You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Service Manual For Preventive Maintenance 6SE483 0303Document55 pagesService Manual For Preventive Maintenance 6SE483 0303Antony MorenoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Neuro Exam ReviewDocument6 pagesNeuro Exam ReviewDianne Flores100% (2)
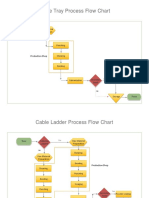
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- D.S.R. - 2012-2013finel PDWDocument243 pagesD.S.R. - 2012-2013finel PDWprashantlingayat25% (4)
- Goody Anthropology of Sensess and Sensations LRF 2002 45 PDFDocument13 pagesGoody Anthropology of Sensess and Sensations LRF 2002 45 PDFAntroVirtualNo ratings yet
- Creative Idea Bulb PowerPoint TemplateDocument36 pagesCreative Idea Bulb PowerPoint TemplateReza Adhi NugrohoNo ratings yet
- Biotech ProjectDocument14 pagesBiotech ProjectRahul V ChandramouliNo ratings yet
- Power Gating - Power Management Technique: VLSI Basics and Interview QuestionsDocument12 pagesPower Gating - Power Management Technique: VLSI Basics and Interview QuestionsRohith RajNo ratings yet
- Lukong Cornelius Fai - Feynman Path Integrals in Quantum Mechanics and Statistical Physics-CRC Press (2021)Document415 pagesLukong Cornelius Fai - Feynman Path Integrals in Quantum Mechanics and Statistical Physics-CRC Press (2021)Vi Kem100% (1)
- PRACH Optimization - V1Document11 pagesPRACH Optimization - V1Tulipe Pivoine100% (5)
- Air Transportation ReviewerDocument16 pagesAir Transportation ReviewerJuly BacarNo ratings yet
- ORTHOPEDICS: FEMORAL FRACTURES IN CHILDRENDocument8 pagesORTHOPEDICS: FEMORAL FRACTURES IN CHILDRENMitra NofembriNo ratings yet
- Pemeriksaan PenunjangDocument4 pagesPemeriksaan PenunjangMitra NofembriNo ratings yet
- Acute Myeloid Leukemia Masquerading As Acute Appendicitis: CorrespondenceDocument2 pagesAcute Myeloid Leukemia Masquerading As Acute Appendicitis: CorrespondenceMitra NofembriNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaMitra NofembriNo ratings yet
- Uji Normalitas: 1. S. AureusDocument10 pagesUji Normalitas: 1. S. AureusMitra NofembriNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaMitra NofembriNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaMitra NofembriNo ratings yet
- Pyogenic Microorganisms: Roy, Nova, Jessie, Szechia, and ShangyoungDocument34 pagesPyogenic Microorganisms: Roy, Nova, Jessie, Szechia, and ShangyoungMitra NofembriNo ratings yet
- 69803Document6 pages69803Mitra NofembriNo ratings yet
- HiponatremiaDocument10 pagesHiponatremiaHakim Arul100% (1)
- DDGDocument80 pagesDDGMitra NofembriNo ratings yet
- 58 PDFDocument16 pages58 PDFMitra NofembriNo ratings yet
- 43 48Document6 pages43 48Mitra NofembriNo ratings yet
- 33A AntioxidantnDocument6 pages33A AntioxidantnMitra NofembriNo ratings yet
- 1 6 (2) 2008hDocument21 pages1 6 (2) 2008hMitra NofembriNo ratings yet
- Haemodynamic DisordersDocument3 pagesHaemodynamic DisordersMitra NofembriNo ratings yet
- MCQs in Oral Surgery by Babu SParmarDocument517 pagesMCQs in Oral Surgery by Babu SParmarAmr KhattabNo ratings yet
- LA36300 Circuit Breaker Data SheetDocument2 pagesLA36300 Circuit Breaker Data SheetALEJANDRO DOMINGUEZNo ratings yet
- DC TC 600 L, 01.00, enDocument61 pagesDC TC 600 L, 01.00, enDarkNo ratings yet
- Taller de Calor EstDocument2 pagesTaller de Calor EstDiegoMuñozNo ratings yet
- Lecture Drugs in Sport - NotesDocument14 pagesLecture Drugs in Sport - NotesDavid FornitoNo ratings yet
- VOLLEYBALL HISTORY AND RULESDocument12 pagesVOLLEYBALL HISTORY AND RULESJennybelle MolinaNo ratings yet
- TermoooDocument11 pagesTermoooJay-r Capate TanNo ratings yet
- Energy Security IndexDocument13 pagesEnergy Security IndexCarlos AlvarezNo ratings yet
- Dont Think About A ZebraDocument2 pagesDont Think About A ZebraD2WNo ratings yet
- CAS circuit analysis simulationDocument9 pagesCAS circuit analysis simulationIan MejiaNo ratings yet
- LP in ArtsDocument6 pagesLP in ArtsBilindaNo ratings yet
- Despiece Motor Briggs 14hp 400707122102Document58 pagesDespiece Motor Briggs 14hp 400707122102leinadNo ratings yet
- Briarborn - Nature's ProtectorsDocument6 pagesBriarborn - Nature's Protectorsa1057soulNo ratings yet
- Unit Ii, Lesson 4: Qualitative Research in Different Areas of KnowledgeDocument6 pagesUnit Ii, Lesson 4: Qualitative Research in Different Areas of KnowledgeJessy RoseNo ratings yet
- InglesDocument6 pagesInglesyarilisNo ratings yet
- Epidemiology and Etiology of Peptic Ulcer DiseaseDocument5 pagesEpidemiology and Etiology of Peptic Ulcer DiseaseDeepali Mahajan ChaudhariNo ratings yet
- Quick Manual v2.3: Advanced LTE Terminal With Flexible Inputs ConfigurationDocument16 pagesQuick Manual v2.3: Advanced LTE Terminal With Flexible Inputs ConfigurationanditowillyNo ratings yet
- Final QuesDocument5 pagesFinal QuesMani KumarNo ratings yet
- Master Drive 6RA70 Parameter ListDocument186 pagesMaster Drive 6RA70 Parameter Listsanjaya srivastava100% (3)
- Math10 Q2 Mod24 WritingtheEquationofaCircleandDeterminingtheCenterandRadiusofaCircle V3-1Document19 pagesMath10 Q2 Mod24 WritingtheEquationofaCircleandDeterminingtheCenterandRadiusofaCircle V3-1Bridget SaladagaNo ratings yet