandMicrocirculation as Related to ShockDavid SheproNo ratings yet
- Emergency Medical Procedures GuideDocument57 pagesEmergency Medical Procedures GuideDuane Liloc100% (1)
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Head TraumaDocument22 pagesHead TraumaEllsay AliceNo ratings yet
- Febrile Seizure: Satanun Charoencholvanich, MDDocument10 pagesFebrile Seizure: Satanun Charoencholvanich, MDAPETT WichaiyoNo ratings yet
- Paediatric Emergencies NotesDocument6 pagesPaediatric Emergencies NotesJana AldourNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- A Clinical Approach To SyncopeDocument8 pagesA Clinical Approach To Syncopepuskesmas tarik100% (1)
- TraumaBurn ClinicalGuidelines Final PDFDocument34 pagesTraumaBurn ClinicalGuidelines Final PDFJuan Antonio GarcíaNo ratings yet
- Critical Care SedationFrom EverandCritical Care SedationAngelo Raffaele De GaudioNo ratings yet
- Neuro Notes #3Document11 pagesNeuro Notes #3Monica JubaneNo ratings yet
- Anaerobic Infections in HumansFrom EverandAnaerobic Infections in HumansSydney FinegoldRating: 5 out of 5 stars5/5 (1)
- Alphabet-Course-Breakdown-Nccp 1Document3 pagesAlphabet-Course-Breakdown-Nccp 1api-232950579No ratings yet
- Snake Bite Medical ManagementDocument35 pagesSnake Bite Medical Managementsyarifah nurlailaNo ratings yet
- Higher Mental Function Examination Dementia, Altered MentalDocument37 pagesHigher Mental Function Examination Dementia, Altered MentalCamille DoamanNo ratings yet
- Guidelines For The Management of Severe Traumatic Brain Injury 4th EditionDocument62 pagesGuidelines For The Management of Severe Traumatic Brain Injury 4th EditionNailahRahmahNo ratings yet
- CNSexam PDFDocument8 pagesCNSexam PDFkarthiktsvmcNo ratings yet
- Wellen EcgDocument9 pagesWellen EcgElokNo ratings yet
- Nursing Care of Clients in Emergency Situation 2Document52 pagesNursing Care of Clients in Emergency Situation 2Danica FrancoNo ratings yet
- 2 - Airway and Ventilatory ManagementDocument5 pages2 - Airway and Ventilatory ManagementJessie E. GeeNo ratings yet
- Neuroscience I - Neurologic History Taking and Examination (POBLETE)Document9 pagesNeuroscience I - Neurologic History Taking and Examination (POBLETE)Johanna Hamnia PobleteNo ratings yet
- ATLS (Advanced Trauma Life Support) Teaching Protocol Pretest (30 Min) Context of Tutorial (2 Hours)Document16 pagesATLS (Advanced Trauma Life Support) Teaching Protocol Pretest (30 Min) Context of Tutorial (2 Hours)anon_778118144No ratings yet
- Retropharyngeal AbscessDocument23 pagesRetropharyngeal AbscessParul GuptaNo ratings yet
- Anes AirwayDocument24 pagesAnes AirwayyanaNo ratings yet
- Surface Anatomy Palpation & Myotomes ReviewDocument5 pagesSurface Anatomy Palpation & Myotomes ReviewHyy5No ratings yet
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocument15 pagesPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNo ratings yet
- Examination of ThyroidDocument4 pagesExamination of ThyroidNoor Ul AinNo ratings yet
- Trauma OverviewDocument48 pagesTrauma OverviewFrancescoBarbero100% (1)
- Respiratory EmergenciesDocument21 pagesRespiratory EmergenciesMohamed Anas SayedNo ratings yet
- MS Brain and Neurological DisordersDocument5 pagesMS Brain and Neurological DisordershaxxxessNo ratings yet
