You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Professional Summary: Email ID: Name Mobile NoDocument4 pagesProfessional Summary: Email ID: Name Mobile NoMallikaNo ratings yet
- Introduction To DAXDocument7 pagesIntroduction To DAXMallikaNo ratings yet
- Int Marketid String Spudtype String Producingstate Int Price (Per KG)Document5 pagesInt Marketid String Spudtype String Producingstate Int Price (Per KG)MallikaNo ratings yet
- PH No: 9290981182, 6303673482: Venkata Satya Sai Naga Amrutha MajetiDocument2 pagesPH No: 9290981182, 6303673482: Venkata Satya Sai Naga Amrutha MajetiMallikaNo ratings yet
- KMM Institute of Post Graduate Studies:: Online Gas Booking SystemDocument61 pagesKMM Institute of Post Graduate Studies:: Online Gas Booking SystemMallikaNo ratings yet
- Post Dcpu/ SAA: Annexure-I Recruitment Notification "District Child Protection Unit" (Dcpu) "Document3 pagesPost Dcpu/ SAA: Annexure-I Recruitment Notification "District Child Protection Unit" (Dcpu) "MallikaNo ratings yet
- Code Coverage Testing: 1. Statement Coverage (Line Coverage)Document17 pagesCode Coverage Testing: 1. Statement Coverage (Line Coverage)MallikaNo ratings yet
- Loop Coverage: I. Example of Loop Covergae Testing (Loop Coverage For)Document8 pagesLoop Coverage: I. Example of Loop Covergae Testing (Loop Coverage For)MallikaNo ratings yet
- Path CoverageDocument30 pagesPath CoverageMallikaNo ratings yet
- Software Testing: Overview of SDLCDocument5 pagesSoftware Testing: Overview of SDLCMallikaNo ratings yet
- Junit TestingDocument15 pagesJunit TestingMallikaNo ratings yet
- Aws - S3Document10 pagesAws - S3MallikaNo ratings yet
- Curriculum Vitate:: Mallikanandi369Document2 pagesCurriculum Vitate:: Mallikanandi369MallikaNo ratings yet
- Curriculum Vitate:: Mallikanandi369Document2 pagesCurriculum Vitate:: Mallikanandi369MallikaNo ratings yet
- Branch CoverageDocument11 pagesBranch CoverageMallikaNo ratings yet
- AndhraPradesh-01 Cycle3Document161 pagesAndhraPradesh-01 Cycle3MallikaNo ratings yet
- S.V.University, Tirupati: Semester: IiDocument13 pagesS.V.University, Tirupati: Semester: IiMallikaNo ratings yet
- Data Base Management System: Iii Year V SemesterDocument5 pagesData Base Management System: Iii Year V SemesterMallikaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Jul Dec 2019 SA 1 ScopeDocument20 pagesJul Dec 2019 SA 1 ScopeBonginkosi100% (1)
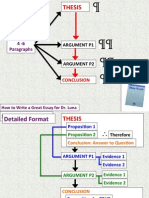
- How To Write An Essay PDFDocument9 pagesHow To Write An Essay PDFCarl Luna100% (2)
- Topic Content Standards Performance Standards Learning Competency Learning ObjectivesDocument9 pagesTopic Content Standards Performance Standards Learning Competency Learning ObjectivesLianne Marie CabanginNo ratings yet
- Abra State Institute of Sciences and Technology Graduate SchoolDocument2 pagesAbra State Institute of Sciences and Technology Graduate SchoolSheenley Pardo100% (1)
- Sub: Draughtsman (Architecture/Structure/Civil) : To, The HR ManagerDocument5 pagesSub: Draughtsman (Architecture/Structure/Civil) : To, The HR ManagerSyed Abdul Nayeem100% (2)
- ATR Flight Deck SecurityDocument2 pagesATR Flight Deck Securitybroken_airplaneNo ratings yet
