You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Self-Perception Profile For LD StudentsDocument67 pagesSelf-Perception Profile For LD StudentsCátia Alexandra CorreiaNo ratings yet
- Science Current Directions in PsychologicalDocument7 pagesScience Current Directions in PsychologicalCátia Alexandra CorreiaNo ratings yet
- Literature Review: Using Elements of Hypnosis Prior To or During Pediatric Dental TreatmentDocument4 pagesLiterature Review: Using Elements of Hypnosis Prior To or During Pediatric Dental TreatmentCátia Alexandra CorreiaNo ratings yet
- 1471 2458 10 499Document15 pages1471 2458 10 499Cátia Alexandra CorreiaNo ratings yet
- International Journal of Clinical and Experimental HypnosisDocument15 pagesInternational Journal of Clinical and Experimental HypnosisCátia Alexandra CorreiaNo ratings yet
- A Type A and Type D PersonalityDocument29 pagesA Type A and Type D PersonalityCátia Alexandra CorreiaNo ratings yet
- The Final Research PaperDocument47 pagesThe Final Research Paperapi-402790311No ratings yet
- Pcon Ca (Me0289 7i)Document300 pagesPcon Ca (Me0289 7i)HermanTo0% (1)
- Gray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full ChapterDocument51 pagesGray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full Chaptereugene.poremski145100% (5)
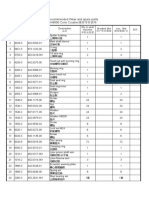
- Recommended Wear and spare parts H8800 Cone Crusher推荐零件清单Document3 pagesRecommended Wear and spare parts H8800 Cone Crusher推荐零件清单Lmf DanielNo ratings yet
- p385 90Document35 pagesp385 90Edward MacDermidNo ratings yet
- Dr. Ahmed Shafai P6Document13 pagesDr. Ahmed Shafai P6Haya ZayedNo ratings yet
- Niral Network ProductsDocument7 pagesNiral Network ProductsNiral NetworksNo ratings yet
- Electrostatic - 1Document3 pagesElectrostatic - 1AnjuNo ratings yet
- Substance Abuse and Psychiatric: Disordersin Prison InmatesDocument3 pagesSubstance Abuse and Psychiatric: Disordersin Prison InmatesNorberth Ioan OkrosNo ratings yet
- Times Leader 06-04-2013Document32 pagesTimes Leader 06-04-2013The Times LeaderNo ratings yet
- Canada Drugs Direct PAFDocument1 pageCanada Drugs Direct PAFrjohngdcNo ratings yet
- Datasheet Nastra Uk 1.01 01Document1 pageDatasheet Nastra Uk 1.01 01Ahmed EbhaireNo ratings yet
- Reaction To EJKDocument9 pagesReaction To EJKKevin DawangNo ratings yet
- Sikafiber® Novocon® He-1050 HT: Product Data SheetDocument3 pagesSikafiber® Novocon® He-1050 HT: Product Data SheetCsillag JanosNo ratings yet
- Principles of ChromatographyDocument8 pagesPrinciples of ChromatographylordniklausNo ratings yet
- Sensory EssentialsDocument8 pagesSensory Essentialsbaji sharifNo ratings yet
- Chlamydia InfectionsDocument4 pagesChlamydia InfectionsPearl CalisNo ratings yet
- MAN Marine Auxiliary Engines 2018 1Document1 pageMAN Marine Auxiliary Engines 2018 1Tudor AgheorghieseiNo ratings yet
- Science: Quarter 1 - Module 2 Lesson 3: Changes in Matter and Its Effect in The EnvironmentDocument20 pagesScience: Quarter 1 - Module 2 Lesson 3: Changes in Matter and Its Effect in The EnvironmentTEAM KnightzNo ratings yet
- Direct Look Versus Evasive Glance and Compliance With A RequestDocument4 pagesDirect Look Versus Evasive Glance and Compliance With A RequestPublia PromenadeNo ratings yet
- Mammomat Revelation Product Brochure-2018!01!04848077Document16 pagesMammomat Revelation Product Brochure-2018!01!04848077Ngọc Hoàng TuấnNo ratings yet
- The Central Pollution Control BoardDocument7 pagesThe Central Pollution Control BoardGanapati Joshi SankolliNo ratings yet
- Case Study AmulDocument6 pagesCase Study AmulTales Of TanviNo ratings yet
- Covenant On Civil and Political RightsDocument3 pagesCovenant On Civil and Political RightsRainier Rhett ConchaNo ratings yet
- Biochemistry - Lipid ProfileDocument1 pageBiochemistry - Lipid ProfileHassan RazaNo ratings yet
- EDANA Guidelines For Testing Feminine Hygiene Products: December 2018Document21 pagesEDANA Guidelines For Testing Feminine Hygiene Products: December 2018Kinga B.No ratings yet
- Soap Note-Heidi Martinez PedsDocument6 pagesSoap Note-Heidi Martinez PedsHeidi Martinez100% (2)
- Molusco ContagiosoDocument12 pagesMolusco ContagiosoEduardo Medeiros Tabosa PinheiroNo ratings yet
- Problem Identification - Illuminate EducationDocument6 pagesProblem Identification - Illuminate Educationhailemecaile kfileNo ratings yet
- 12 Hvac Design Guide For High Rise Tall BuildingsDocument94 pages12 Hvac Design Guide For High Rise Tall BuildingsjendrikoNo ratings yet