You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
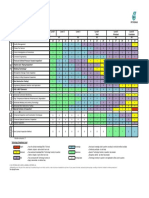
- Preschool Key Developmental Indicators ChartDocument1 pagePreschool Key Developmental Indicators Chartapi-375217674No ratings yet
- Learning Chess Step4 SolutionsDocument15 pagesLearning Chess Step4 SolutionsZeynep Ciftci100% (4)
- BGB C 2016Document9 pagesBGB C 2016Susuru AsepNo ratings yet
- 2 - Preferred Practice PatternDocument7 pages2 - Preferred Practice PatternSusuru AsepNo ratings yet
- Signs in Chest ImagingDocument13 pagesSigns in Chest ImagingSusuru AsepNo ratings yet
- Imaging of Acute Pulmonary Embolism: An UpdateDocument19 pagesImaging of Acute Pulmonary Embolism: An UpdateSusuru AsepNo ratings yet
- Covid 19 MriDocument2 pagesCovid 19 MriSusuru AsepNo ratings yet
- Esesmen Dan Manajemen Pasien DemensiaDocument19 pagesEsesmen Dan Manajemen Pasien DemensiaSusuru AsepNo ratings yet
- Cerebrospinal Fluid (CSF) Collection GuidelinesDocument2 pagesCerebrospinal Fluid (CSF) Collection GuidelinesSusuru AsepNo ratings yet
- Bed Thesis FormatDocument10 pagesBed Thesis FormatMuhammad JavedNo ratings yet
- Lecture 4-Fluid KinematicsDocument37 pagesLecture 4-Fluid KinematicsFaith TariuNo ratings yet
- Junttan PMx27 DatasheetDocument4 pagesJunttan PMx27 DatasheetIkhsan SetiawanNo ratings yet
- WorkApps ChatDocument18 pagesWorkApps ChatRuletaNo ratings yet
- Compression Labs Incorporated v. Dell, Inc Et Al - Document No. 35Document14 pagesCompression Labs Incorporated v. Dell, Inc Et Al - Document No. 35Justia.comNo ratings yet
- Steering: Essential To Driving: Latest Blog EntryDocument8 pagesSteering: Essential To Driving: Latest Blog EntrySoham DeNo ratings yet
- Material Downloaded From - 1 / 4Document4 pagesMaterial Downloaded From - 1 / 4NihalSoniNo ratings yet
- LIST Egam3s 2019Document92 pagesLIST Egam3s 2019Muhammad ZulvindadaniNo ratings yet
- LPJ MR AreaDocument11 pagesLPJ MR AreaBagas AudiNo ratings yet
- English SummaryDocument9 pagesEnglish Summaryyaminshehadeh14No ratings yet
- AR1740 EdD User Guide HomeLYnk enDocument162 pagesAR1740 EdD User Guide HomeLYnk enjcalberdiNo ratings yet
- The Girl On The Train (2016) - Plot Summary - IMDbDocument1 pageThe Girl On The Train (2016) - Plot Summary - IMDbhaddad walidNo ratings yet
- Yates Washington 0250O 16760Document103 pagesYates Washington 0250O 16760Abeer NåśįmNo ratings yet
- SKG15 TIR Inspection Engineering 2016.5Document1 pageSKG15 TIR Inspection Engineering 2016.5Abdul RahimNo ratings yet
- Application Form 1Document1 pageApplication Form 1raileosibo123No ratings yet
- Formula Sheet For Stage 6 PhysicsDocument8 pagesFormula Sheet For Stage 6 PhysicskevinNo ratings yet
- Oracle Database 12C SQL WORKSHOP 2 - Student Guide Volume 2 PDFDocument486 pagesOracle Database 12C SQL WORKSHOP 2 - Student Guide Volume 2 PDFenrrichel0% (1)
- History of Photography Research Paper TopicsDocument5 pagesHistory of Photography Research Paper Topicsgw11pm8h100% (1)
- Schooling and Aggregation of FishDocument12 pagesSchooling and Aggregation of FishMUHAMMAD HAIKAL0% (1)
- Physics Assessment 1Document8 pagesPhysics Assessment 1Nayyir Mumtasir Rahman 2323059047No ratings yet
- Bahan-Bahan Masak Dalam Bahasa InggrisDocument30 pagesBahan-Bahan Masak Dalam Bahasa Inggrisberd zainNo ratings yet
- Mrs - Nandini - Villa-56 BOQDocument3 pagesMrs - Nandini - Villa-56 BOQAlemeluNo ratings yet
- Company Profile of Maruti SuzukiDocument10 pagesCompany Profile of Maruti SuzukiDave ChaudharyNo ratings yet
- (B) Superposition TheoremDocument4 pages(B) Superposition TheoremMuhammad AbdullahNo ratings yet
- Digital MarketingDocument8 pagesDigital MarketingYounus ahmedNo ratings yet
- Upside Down Pineapple Cake Parsi Style by Tanaz Daruwalla Medhora - Bawi BrideDocument2 pagesUpside Down Pineapple Cake Parsi Style by Tanaz Daruwalla Medhora - Bawi BridefatduckNo ratings yet
- New College Grads Mismatch To Their JobsDocument20 pagesNew College Grads Mismatch To Their JobsJoanna SilvestreNo ratings yet
- Control of MachinesDocument355 pagesControl of Machineswado11No ratings yet