You might also like
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- HydroceleDocument10 pagesHydroceleRyan ReNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- NCP PediatricDocument5 pagesNCP PediatricSL Hanna NebridaNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Nursing Care Plan NCPDocument24 pagesNursing Care Plan NCPRosemarie R. Reyes100% (1)
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- Managing Overweight through Diet and ExerciseDocument17 pagesManaging Overweight through Diet and ExerciseMarie Ashley CasiaNo ratings yet
- CASE STUDY PPT Group1 - Revised WithoutvideoDocument34 pagesCASE STUDY PPT Group1 - Revised WithoutvideoSamantha BolanteNo ratings yet
- C. Case Study thesis-NCP (Revised)Document5 pagesC. Case Study thesis-NCP (Revised)Lopirts NiganiNo ratings yet
- Epigastric Pain Case StudyDocument19 pagesEpigastric Pain Case StudyYana PotNo ratings yet
- Subjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Document5 pagesSubjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Erle Gray CadangenNo ratings yet
- ASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONDocument4 pagesASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONArian May Marcos100% (1)
- CHAPTER 5 Nursing Care PlanDocument5 pagesCHAPTER 5 Nursing Care PlanMiguelito Galagar GultianoNo ratings yet
- Nursing Care Plans for Fluid Volume and Fatigue ManagementDocument4 pagesNursing Care Plans for Fluid Volume and Fatigue ManagementGILIANNE MARIE JIMENEANo ratings yet
- Abruptio PlacentaDocument6 pagesAbruptio PlacentaBb RabbitNo ratings yet
- Nursing Care PlanDocument12 pagesNursing Care Plankeishaaa29100% (6)
- Case Study 5Document6 pagesCase Study 5Anthony jesusNo ratings yet
- NCP Post PartumDocument2 pagesNCP Post PartumsteffiNo ratings yet
- Sickle Cell - RahafDocument39 pagesSickle Cell - RahafgalalNo ratings yet
- Nursing Care PlanDocument11 pagesNursing Care PlanKirstin del CarmenNo ratings yet
- Gestational Diabetes - Case Study 2Document13 pagesGestational Diabetes - Case Study 2Bb RabbitNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationpamelaideaNo ratings yet
- Nursing Care Plan for a Client with Intestinal ObstructionDocument4 pagesNursing Care Plan for a Client with Intestinal ObstructionRenea Joy ArruejoNo ratings yet
- Medical Management Include Drug Therapy: Hydatidiform MoleDocument2 pagesMedical Management Include Drug Therapy: Hydatidiform MoleMaye ArugayNo ratings yet
- Threatened Abortion - Edited 1Document55 pagesThreatened Abortion - Edited 1اكينو ستيفاني100% (1)
- Fluid Volume Defict Ms. HicksDocument8 pagesFluid Volume Defict Ms. HicksShenna RegaspiNo ratings yet
- Hainashri MSN ProcedureDocument9 pagesHainashri MSN ProcedureRickjit SadhukhanNo ratings yet
- Waiters PATIENT CARE PLAN 2020 For PPHDocument3 pagesWaiters PATIENT CARE PLAN 2020 For PPHmp1757No ratings yet
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- Helping a Patient Manage Nausea and VomitingDocument3 pagesHelping a Patient Manage Nausea and VomitingJakeNo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitRainier IbarretaNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPjsksNo ratings yet
- Nursing Care Plan for Postpartum HemorrhageDocument4 pagesNursing Care Plan for Postpartum HemorrhageEvangeline Anne MacanasNo ratings yet
- NCP Case Analysis GastritisDocument7 pagesNCP Case Analysis GastritisSteffi GolezNo ratings yet
- NCP - AgeDocument5 pagesNCP - Ageunsp3akabl386% (7)
- Gonzaga Rlems - NCPDocument3 pagesGonzaga Rlems - NCPShaynne Wencille A. GONZAGANo ratings yet
