You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 112 HTP - HypertensionDocument4 pages112 HTP - HypertensionMae CeaesarNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Reflection About Confidentiality and Privacy in HealthcareDocument1 pageReflection About Confidentiality and Privacy in HealthcareMae CeaesarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- NCP - Risk For FallsDocument5 pagesNCP - Risk For FallsMae CeaesarNo ratings yet
- Thryoid Cancer NotesDocument1 pageThryoid Cancer NotesMae CeaesarNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- NCP - Impaired Social InteractionDocument3 pagesNCP - Impaired Social InteractionMae Ceaesar50% (2)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- MedSurg Notes - LeukemiaDocument3 pagesMedSurg Notes - LeukemiaMae CeaesarNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
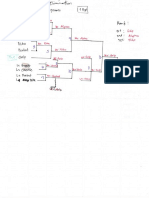
- 7 Teams Double Elimination TournamentDocument1 page7 Teams Double Elimination TournamentMae CeaesarNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- MedSurg Notes - Radiation Therapy9Document5 pagesMedSurg Notes - Radiation Therapy9Mae CeaesarNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- NCP Template ObDocument7 pagesNCP Template ObMae CeaesarNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Creating Teams Round Robin TournamentDocument1 pageCreating Teams Round Robin TournamentMae CeaesarNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- EDB Postgres Failover Manager Guide v2.1Document86 pagesEDB Postgres Failover Manager Guide v2.1Anggia MauritianaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Bin Adam Group of CompaniesDocument8 pagesBin Adam Group of CompaniesSheema AhmadNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Process Industry Practices Insulation: PIP INEG2000 Guidelines For Use of Insulation PracticesDocument15 pagesProcess Industry Practices Insulation: PIP INEG2000 Guidelines For Use of Insulation PracticesZubair RaoofNo ratings yet
- Rab Sikda Optima 2016Document20 pagesRab Sikda Optima 2016Julius Chatry UniwalyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gmail - ICICI BANK I PROCESS HIRING FOR BACKEND - OPERATION PDFDocument2 pagesGmail - ICICI BANK I PROCESS HIRING FOR BACKEND - OPERATION PDFDeepankar ChoudhuryNo ratings yet
- Operational Readiness and Airport TransferDocument2 pagesOperational Readiness and Airport TransferochweriNo ratings yet
- List of Modern Equipment and Farm ToolsDocument15 pagesList of Modern Equipment and Farm ToolsCarl Johnrich Quitain100% (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 3g Node B On Ip MediaDocument79 pages3g Node B On Ip MediaBsskkd KkdNo ratings yet
- 2432 - Test Solutions - Tsol - 2432 - 21702Document5 pages2432 - Test Solutions - Tsol - 2432 - 21702Anmol PanchalNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Uh 60 ManualDocument241 pagesUh 60 ManualAnonymous ddjwf1dqpNo ratings yet
- KiSoft Sort & Pack Work Station (User Manual)Document41 pagesKiSoft Sort & Pack Work Station (User Manual)Matthew RookeNo ratings yet
- Micro - Systemic Bacteriology Questions PDFDocument79 pagesMicro - Systemic Bacteriology Questions PDFShashipriya AgressNo ratings yet
- Aspek Perpajakan Dalam Transfer Pricing: Related PapersDocument15 pagesAspek Perpajakan Dalam Transfer Pricing: Related PapersHasrawati AzisNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Pautas Anatómicas para La Inserción de Minitornillos: Sitios PalatinosDocument11 pagesPautas Anatómicas para La Inserción de Minitornillos: Sitios PalatinosValery V JaureguiNo ratings yet
- New Microsoft Office Word DocumentDocument5 pagesNew Microsoft Office Word DocumentSukanya SinghNo ratings yet
- XU-CSG Cabinet Minutes of Meeting - April 4Document5 pagesXU-CSG Cabinet Minutes of Meeting - April 4Harold John LaborteNo ratings yet
- Case Study On Goodearth Financial Services LTDDocument15 pagesCase Study On Goodearth Financial Services LTDEkta Luciferisious Sharma0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Reading Stressful Jobs 1 4Document4 pagesReading Stressful Jobs 1 4Ivana C. AgudoNo ratings yet
- Dance Terms Common To Philippine Folk DancesDocument7 pagesDance Terms Common To Philippine Folk DancesSaeym SegoviaNo ratings yet
- GA Power Capsule For SBI Clerk Mains 2024 (Part-2)Document82 pagesGA Power Capsule For SBI Clerk Mains 2024 (Part-2)aa1904bbNo ratings yet
- Jota - EtchDocument3 pagesJota - EtchRidwan BaharumNo ratings yet
- What Is Product Management?Document37 pagesWhat Is Product Management?Jeffrey De VeraNo ratings yet
- Remedy MidTier Guide 7-5Document170 pagesRemedy MidTier Guide 7-5martin_wiedmeyerNo ratings yet
- ANS145 - Beef Cattle ProductionDocument52 pagesANS145 - Beef Cattle ProductionEgie BulawinNo ratings yet
- Model Answer Winter 2015Document38 pagesModel Answer Winter 2015Vivek MalwadeNo ratings yet
- AMO Exercise 1Document2 pagesAMO Exercise 1Jonell Chan Xin RuNo ratings yet
- Assessment 4 PDFDocument10 pagesAssessment 4 PDFAboud Hawrechz MacalilayNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- VLSI Implementation of Floating Point AdderDocument46 pagesVLSI Implementation of Floating Point AdderParamesh Waran100% (1)
- Course DescriptionDocument54 pagesCourse DescriptionMesafint lisanuNo ratings yet
- Rocker ScientificDocument10 pagesRocker ScientificRody JHNo ratings yet