- CPR ACLS Study GuideDocument18 pagesCPR ACLS Study GuideJohn Phamacy100% (1)
- Peadiatric Brain Tumour: Wong Ann Cheng MD (Ukm) MRCPCH (Uk)Document48 pagesPeadiatric Brain Tumour: Wong Ann Cheng MD (Ukm) MRCPCH (Uk)An Zheng100% (4)
- Ent Emergencies: DR Mohammad Almayouf Associat Consultant ENTDocument27 pagesEnt Emergencies: DR Mohammad Almayouf Associat Consultant ENTMuhammad ANo ratings yet
- 20 - Toronto Notes 2011 - Ophthamology PDFDocument46 pages20 - Toronto Notes 2011 - Ophthamology PDFSisterzzShopDua0% (1)
- Acute Respiratory Distress: Section I: Scenario DemographicsDocument6 pagesAcute Respiratory Distress: Section I: Scenario DemographicsharasthaNo ratings yet
- Word Part ReviewDocument6 pagesWord Part ReviewRanee ToNo ratings yet
- Basic Ecg 2016Document75 pagesBasic Ecg 2016api-284503860No ratings yet
- Anatomic LocalizationDocument9 pagesAnatomic Localizationkid100% (1)
- Bio 235 Midterm 1 NotesDocument53 pagesBio 235 Midterm 1 NotesNita JosephNo ratings yet
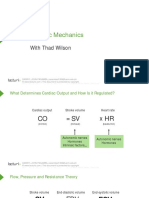
- Cardiac Mechanics: With Thad WilsonDocument26 pagesCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNo ratings yet
- Neurologic EmergenciesDocument194 pagesNeurologic Emergenciesapi-205902640No ratings yet
- Open Fracture ManagementDocument44 pagesOpen Fracture ManagementNur Liyana Ahmad ZakiNo ratings yet
- A2 Prostate Ca - AinDocument4 pagesA2 Prostate Ca - AinNur Liyana Ahmad ZakiNo ratings yet
- Orthopedic Clerking TemplateDocument4 pagesOrthopedic Clerking TemplateNur Liyana Ahmad ZakiNo ratings yet
- Ortho DevicesDocument22 pagesOrtho DevicesNur Liyana Ahmad ZakiNo ratings yet
- Open Fracture ManagementDocument44 pagesOpen Fracture ManagementNur Liyana Ahmad ZakiNo ratings yet
- SCRIPT OrthoDocument20 pagesSCRIPT OrthoNur Liyana Ahmad ZakiNo ratings yet
- Easyscore Microb - GameDocument21 pagesEasyscore Microb - GameNur Liyana Ahmad ZakiNo ratings yet
- RespirationDocument40 pagesRespirationNur Liyana Ahmad ZakiNo ratings yet
- Jadual ENTDocument1 pageJadual ENTNur Liyana Ahmad ZakiNo ratings yet
- N Memory of DRDocument3 pagesN Memory of DRNur Liyana Ahmad ZakiNo ratings yet
- Model Exam Paper-1Document0 pagesModel Exam Paper-1Nur Liyana Ahmad ZakiNo ratings yet
- Presentation BiochemDocument40 pagesPresentation BiochemNur Liyana Ahmad ZakiNo ratings yet
- AGN and NSDocument2 pagesAGN and NSNur Liyana Ahmad ZakiNo ratings yet
- Coal WorkersDocument14 pagesCoal WorkersNur Liyana Ahmad ZakiNo ratings yet
- Respiratory 1Document2 pagesRespiratory 1Nur Liyana Ahmad ZakiNo ratings yet
- Neuro PatientDocument11 pagesNeuro PatientNur Liyana Ahmad ZakiNo ratings yet
- 5TH YearDocument9 pages5TH YearNur Liyana Ahmad ZakiNo ratings yet
- MicrobeDocument4 pagesMicrobeNur Liyana Ahmad ZakiNo ratings yet
- ECG BasicsDocument98 pagesECG BasicsNur Liyana Ahmad ZakiNo ratings yet
- AsthmaDocument45 pagesAsthmaNur Liyana Ahmad ZakiNo ratings yet
- SleDocument66 pagesSleNur Liyana Ahmad Zaki100% (1)
- Lower GIT BleedingDocument50 pagesLower GIT BleedingNur Liyana Ahmad ZakiNo ratings yet
- Acute Viral HepatitisDocument2 pagesAcute Viral HepatitisNur Liyana Ahmad ZakiNo ratings yet
- 5th Year Oral QDocument10 pages5th Year Oral QNur Liyana Ahmad ZakiNo ratings yet
- Suppurative Lung DIseaseDocument33 pagesSuppurative Lung DIseaseNur Liyana Ahmad ZakiNo ratings yet
