You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Time and Memory)Document340 pagesTime and Memory)gustavoalbertomaseraNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Depressive DisoredersDocument125 pagesDepressive DisoredersAbelNo ratings yet
- Obstetrics & GynecologyDocument10 pagesObstetrics & GynecologyRaul DoctoNo ratings yet
- Depression As An Evolutionary Strategy For Defense Against InfectionDocument14 pagesDepression As An Evolutionary Strategy For Defense Against InfectionOscar Alejandro Cardenas Quintero100% (2)
- 8 Physio OB - Physiology of Labor I - IIDocument14 pages8 Physio OB - Physiology of Labor I - IIArnoldBorromeoNo ratings yet
- Lecture 1: NeuroembryologyDocument13 pagesLecture 1: NeuroembryologyRaul Docto100% (1)
- HIGH HISTAMINE - LOW HEALTH - Brainstorm HealthDocument1 pageHIGH HISTAMINE - LOW HEALTH - Brainstorm HealthRodrigo FerreiraNo ratings yet
- Drugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Document467 pagesDrugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Marc Imhotep Cray, M.D.100% (1)
- Presented By:: Mr. Vinay Kumar M.Sc. Nursing 1 Year HCN, SrhuDocument44 pagesPresented By:: Mr. Vinay Kumar M.Sc. Nursing 1 Year HCN, SrhuVinay KumarNo ratings yet
- BMW 6 Cylinder Dual Vanos Piston Seal Repair Fix PDocument13 pagesBMW 6 Cylinder Dual Vanos Piston Seal Repair Fix PRaul DoctoNo ratings yet
- 1998 Volvo s70-v70Document52 pages1998 Volvo s70-v70Raul DoctoNo ratings yet
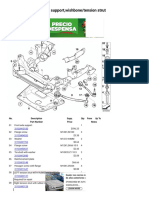
- X3 E83 X3 3.0i FRNT Axle Support, Wishbone Tension StrutDocument3 pagesX3 E83 X3 3.0i FRNT Axle Support, Wishbone Tension StrutRaul DoctoNo ratings yet
- Central Venous Pressure (CVP)Document3 pagesCentral Venous Pressure (CVP)Raul DoctoNo ratings yet
- An Update On COVID-19 and Pregnancy: Djamieson@emory - EduDocument10 pagesAn Update On COVID-19 and Pregnancy: Djamieson@emory - EduRaul DoctoNo ratings yet
- Why Exercise Builds Muscles: Titin Mechanosensing Controls Skeletal Muscle Growth Under LoadDocument15 pagesWhy Exercise Builds Muscles: Titin Mechanosensing Controls Skeletal Muscle Growth Under LoadRaul Docto100% (1)
- Seminar: Jan Claassen, Soojin ParkDocument17 pagesSeminar: Jan Claassen, Soojin ParkRaul DoctoNo ratings yet
- 2022 ACC A-Ha HFSAGuideline For The Management of Heart FailureDocument167 pages2022 ACC A-Ha HFSAGuideline For The Management of Heart FailureRaul DoctoNo ratings yet
- Ascoping Review of The Pathophysiology of COVID-19Document16 pagesAscoping Review of The Pathophysiology of COVID-19Raul DoctoNo ratings yet
- Case 35-2021: A 50-Year-Old Woman With Pain in The Left Upper Quadrant and HypoxemiaDocument7 pagesCase 35-2021: A 50-Year-Old Woman With Pain in The Left Upper Quadrant and HypoxemiaRaul DoctoNo ratings yet
- How To Install Google Play On The Amazon Fire HD 8Document7 pagesHow To Install Google Play On The Amazon Fire HD 8Raul DoctoNo ratings yet
- Tugwell 1985Document13 pagesTugwell 1985Raul DoctoNo ratings yet
- 007 Obgyn-CatalogDocument100 pages007 Obgyn-CatalogRaul DoctoNo ratings yet
- Vlaar2021 Article TransfusionStrategiesInBleedinDocument25 pagesVlaar2021 Article TransfusionStrategiesInBleedinRaul DoctoNo ratings yet
- Human Infection With Strongyloides Stercoralis and Other Related Strongyloides SpeciesDocument11 pagesHuman Infection With Strongyloides Stercoralis and Other Related Strongyloides SpeciesRaul DoctoNo ratings yet
- Ventilator Weaning and Spontaneous Breathing Trials An Educational ReviewDocument7 pagesVentilator Weaning and Spontaneous Breathing Trials An Educational ReviewRaul DoctoNo ratings yet
