You might also like
- Pandemic Response and International Health Regulations: Short CommunicationDocument2 pagesPandemic Response and International Health Regulations: Short CommunicationdrdivishNo ratings yet
- COVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsFrom EverandCOVID-19 AFRICA, HAITI, AND THE U. S. VIRGIN ISLANDS:: The Response, the Aftermath, & Future ProjectionsNo ratings yet
- COVID 19 and International Health RegulationsDocument5 pagesCOVID 19 and International Health RegulationsMd. Abdullah RummanNo ratings yet
- Global Health Security and The International Health RegulationsDocument7 pagesGlobal Health Security and The International Health RegulationssarsulthaNo ratings yet
- World Health Organization: Is It Fit For Purpose?Document8 pagesWorld Health Organization: Is It Fit For Purpose?Toprak AkbaşNo ratings yet
- International Health Regulation (Ihr) : Yuri Nurdiantami, Apt., MPH Global Health Class UPN Veteran JakartaDocument22 pagesInternational Health Regulation (Ihr) : Yuri Nurdiantami, Apt., MPH Global Health Class UPN Veteran JakartaIzmi Azizah ZahraNo ratings yet
- CD Rom Ihr Optional Content IntroDocument7 pagesCD Rom Ihr Optional Content IntroTâm Nguyễn MinhNo ratings yet
- International Health RegulationDocument60 pagesInternational Health RegulationAnonymous 7ugfwjsHQUNo ratings yet
- ""We Must Stop The Global Epidemic of Chronic Disease."Document5 pages""We Must Stop The Global Epidemic of Chronic Disease."AmanNo ratings yet
- International Health Regulation (IHR) 2005: Unika Soegijapranata SemarangDocument32 pagesInternational Health Regulation (IHR) 2005: Unika Soegijapranata SemarangHari SantosoNo ratings yet
- World Health OrganizationDocument13 pagesWorld Health OrganizationVincent Ranara Sabornido100% (1)
- The Revised International Health Regulations and Restraint of National Health MeasuresDocument42 pagesThe Revised International Health Regulations and Restraint of National Health MeasuresSitiNo ratings yet
- MUN Topics For SLMUNDocument2 pagesMUN Topics For SLMUNthriyampakan dhivyakrishnanNo ratings yet
- World Health OrganızatıonDocument22 pagesWorld Health OrganızatıonKakashi 12No ratings yet
- International Health Regulations (IHR) - Division of Global Health Protection - Global Health - CDCDocument5 pagesInternational Health Regulations (IHR) - Division of Global Health Protection - Global Health - CDCObie BahhierNo ratings yet
- World Health Organization (WHO) : ObjectivesDocument9 pagesWorld Health Organization (WHO) : ObjectivesSAMAYAM KALYAN KUMARNo ratings yet
- History Project Rough DraftDocument11 pagesHistory Project Rough DraftDeep MalaniNo ratings yet
- World Health OrganizationDocument18 pagesWorld Health OrganizationsulyNo ratings yet
- World Health Organization (WHO)Document6 pagesWorld Health Organization (WHO)EllaNo ratings yet
- Pil RPDocument13 pagesPil RPgavileNo ratings yet
- Oms BookDocument292 pagesOms BookLUisNo ratings yet
- World Health Organization: Report by The Director-GeneralDocument9 pagesWorld Health Organization: Report by The Director-GeneralJaerose MuyongNo ratings yet
- Report - 7thEndTBSummitFor The HighestTBBurdenCountriesCountriesOnTheGlobal Watchlist - 16-17nov21Document38 pagesReport - 7thEndTBSummitFor The HighestTBBurdenCountriesCountriesOnTheGlobal Watchlist - 16-17nov21Charles SandyNo ratings yet
- World Health OrganizationDocument17 pagesWorld Health OrganizationRichi SinghNo ratings yet
- World Health Organisation's Help During The Pandemic History Project by PranayDocument28 pagesWorld Health Organisation's Help During The Pandemic History Project by Pranay;LDSKFJ ;No ratings yet
- 5 - GlobalizationDocument22 pages5 - GlobalizationDura EbrahimNo ratings yet
- COVID-19: An Overview of The Pandemic and Its Impact On Global HealthDocument2 pagesCOVID-19: An Overview of The Pandemic and Its Impact On Global HealthiwpNo ratings yet
