Professional Documents
Culture Documents
Meals 2013
Uploaded by
Harry CenCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Meals 2013
Uploaded by
Harry CenCopyright:
Available Formats
CURRENT CONCEPTS
Hand Fractures: A Review of Current
Treatment Strategies
Clifton Meals, MD, Roy Meals, MD
CME INFORMATION AND DISCLOSURES
The Review Section of JHS will contain at least 3 clinically relevant articles selected by the ASSH Disclosure Policy: As a provider accredited by the ACCME, the ASSH must ensure
editor to be offered for CME in each issue. For CME credit, the participant must read the balance, independence, objectivity, and scientific rigor in all its activities. All authors
articles in print or online and correctly answer all related questions through an online participating in the activity are required to disclose to the audience any relevant financial
examination. The questions on the test are designed to make the reader think and will relationships with any commercial interest to the provider. The intent of this disclosure is not
occasionally require the reader to go back and scrutinize the article for details. to prevent authors with relevant financial relationships from serving as authors, but rather to
provide members of the audience with information on which they can make their own
The JHS CME Activity fee of $20.00 includes the exam questions/answers only and does not judgments. The ASSH must resolve any conflicts of interest prior to the commencement of the
include access to the JHS articles referenced. educational activity. It remains for the audience to determine if the audience’s relationships
may influence the educational content with regard to exposition or conclusion. When
Statement of Need: This CME activity was developed by the JHS review section editors and
unlabeled or unapproved uses of drugs or devices are discussed, these will also be indicated.
review article authors as a convenient education tool to help increase or affirm reader’s
knowledge. The overall goal of the activity is for participants to evaluate the appropriateness Disclosures for this Article
of clinical data and apply it to their practice and the provision of patient care. Editors
The editors involved with this CME activity and all content validation/peer reviewers of this
Accreditation: The ASSH is accredited by the Accreditation Council for Continuing Medical
journal-based CME activity have reported no relevant financial relationships with commercial
Education to provide continuing medical education for physicians.
interest(s).
AMA PRA Credit Designation: The American Society for Surgery of the Hand designates this
Authors
Journal-Based CME activity for a maximum of 2.00 “AMA PRA Category 1 Credits™”. Physicians All authors of this journal-based CME activity have reported no relevant financial
should claim only the credit commensurate with the extent of their participation in the activity. relationships with commercial interest(s).
ASSH Disclaimer: The material presented in this CME activity is made available by the ASSH Planners
for educational purposes only. This material is not intended to represent the only methods or The planners involved with this journal-based CME activity have reported no relevant
the best procedures appropriate for the medical situation(s) discussed, but rather it is financial relationships with commercial interest(s). The editorial and education staff involved
intended to present an approach, view, statement, or opinion of the authors that may be with this journal-based CME activity has reported no relevant financial relationships with
helpful, or of interest, to other practitioners. Examinees agree to participate in this medical commercial interest(s).
education activity, sponsored by the ASSH, with full knowledge and awareness that they
waive any claim they may have against the ASSH for reliance on any information presented. Learning Objectives
The approval of the US Food and Drug Administration is required for procedures and drugs • Appraise the history and epidemiology and mechanics of hand fractures.
that are considered experimental. Instrumentation systems discussed or reviewed during this • Clarify the diagnosis of hand fractures through clinical and radiographic findings.
educational activity may not yet have received FDA approval. • List general operative and nonoperative treatment principles of hand fractures.
• Elucidate the treatment principles of individual hand fractures, including the thumb.
Provider Information can be found at http://www.assh.org/Pages/ContactUs.aspx. • Discuss the complications of hand fractures and their treatment.
Technical Requirements for the Online Examination can be found at http:// Deadline: Each exam purchased in 2013 must be completed by January 31, 2014, to be
jhandsurg.org/cme/home. eligible for CME. A certificate will be issued upon completion of the activity. Estimated time to
complete each month’s JHS CME activity is 2 hours.