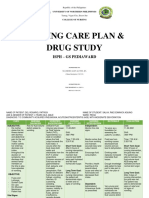
- Salva, R.D NCP & Drug Study (Isph - Gs Pediaward)Document7 pagesSalva, R.D NCP & Drug Study (Isph - Gs Pediaward)Rae Dominick Aquino SalvaNo ratings yet
- Campugan, Jay NCP PT 14-08-2023Document8 pagesCampugan, Jay NCP PT 14-08-2023Flower Flower FlowerNo ratings yet
- Group-5 NCM-107 NCPDocument4 pagesGroup-5 NCM-107 NCPbulok netflakes100% (1)
- Guinitaran, Christine Ann P. BSN 4 Abruptio Placenta Nursing Care PlanDocument19 pagesGuinitaran, Christine Ann P. BSN 4 Abruptio Placenta Nursing Care PlanGemmalene PaclebNo ratings yet
- Abruptio Placenta NCP 2 FinalDocument19 pagesAbruptio Placenta NCP 2 FinalTin100% (1)
- Hepatitis A N C P BY BHERU LALDocument2 pagesHepatitis A N C P BY BHERU LALBheru LalNo ratings yet
- Pregnancy Induced HypertensionDocument67 pagesPregnancy Induced HypertensionTrisha OrtegaNo ratings yet
- Set 1 PDFDocument62 pagesSet 1 PDFAlyssa MontimorNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Nle BulletsDocument53 pagesNle BulletsdjhemzNo ratings yet
- Case Plan On Diarrhoea (Medical Surgical Nursing)Document15 pagesCase Plan On Diarrhoea (Medical Surgical Nursing)kamini ChoudharyNo ratings yet
- Clinical Case Study - Online Discussion Form Fall 2020-1Document14 pagesClinical Case Study - Online Discussion Form Fall 2020-1Sabrina Odies100% (1)
- Renal Failure NCPDocument3 pagesRenal Failure NCPJet Ray-Ann GaringanNo ratings yet
- Nursing Care PlansDocument31 pagesNursing Care PlansCyril Jane Caanyagan AcutNo ratings yet
- Case Study #1 (NCM116RC)Document4 pagesCase Study #1 (NCM116RC)Dexel Lorren ValdezNo ratings yet
- Care Plan Number 2Document5 pagesCare Plan Number 2Teddy mc Bones100% (1)
- Nursing Care Plan for UTIDocument3 pagesNursing Care Plan for UTIAl TheóNo ratings yet
- Capacio Case#1 RevisedDocument4 pagesCapacio Case#1 RevisedLorenz CapacioNo ratings yet
- Risk NCP - PESCADERO 4CDocument1 pageRisk NCP - PESCADERO 4COrlando VillanuevaNo ratings yet
- Assessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationDocument10 pagesAssessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationApol Pen67% (3)
- MS Soapie #1Document2 pagesMS Soapie #1Fatima KateNo ratings yet
- Homework Activity-2 NUR-102 MODULE6-7-8Document3 pagesHomework Activity-2 NUR-102 MODULE6-7-8Duchess Juliane Jose MirambelNo ratings yet
- Nur-102 Laboratory Homework Activity-2 Module 6-7 and 8Document4 pagesNur-102 Laboratory Homework Activity-2 Module 6-7 and 8Duchess Juliane Jose MirambelNo ratings yet
- Hygiene NotesDocument60 pagesHygiene NotesDuchess Juliane Jose MirambelNo ratings yet
- Module 6-7Document2 pagesModule 6-7Duchess Juliane Jose MirambelNo ratings yet
- Activity Module - 17 and 18 Essay Question and AnswerDocument2 pagesActivity Module - 17 and 18 Essay Question and AnswerDuchess Juliane Jose MirambelNo ratings yet
- SHAMPOOING HAIR IN BED: 27-STEP PROCEDUREDocument3 pagesSHAMPOOING HAIR IN BED: 27-STEP PROCEDUREDuchess Juliane Jose MirambelNo ratings yet
- Data Analysis and InterpretationDocument12 pagesData Analysis and InterpretationDuchess Juliane Jose MirambelNo ratings yet
- Volleyball (Women) Workout Plan: Warm UpDocument1 pageVolleyball (Women) Workout Plan: Warm UpDuchess Juliane Jose MirambelNo ratings yet
- Hygiene NotesDocument60 pagesHygiene NotesDuchess Juliane Jose MirambelNo ratings yet
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Document2 pagesSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Duchess Juliane Jose MirambelNo ratings yet