- Cars Should Be Banned From CitiesDocument2 pagesCars Should Be Banned From Citiesnona djenNo ratings yet
- Benji Bruce BioDocument1 pageBenji Bruce BioVictorNo ratings yet
- Applied Economics Module 10Document16 pagesApplied Economics Module 10flo75% (4)
- Apparel House, Institutional Area Sector-44, Gurgaon Haryana-122 003Document8 pagesApparel House, Institutional Area Sector-44, Gurgaon Haryana-122 003abhiNo ratings yet
- CWTS101 - OL3-LeadershipDocument4 pagesCWTS101 - OL3-LeadershipAyle NakamuraNo ratings yet
- Ele Social Studies ArabicDocument23 pagesEle Social Studies ArabicNasrin AktherNo ratings yet
- RiskAssessment For Precast Foundation and Road MarkingDocument13 pagesRiskAssessment For Precast Foundation and Road MarkingAneessh KumarNo ratings yet
- Air Transportation 2Document19 pagesAir Transportation 2Clerk Janly R FacunlaNo ratings yet
- The Yom Kippur War by Insight Team of The London Sunday Time PDFDocument560 pagesThe Yom Kippur War by Insight Team of The London Sunday Time PDFNestor Andres Ortiz Riquelme100% (3)
- Learning Delivery Modalities Course For Teachers: LDM Module 3A: Designing Instruction in The Different Learning ModalityDocument39 pagesLearning Delivery Modalities Course For Teachers: LDM Module 3A: Designing Instruction in The Different Learning ModalityJovie Masongsong78% (9)
- 20 Years of CARPDocument132 pages20 Years of CARPNational Food CoalitionNo ratings yet
- English For Midwifery SyllabusDocument4 pagesEnglish For Midwifery SyllabusResaNo ratings yet
- Startup Evolution Curve Excerpt 2017-05-31Document193 pagesStartup Evolution Curve Excerpt 2017-05-31LEWOYE BANTIENo ratings yet
- 1 - 2019 - Fundamentals of Taxation An Introduction To Tax Policy Tax Law and Tax AdministrationDocument197 pages1 - 2019 - Fundamentals of Taxation An Introduction To Tax Policy Tax Law and Tax AdministrationSeydina-Ousmane Dramé100% (1)
- Grade 6 - Digital Drama Unplugged - Taking The Lead Student HandoutDocument3 pagesGrade 6 - Digital Drama Unplugged - Taking The Lead Student Handoutapi-465086775No ratings yet
- Compiled Sec12 19Document172 pagesCompiled Sec12 19anjisy100% (1)
- Three Level of Product MarketingDocument8 pagesThree Level of Product MarketingDorian GoNo ratings yet
- Contract Works Procurement Plan TemplateDocument5 pagesContract Works Procurement Plan TemplateFrancisco SalazarNo ratings yet
- Values, Ethics and Working CollaborativelyDocument14 pagesValues, Ethics and Working CollaborativelyFahmina AhmedNo ratings yet
- Claudette Colvin Chapters 1 3Document1 pageClaudette Colvin Chapters 1 3api-328194161No ratings yet
- World Wildlife Report 2020 9julyDocument136 pagesWorld Wildlife Report 2020 9julymarsveloNo ratings yet
- Cheap Air Tickets Online, International Flights To India, Cheap International Flight Deals - SpiceJet AirlinesDocument2 pagesCheap Air Tickets Online, International Flights To India, Cheap International Flight Deals - SpiceJet Airlinescpe plNo ratings yet
- Syldavia (Claimant) - Trade Moot CourtDocument19 pagesSyldavia (Claimant) - Trade Moot CourtjeffreyNo ratings yet
- Fieldwork Risk Assessment (Low Risk Activities) Fieldwork Project DetailsDocument3 pagesFieldwork Risk Assessment (Low Risk Activities) Fieldwork Project DetailsDiyoke HenryNo ratings yet