Privacy Policy can be found at http://www.assh.org/pages/ASSHPrivacyPolicy.aspx. Copyright © 2013 by the American Society for Surgery of the Hand. All rights reserved.
Fractures of the tubular bones of the hand are common and potentially debilitating. The
majority of these injuries may be treated without an operation. Surgery, however, offers
distinct advantages in properly selected cases. We present a review of hand fracture
management, with special attention paid to advances since 2008. The history and mecha-
nisms of these fractures are discussed, as are treatment options and common complications.
Early mobilization of the fractured hand is emphasized because soft tissue recovery may be
Current Concepts
more problematic than that of bone. (J Hand Surg 2013;38A:1021–1031. Copyright © 2013
by the American Society for Surgery of the Hand. All rights reserved.)
Key words Hand, fracture, metacarpal, phalanges.
© ASSH 䉬 Published by Elsevier, Inc. All rights reserved. 䉬 1021
1022 HAND FRACTURES: CURRENT TREATMENT STRATEGIES
vulnerable. Its ability phalanx with a fixateur externe, a phrase he coined.6
T
HE HAND IS VALUABLE AND
to both sense and manipulate its environment is Kirschner developed the use of fine wires for skeletal
unique in nature. As such, the hand is fre- traction; this technique and fixation with K-wires are
quently injured. Despite its mechanical refinement, the relevant to the treatment of hand fractures a century
hand is particularly resilient to fractures, and when they later. Twentieth-century advances in anesthesia, radiol-
occur, broken digits can often be treated without an ogy, and metallurgy have helped to refine the operative
operation. Surgery, nonetheless, has a place in the man- care of hand fractures. The fact remains, however, as it
agement of carefully chosen cases. Although hand frac- was known to ancient physicians, that the majority of
tures are generally forgiving, soft tissue injury is not. It these injuries can be treated without surgery.7
is easy for the treating physician to do more harm than
good, even without cutting the skin. Hand surgeons EPIDEMIOLOGY
have special claim to only the most complicated inju- Hand fractures are among the most common skeletal
ries; many fractures of the hand can be treated by a injuries. As is the case with many orthopedic injuries,
variety of physicians. The majority of hand fractures are young men and elderly women are most susceptible.
appropriately treated by emergency physicians, primary Modes of injury in different age groups are predictable:
care doctors, and general orthopedic and plastic sur- children and young adults are frequently injured in
geons. The following is intended for an accordingly sports-related activities, middle-age manual laborers are
broad audience. We present management strategies for prone to work-related injuries, and older patients may
the most representative tubular bone fractures of the experience hand trauma as the result of a fall or motor
hand. We highlight recent research to avoid rehashing vehicle collision. The distal phalanx is the most com-
previous reviews.1– 4 monly fractured bone in the hand.1 A large subset of
young adult males fracture their fifth metacarpal, clas-
HISTORY sically the result of violent contact with the fist.3,8
Rudimentary care of hand fractures (eg, rest and eleva-
tion) is presumably as old as humans themselves. Up- DIAGNOSIS
right posture may have contributed to an increase in Diagnosis of hand fractures begins with a thorough
these injuries, and today, falls from standing height patient interview. The patient should describe the mech-
remain a major source of hand injuries. The ancient anism of injury because this may suggest certain reduc-
Egyptian Imhotep described reduction and immobiliza- tion maneuvers, assist in identifying secondary injuries,
tion of fractures in 3000 BC. Hippocrates in 200 BC and and reveal pathological fractures. A very low-impact
Galen in AD 160 recommended prolonged immobiliza-
injury leading to fracture, for instance, should raise the
tion of broken bones and frequent dressing changes.