- First Week Workout PlanDocument2 pagesFirst Week Workout PlanDuchess Juliane Jose MirambelNo ratings yet
- Lto Written Test On Driving: LTO Driver's License Exam ReviewerDocument22 pagesLto Written Test On Driving: LTO Driver's License Exam ReviewerDuchess Juliane Jose MirambelNo ratings yet
- Primary Skin Lesion Types and DescriptionsDocument6 pagesPrimary Skin Lesion Types and DescriptionsDuchess Juliane Jose MirambelNo ratings yet
- Drug Name Classification Mechanism of Action Indication Contraindication Nursing Responsibilities Generic Name CVDocument3 pagesDrug Name Classification Mechanism of Action Indication Contraindication Nursing Responsibilities Generic Name CVDuchess Juliane Jose MirambelNo ratings yet
- A CHAPTER 4Document11 pagesA CHAPTER 4Duchess Juliane Jose MirambelNo ratings yet
- SDL 3Document2 pagesSDL 3Duchess Juliane Jose MirambelNo ratings yet
- DedicationDocument5 pagesDedicationDuchess Juliane Jose MirambelNo ratings yet
- School of Health and Allied Health Sciences Nursing DepartmentDocument2 pagesSchool of Health and Allied Health Sciences Nursing DepartmentDuchess Juliane Jose MirambelNo ratings yet
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Document3 pagesSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Duchess Juliane Jose MirambelNo ratings yet
- Fetal Deaths: by AttendanceDocument3 pagesFetal Deaths: by AttendanceDuchess Juliane Jose MirambelNo ratings yet
- Self-Directed Learning (Nur 146 - Clinical Area)Document2 pagesSelf-Directed Learning (Nur 146 - Clinical Area)Duchess Juliane Jose MirambelNo ratings yet
- COLLAGEDocument1 pageCOLLAGEDuchess Juliane Jose MirambelNo ratings yet
- SDL 1Document2 pagesSDL 1Duchess Juliane Jose MirambelNo ratings yet
- Module 58Document2 pagesModule 58Duchess Juliane Jose MirambelNo ratings yet
- V Kinematic Viscosity: F F F 2 F N 2 NDocument4 pagesV Kinematic Viscosity: F F F 2 F N 2 NDuchess Juliane Jose Mirambel0% (1)
- Module 20 Hook Activity Hormones Functions 1. Hormones of ThyroidDocument2 pagesModule 20 Hook Activity Hormones Functions 1. Hormones of ThyroidDuchess Juliane Jose MirambelNo ratings yet
- Research in Community Health Nursing Part Ii: Answer RationaleDocument1 pageResearch in Community Health Nursing Part Ii: Answer RationaleDuchess Juliane Jose MirambelNo ratings yet
- Shampooing Hair in BedDocument2 pagesShampooing Hair in BedDuchess Juliane Jose Mirambel100% (1)
- Physiological Changes in Aging Affecting The Urinary System: Check For Understanding Answer RationaleDocument1 pagePhysiological Changes in Aging Affecting The Urinary System: Check For Understanding Answer RationaleDuchess Juliane Jose MirambelNo ratings yet
- Sexual SelfDocument24 pagesSexual SelfLady of the Light100% (1)
- The BAR - Philippine Digested Cases - Landmark Case - RH BILL CASE - Imbong Vs Ochoa Et - Al. G.R. No. 204819 April 8, 2014 (Digested Case)Document8 pagesThe BAR - Philippine Digested Cases - Landmark Case - RH BILL CASE - Imbong Vs Ochoa Et - Al. G.R. No. 204819 April 8, 2014 (Digested Case)Patronus GoldenNo ratings yet
- Radio Production Manual - Edited and FormattedDocument152 pagesRadio Production Manual - Edited and FormattedMushtaq Muhammad100% (1)
- NCERT Solution For CBSE Class 10 Science Chapter 8 How Do Organisms ReproduceDocument5 pagesNCERT Solution For CBSE Class 10 Science Chapter 8 How Do Organisms ReproduceAmbarish ParikiNo ratings yet
- CP-PHC 1 Removal ExamDocument6 pagesCP-PHC 1 Removal ExamJuana I. Dela Cruz100% (1)