- Naemi Root Crop Rat Killer ResearchDocument3 pagesNaemi Root Crop Rat Killer ResearchJerome BumagatNo ratings yet
- Xii Physical Education PracticalDocument3 pagesXii Physical Education PracticalAayush AdlakNo ratings yet
- Lecture Notes 12&13 Phylum ApicomplexaDocument20 pagesLecture Notes 12&13 Phylum ApicomplexaAmirr4uddinNo ratings yet
- Gym Membership AgreementDocument3 pagesGym Membership Agreementzde thai100% (1)
- PFC Katalog PPDocument128 pagesPFC Katalog PPbmsinghNo ratings yet
- Alpha Full CaseDocument5 pagesAlpha Full CaseAnonymous 4IOzjRIB1No ratings yet
- Goat anatomy and physiology guideDocument8 pagesGoat anatomy and physiology guideLochi GmNo ratings yet
- The Scientific Facts About WaterDocument7 pagesThe Scientific Facts About WaterNizam HasniNo ratings yet
- Disease Causation 2Document32 pagesDisease Causation 2andualem werkinehNo ratings yet
- ReportDocument1 pageReportRanjan Mano100% (1)
- Lab Report 1 Biology PhotosynthesisDocument4 pagesLab Report 1 Biology PhotosynthesisSarthak PatelNo ratings yet
- M6 Artificial Disc Failure Report (1st Part)Document21 pagesM6 Artificial Disc Failure Report (1st Part)Keanu ReevesNo ratings yet
- Steps in Balancing Redox ReactionsDocument28 pagesSteps in Balancing Redox ReactionsRUZCHEMISTRYNo ratings yet
- TDS - Rheofinish 288 FDDocument2 pagesTDS - Rheofinish 288 FDVenkata RaoNo ratings yet
- Cessna 208 (B) Caravan I T.T.R.Document7 pagesCessna 208 (B) Caravan I T.T.R.Junior Mebude SimbaNo ratings yet
- Spain-Final ProjectDocument29 pagesSpain-Final Projectapi-264431075No ratings yet
- Cat TH360B Telehandler Operator and Maintanence Manual PDFDocument164 pagesCat TH360B Telehandler Operator and Maintanence Manual PDFB.H100% (2)
- MBR-STP Design Features PDFDocument7 pagesMBR-STP Design Features PDFManjunath HrmNo ratings yet
- EOA 2023 VISIOMER Portfolio Brochure en Digital RZ InteraktivDocument13 pagesEOA 2023 VISIOMER Portfolio Brochure en Digital RZ Interaktivichsan hakimNo ratings yet
- English Hand Out for Class 3Document19 pagesEnglish Hand Out for Class 3Pat WibawaNo ratings yet
- Swancor 901 Data SheetDocument2 pagesSwancor 901 Data SheetErin Guillermo33% (3)
- Katalog Baylan Vodomjer 1-2Document1 pageKatalog Baylan Vodomjer 1-2Edin Dervishi100% (1)
- WaterDocument2 pagesWaterLogan Marquez AguayoNo ratings yet
- Ben T. Zinn Combustion LaboratoryDocument2 pagesBen T. Zinn Combustion LaboratoryLeslie WilliamsNo ratings yet
- UK-India Coffee Market ReportDocument27 pagesUK-India Coffee Market ReportNikhil MunjalNo ratings yet
- Can You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsDocument3 pagesCan You Distinguish Neutral, Formal and Informal Among The Following Groups of WordsВікторія РудаNo ratings yet
- Presentation 1Document20 pagesPresentation 1anon_658550121No ratings yet
- ADAB Member List Provides Contact Details for Development OrganizationsDocument8 pagesADAB Member List Provides Contact Details for Development OrganizationsShipon GhoshNo ratings yet
- The Impact of ProstitutionDocument6 pagesThe Impact of ProstitutionLea TanNo ratings yet
- 17EEX01-FUNDAMENTALS OF FIBRE OPTICS AND LASER INSTRUMENTATION SyllabusDocument2 pages17EEX01-FUNDAMENTALS OF FIBRE OPTICS AND LASER INSTRUMENTATION SyllabusJayakumar ThangavelNo ratings yet