suspicion of osteoporosis or enchondroma. In addition
More durable, plaster-based splinting materials were
to a history of the injury, it is important to note the
developed in the Middle East as early as the 10th
patient’s handedness, their functional status, occupa-
century. As this technology reached 19th-century Eu-
tion, hobbies, and expectations for recovery. A 25-year-
rope, it permitted less frequent splint exchange in an era
old concert pianist and a retiree with the same fracture
of population expansion and increased demand for
represent different challenges to the treating physician.
medical attention. Sophisticated splinting of the hand
Physical examination of the hand begins with noting
and the so-called “intrinsic-plus” position were advo-
skin integrity including abrasions and lacerations and
cated by James in the 20th century. The Belgian sur-
the location and extent of any bruising, swelling, or
geon Lambotte described operative care of a phalangeal
underlying deformity. A neurovascular examination is
fracture as early as 1904.5 He stabilized this proximal
undertaken with attention paid to the digits distal to any
Current Concepts
injury. Angular and particularly rotational deformity
FromtheDepartmentofOrthopedics,GeorgeWashingtonUniversityMedicalCenter,Washington,DC,
and the Department of Orthopedics, UCLA Medical Center, Los Angeles, California. can be subtle when the patient is unable to make a full
Received for publication August 7, 2012; accepted February 7, 2013.
fist and demonstrate parallel digital alignment. In this
instance, examining end-on the digital pulps and the
No benefits in any form have been received or will be received related directly or indirectly to the
subject of this article. planar alignment of the nails with respect to the adja-
Corresponding author: Clifton Meals, MD, George Washington University Medical Center, De- cent digits and the opposite hand is revealing. Caution
partment of Orthopedics, 22nd & I Street, NW, 7th Floor, Washington, DC 20037; e-mail: must be exercised, however, when identifying a patho-
cliftongm@gmail.com. logical supination deformity in the small finger because
0363-5023/13/38A05-0032$36.00/0 the uninjured small finger tends to scissor with the ring
http://dx.doi.org/10.1016/j.jhsa.2013.02.017
finger at midflexion and then come into parallel align-
JHS 䉬 Vol A, May
HAND FRACTURES: CURRENT TREATMENT STRATEGIES 1023
ment with full flexion. The hand should be lightly trauma or open fracture, and in the face of concomitant
palpated, seeking points of maximal tenderness. Passive injury to nerves, vessels, and soft tissue.1
and active range of motion should be documented at all Open fractures of the hand are common and may
affected and adjacent joints. Range of motion maneu- necessitate irrigation and debridement in the operating
vers may be facilitated by neuroblockade at the meta- room. Initial management is case-based but often con-
carpophalangeal (MCP) joints or the wrist but not be- sists of irrigation, sterile coverage of the wound, anti-
fore recording a neurological examination. In biotics, and tetanus prophylaxis.
evaluating a hand fracture, injury to nerves, vessels, Reduction is appropriate in the initial care of dis-
ligaments, and tendons must be identified and treated placed fractures, and special techniques for certain frac-
with the same attention due any broken bone. tures are discussed later. All reduction maneuvers rely
Good-quality radiographs are the cornerstone of on gentle traction. They are in general aided by nerve
fracture diagnosis. Most metacarpal fractures are accu- blocks and gentle flexion of the MCP joints and wrist.