- Committee: World Health Organization (WHO) Topic: Infection Prevention and Control of Future Pandemics Delegation: GreeceDocument2 pagesCommittee: World Health Organization (WHO) Topic: Infection Prevention and Control of Future Pandemics Delegation: GreeceEvelynNo ratings yet
- Strengthening The International Health Regulations: Lessons From The H1N1 PandemicDocument5 pagesStrengthening The International Health Regulations: Lessons From The H1N1 PandemicnddyNo ratings yet
- Report On Covid-19: ShivamDocument5 pagesReport On Covid-19: ShivamTarun NarayanNo ratings yet
- Tori Robbins Research Paper SubmissionDocument40 pagesTori Robbins Research Paper Submissionapi-529132931No ratings yet
- World Health Organization PDFDocument32 pagesWorld Health Organization PDFBob LablaNo ratings yet
- Ir AssignmentDocument6 pagesIr AssignmentvannesaNo ratings yet
- Age of PandemicDocument12 pagesAge of PandemicDavide FalcioniNo ratings yet
- International HealthDocument110 pagesInternational HealthHiren patelNo ratings yet
- Global Pandemics and Human Security - Docx Research Article 2Document14 pagesGlobal Pandemics and Human Security - Docx Research Article 2quratNo ratings yet
- Globalisation& PublichealthDocument102 pagesGlobalisation& Publichealthujangketul62No ratings yet
- WHO 1991 128 PagesDocument136 pagesWHO 1991 128 PagesLilmariusNo ratings yet
- Contributions of WhoDocument6 pagesContributions of WhoRahilNo ratings yet
- Epih 42 E2020013Document4 pagesEpih 42 E2020013Maria PopescuNo ratings yet
- Who HungaryDocument2 pagesWho HungaryDiva CarissaNo ratings yet
- The Invisible Enemy - COVID-19Document6 pagesThe Invisible Enemy - COVID-19Eren MERICNo ratings yet
- What Is The World Doing in Order To Prevent Humans From Turning Into Zombies? A Theoritical Framework For Global Pandemic ResponseDocument4 pagesWhat Is The World Doing in Order To Prevent Humans From Turning Into Zombies? A Theoritical Framework For Global Pandemic Responseneo paulNo ratings yet
- (26662531 - Yearbook of International Disaster Law Online) International Health Law (2020)Document14 pages(26662531 - Yearbook of International Disaster Law Online) International Health Law (2020)Karla Monique PadrelananNo ratings yet
- The Outbreak of COVID-19 Coronavirus Are The International Health Regulations Fit For PurposeDocument7 pagesThe Outbreak of COVID-19 Coronavirus Are The International Health Regulations Fit For PurposecitizenNo ratings yet
- United OdtDocument2 pagesUnited OdtsumitNo ratings yet
- The United Nations and Global HealthDocument26 pagesThe United Nations and Global HealthIoan VoicuNo ratings yet
- Draft ResolutionDocument6 pagesDraft Resolutionsuvendu shekhar MahakudNo ratings yet
- WHODocument17 pagesWHOMrutunjay PatraNo ratings yet
- A History of Global HealthDocument5 pagesA History of Global HealthJorge Luis MendezNo ratings yet
- DocumentDocument4 pagesDocumenttangaramariam566No ratings yet
- International Narcotics Control Board: United NationsDocument121 pagesInternational Narcotics Control Board: United NationsDudu RibeiroNo ratings yet
- Epidemiology - COVID-19RebeccacgDocument10 pagesEpidemiology - COVID-19RebeccacgIheakachi IheakachiNo ratings yet
- STS ResearchDocument27 pagesSTS ResearchArlyn NaritoNo ratings yet
- Global Surveillance of Communicable Diseases: Special IssueDocument4 pagesGlobal Surveillance of Communicable Diseases: Special IssueMuhammad Hafiidh MuizzNo ratings yet
- Interim Minority Report On The Origins of The COVID 19 Global Pandemic Including The Roles of The CCP and WHO 6.15.20Document50 pagesInterim Minority Report On The Origins of The COVID 19 Global Pandemic Including The Roles of The CCP and WHO 6.15.20Kristina WongNo ratings yet
- Study Guide - Who - Mun Simulation 1.0Document6 pagesStudy Guide - Who - Mun Simulation 1.019O2OO513 Dava PebrianNo ratings yet
- House GOP - Coronavirus and China - Interim ReportDocument50 pagesHouse GOP - Coronavirus and China - Interim ReportJenna RomaineNo ratings yet
- International Conventions One HealthDocument3 pagesInternational Conventions One HealthLauren PremNo ratings yet
- Medical CertificateDocument3 pagesMedical CertificateSñëhå PàlNo ratings yet