- Ethnocultural InfluencesDocument17 pagesEthnocultural Influencesmuwaag musaNo ratings yet
- Population and Its Control by Kailash NagarDocument69 pagesPopulation and Its Control by Kailash NagarKailash NagarNo ratings yet
- UNDS111 Midterm ReviewerDocument18 pagesUNDS111 Midterm ReviewerJULIANA NICOLE TUIBUENNo ratings yet
- Drug Dosage FormsDocument56 pagesDrug Dosage FormsHamid HamidNo ratings yet
- 2020 National Health Goals Related To Reproductive and Sexual Health.Document2 pages2020 National Health Goals Related To Reproductive and Sexual Health.KHRISTINE KAYE SALUDESNo ratings yet
- Army Public School Gopalpur: Class-Xii Science Subject - Biology Chapter-4 Reproductive Health NotesDocument5 pagesArmy Public School Gopalpur: Class-Xii Science Subject - Biology Chapter-4 Reproductive Health NotesAshok KumarNo ratings yet
- Birth Control Pill Factsheet - ADocument2 pagesBirth Control Pill Factsheet - AkaybeeNo ratings yet
- Wa0033Document10 pagesWa0033Obrian RobinsonNo ratings yet
- IRR RA 10354 RH LawDocument81 pagesIRR RA 10354 RH LawCBCP for LifeNo ratings yet
- RESEARCH PROJECT-2014 (RUNYANGA TENDERANO-BSNS-Zimbabwe Open University-Empowerment Through Open Learning)Document94 pagesRESEARCH PROJECT-2014 (RUNYANGA TENDERANO-BSNS-Zimbabwe Open University-Empowerment Through Open Learning)Tenderano Runyanga100% (1)
- Alliance vs. Garin 2017Document23 pagesAlliance vs. Garin 2017shirlyn cuyongNo ratings yet
- Clinical Obstetrics and Gynecology Volume 50, Number 4, 898–906 r 2007, Lippincott Williams & Wilkins Injectable ContraceptionDocument9 pagesClinical Obstetrics and Gynecology Volume 50, Number 4, 898–906 r 2007, Lippincott Williams & Wilkins Injectable ContraceptionCarlosCorderoLópezNo ratings yet
- Contraception Questions and Answers For PharmacistsDocument9 pagesContraception Questions and Answers For PharmacistsMohamed OmerNo ratings yet
- ZgureanuDocument4 pagesZgureanuVictoria OpincaNo ratings yet
- 1975 Jan-Feb #62Document28 pages1975 Jan-Feb #62Merlin ChowkwanyunNo ratings yet
- Report On AbortionDocument5 pagesReport On AbortionMarc Edward TillNo ratings yet
- Eliminating Teenage Pregnancy in The Philippines: Policy BriefDocument6 pagesEliminating Teenage Pregnancy in The Philippines: Policy BriefMari LeianaNo ratings yet
- Factors Influencing Family Planning Uptake Among Women of Reproductive Age in The Sefwi Akontombra District of Western North Region, GhanaDocument25 pagesFactors Influencing Family Planning Uptake Among Women of Reproductive Age in The Sefwi Akontombra District of Western North Region, GhanaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Maternity and Pediatric Nursing 3rd EditionDocument347 pagesMaternity and Pediatric Nursing 3rd EditionTaylor Talley80% (15)
- Causes of Teenage PregnancyDocument4 pagesCauses of Teenage Pregnancycreate foxesNo ratings yet
- The Impact of Multimedia Family Planning Promotion On The Contraceptive Behavior of Women in TanzaniaDocument9 pagesThe Impact of Multimedia Family Planning Promotion On The Contraceptive Behavior of Women in TanzaniaParag DhobleNo ratings yet
- FSRH Guidance Switching or Starting Methods of Contraception August 2019Document10 pagesFSRH Guidance Switching or Starting Methods of Contraception August 2019Ting Yiu WongNo ratings yet
- 12 Body Mapping in Health RRA/PRA: Andrea CornwallDocument7 pages12 Body Mapping in Health RRA/PRA: Andrea CornwallNurusNo ratings yet
- Contraception UpdateDocument24 pagesContraception UpdatePSmNo ratings yet
- DOHS ReportDocument489 pagesDOHS ReportDivya TiwariNo ratings yet