- Heparin Resistance - Clinical Perspectives and Management StrategiesDocument7 pagesHeparin Resistance - Clinical Perspectives and Management StrategiesRaul DoctoNo ratings yet
- Author 'S Accepted ManuscriptDocument46 pagesAuthor 'S Accepted ManuscriptRaul DoctoNo ratings yet
- Prolonged Pregnancy:When Should We Intervene?Document11 pagesProlonged Pregnancy:When Should We Intervene?Raul DoctoNo ratings yet
- Endocrinology Test ReviewDocument5 pagesEndocrinology Test ReviewHermela GhebremichaelNo ratings yet
- Metabolic Response To StressDocument8 pagesMetabolic Response To StressFatima Zahara100% (1)
- PHYL2001 - Tony's Final Tutorial Questions - 2021 FinalDocument32 pagesPHYL2001 - Tony's Final Tutorial Questions - 2021 FinalAlisha Rodrigo100% (1)
- The Maternal BrainDocument358 pagesThe Maternal BrainCarlos VargasNo ratings yet
- The Slings and Arrows of Daily LifeDocument17 pagesThe Slings and Arrows of Daily Lifeneurogenics_18570782No ratings yet
- Chapter 28 PROMDocument24 pagesChapter 28 PROMTansya PurnaningrumNo ratings yet
- Affective DisordersDocument37 pagesAffective Disordersveronicaine91No ratings yet
- Substanceabuseand Trauma: Shannon Simmons,, Liza SuárezDocument12 pagesSubstanceabuseand Trauma: Shannon Simmons,, Liza SuárezEma UrzicaNo ratings yet
- EBOOK 978 0123750976 Handbook of Neuroendocrinology Download Full Chapter PDF KindleDocument61 pagesEBOOK 978 0123750976 Handbook of Neuroendocrinology Download Full Chapter PDF Kindlejuan.speight804100% (44)
- Maternal-Fetal Circadian Communication During PregnancyDocument9 pagesMaternal-Fetal Circadian Communication During PregnancyLeslie AcevesNo ratings yet
- Síndrome Del Intestino Irritable (Caso 1.9)Document10 pagesSíndrome Del Intestino Irritable (Caso 1.9)xixiNo ratings yet
- Congenital Adrenal HyperplasiaDocument13 pagesCongenital Adrenal Hyperplasiaashgee1No ratings yet
- Desmopressin (DDAVP) Stimulation Test - UpToDateDocument13 pagesDesmopressin (DDAVP) Stimulation Test - UpToDateMihaela Alexandra RepeziNo ratings yet
- Endocrinology Lecture 2012Document232 pagesEndocrinology Lecture 2012Takacs CsabaNo ratings yet
- Pengaruh Terapi Dzikir Terhadap Intensitas Nyeri Pada Pasien GastritisDocument5 pagesPengaruh Terapi Dzikir Terhadap Intensitas Nyeri Pada Pasien GastritisRahmidamiliyntNo ratings yet
- Frontiers in Neuroendocrinology: SciencedirectDocument15 pagesFrontiers in Neuroendocrinology: SciencedirectFrancisco Javier Luza RamosNo ratings yet
- Postpartum Depression Current Identification BiomarkersDocument16 pagesPostpartum Depression Current Identification Biomarkersolyvia lenseNo ratings yet
- StressDocument11 pagesStressnurjamima96No ratings yet
- Group D Case Study Cushing SyndromeDocument6 pagesGroup D Case Study Cushing SyndromeMari IllustriousNo ratings yet
- Changes in The Maternal Hypothalamic-Pituitary-Adrenal Axis in Pregnancy and Postpartum: Influences On Maternal and Fetal OutcomesDocument10 pagesChanges in The Maternal Hypothalamic-Pituitary-Adrenal Axis in Pregnancy and Postpartum: Influences On Maternal and Fetal OutcomesAirene ZulfikarNo ratings yet
- Stress, Memory, and The Hippocampus: Can't Live With It, Can't Live Without ItDocument22 pagesStress, Memory, and The Hippocampus: Can't Live With It, Can't Live Without ItsoylahijadeunvampiroNo ratings yet
- Anxiety: Insights Into Signs, Symptoms, Etiology, Pathophysiology, and TreatmentDocument13 pagesAnxiety: Insights Into Signs, Symptoms, Etiology, Pathophysiology, and TreatmentMichael Judika Deardo PurbaNo ratings yet
- Neuropeptido YDocument8 pagesNeuropeptido YAngela Del Castillo AriasNo ratings yet