- Article On Athletes Coping InjuryDocument2 pagesArticle On Athletes Coping InjuryAnna Marie L. MalulanNo ratings yet
- 04 Format Manual UpdatedDocument83 pages04 Format Manual UpdatedBurhan Wagh WaghNo ratings yet
- The Procedure: Cleaning ValidationDocument4 pagesThe Procedure: Cleaning ValidationYousif100% (1)
- Declaration Form For Split StaysDocument1 pageDeclaration Form For Split StaysMohit BhavnagariNo ratings yet
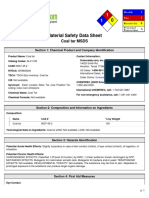
- Msds Coal PDFDocument5 pagesMsds Coal PDFWinaNo ratings yet
- Case Studies On CoagulationDocument3 pagesCase Studies On CoagulationGerald John PazNo ratings yet
- Mangu High School Trial 2 Mocks 2021: Kenya Certificate of Secondary Education (KCSE)Document7 pagesMangu High School Trial 2 Mocks 2021: Kenya Certificate of Secondary Education (KCSE)princewNo ratings yet
- Edu 422 NotesDocument13 pagesEdu 422 NotesAbdulazeez AishatNo ratings yet
- Daily Dose of Sunshine Case StudyDocument2 pagesDaily Dose of Sunshine Case Studyvon aliparNo ratings yet
- Vaccine Wastage Study in Ghana, Mozambique and PakistanDocument12 pagesVaccine Wastage Study in Ghana, Mozambique and PakistanYee Theng NgNo ratings yet
- Las Pe10 Day1 Week1 DonnaDocument4 pagesLas Pe10 Day1 Week1 DonnaBadeth AblaoNo ratings yet
- Dhumapana in Science VisionDocument3 pagesDhumapana in Science Visionmanchak1No ratings yet
- PP Amicus Brief - 5th CircuitDocument17 pagesPP Amicus Brief - 5th CircuitAlanna JeanNo ratings yet
- Computer-Assisted Osteotomy Guides and Pre-Bent Titanium Plates Improve The Planning For Correction of Facial AsymmetryDocument34 pagesComputer-Assisted Osteotomy Guides and Pre-Bent Titanium Plates Improve The Planning For Correction of Facial AsymmetrySantos TicaNo ratings yet
- Ebook Benzels Spine Surgery 2 Volume Set Techniques Complication Avoidance and Management PDF Full Chapter PDFDocument67 pagesEbook Benzels Spine Surgery 2 Volume Set Techniques Complication Avoidance and Management PDF Full Chapter PDFgerald.wesolowski623100% (22)
- FPM - Capstone Project - FinalDocument28 pagesFPM - Capstone Project - FinalVijayendra SinghNo ratings yet
- Sub 25 - Willson Consulting - Attach 2 - RedactedDocument61 pagesSub 25 - Willson Consulting - Attach 2 - Redactedlex lutorNo ratings yet
- Microbiology of Concentrated MilkDocument30 pagesMicrobiology of Concentrated MilkNitric AcidNo ratings yet
- Socio-Cultural Factors in FamilyDocument21 pagesSocio-Cultural Factors in FamilyGangadhar DungaNo ratings yet
- Medicolegal Aspects of Hurt Injury and WoundDocument6 pagesMedicolegal Aspects of Hurt Injury and WoundSebin JamesNo ratings yet
- Natural History of Disease FINALDocument13 pagesNatural History of Disease FINALnadia nisarNo ratings yet
- Course Learning Packets Template Saint Louis University School of Teacher Education and Liberal ArtsDocument8 pagesCourse Learning Packets Template Saint Louis University School of Teacher Education and Liberal ArtsUchayyaNo ratings yet
- All About NailsDocument16 pagesAll About NailsJoel MarasiganNo ratings yet
- How The Special Needs Brain Learns,: Chapter-By-Chapter Study Guide ForDocument2 pagesHow The Special Needs Brain Learns,: Chapter-By-Chapter Study Guide ForElizabeth Clarissa Palar - NainggolanNo ratings yet
- Anueurism Cure NaturalDocument3 pagesAnueurism Cure NaturalbillNo ratings yet
- PR2 Mod 1Document60 pagesPR2 Mod 1Jan Loven Del RosarioNo ratings yet
- Management of LabourDocument38 pagesManagement of LabourAnjali Rahul AjmeriNo ratings yet
- Gallium-67 (Ga) : Physical DataDocument3 pagesGallium-67 (Ga) : Physical DataCarlos CadavidNo ratings yet
- The Impact of Exercise Therapy and Abdominal Binding in The Management of Diastasis Recti Abdominis in The Early Post-Partum Period: A Pilot Randomized Controlled TrialDocument17 pagesThe Impact of Exercise Therapy and Abdominal Binding in The Management of Diastasis Recti Abdominis in The Early Post-Partum Period: A Pilot Randomized Controlled TrialSara EmmanuelaNo ratings yet