rately characterized with posteroanterior, semiprona- Splints should selectively limit motion of injured
tion, and lateral views of the hand. A true lateral view parts. Plaster molds well and is preferable for holding a
of the hand, evident by the superimposition of the reduction. Fiberglass and other materials may be appro-
pisiform and distal pole of the scaphoid and the stag- priate for soft tissue injuries and stable fractures. Im-
gering of each finger, may be difficult to obtain.9 None- mobilization of the wrist in extension is desirable to
theless, this orthogonal view is necessary to fully char- minimize stiffness, although patients are often reluctant
acterize fractures and may identify injuries not obvious to assume this posture on their own.3 A dorsal splint
in other views (eg, fracture dislocations of the ulnar extending from the midforearm to the fingertips is use-
carpometacarpal joints).10 To accurately identify and ful in this regard. Such a splint holds the wrist in some
characterize phalangeal fractures, the same views, per- extension, flexes the MCP joints to 90°, and permits full
haps with the inclusion of a semisupination view and a extension of the interphalangeal joints. Patients may be
fan lateral view, must be obtained with the x-ray beam reluctant to flex their MCP joints, and an overly bulky
centered over the area of concern, not through the splint may obscure residual extension. To aid in flexion
center of the palm as with screening films. Advanced of the MCP joints, the distal end of the splint may be
imaging of the tubular bones of the hand is rarely held down with strips of tape that span the palm and are
necessary, although magnetic resonance imaging (MRI) attached at the wrist. When properly applied, the dorsal
may help to evaluate concomitant soft tissue injuries hand splint has utility in treating a wide variety of hand
and pathological fractures. fractures.
Fractures are evaluated with respect to their location, Splints may be used until the fracture is healed or
orientation, displacement, angulation, degree of com- exchanged for a cast once soft tissue swelling has
minution, and any associated joint involvement or dis- resolved. For the vast majority of metacarpal and pha-
location. Especially in the setting of infection or open langeal fractures, clinical stability occurs well before
injury, the presence of radiopaque foreign bodies must radiographic evidence of healing. Initiation of protected
be noted. X-rays reveal more than fracture lines, and mobilization should be based on time since injury and
this information should be noted. Degenerative, onco- fracture site tenderness rather than x-rays. Over-reliance
logical, rheumatological, and metabolic processes are on radiographs for confirmation of healing may result in
evident on radiographs, and each is potentially more a permanently stiff hand. Immobilizing hand fractures
serious than the patient’s primary complaint. for longer than 4 weeks is rarely necessary. Movement
of noninjured portions of the hand, as well as the
TREATMENT forearm, elbow, and shoulder, should be encouraged
General principles from the outset. In this regard, slings are counterpro-
Most hand fractures are well managed without surgery. ductive.
Current Concepts
This was known to ancient physicians; however, today
we better appreciate the dangers of prolonged immobi- Distal phalanx
lization.7 Stiffness, pressure sores, and, rarely, compart- Tuft fractures of the distal phalanx result from crush
ment syndrome may result from mismanaged casting or injuries, and soft tissue trauma is often of greater con-
splinting, and in this sense, “conservative” treatment cern than the broken bone. Large subungual hematomas
may be particularly risky. Surgery is indicated when should be decompressed by manually drilling a hole in
early mobilization of soft tissues is critical, when the the nail plate with a hypodermic needle or electrocau-
fracture is otherwise unreducible, in instances of poly- tery device. Significant injury to the nail matrix is best
JHS 䉬 Vol A, May
1024 HAND FRACTURES: CURRENT TREATMENT STRATEGIES
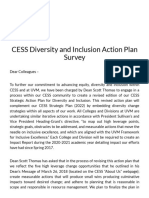
FIGURE 1: Kirschner wire fixation technique for a mallet finger injury. The distal interphalangeal DIP joint is flexed, and
Kirschner wires are used to block the avulsed fragment from displacing proximally. The fracture is reduced with extension of the
finger. The DIP joint is cross-pinned.
FIGURE 2: Sutures-over-button technique for mallet finger injuries. The DIP joint is opened dorsally with an H-shaped incision.
Bone holes are made with a Kirschner wire and suture is passed with the aid of hollow-bore needles. The suture exits the finger
pulp and is tied over a button. The DIP joint is cross-pinned.
treated by removal of the nail plate and suture of the or marked subluxation may be indications for sur-
nail bed. This may help to prevent entrapment of nail gery, although this is a matter of debate.13 Both
matrix in the fracture site and formation of an osseous acute and chronic mallet finger may be addressed
inclusion cyst. Open injuries, including those created to operatively. The use of mini-screws, extension
decompress a hematoma or repair the nail bed, require block pinning, sutures over a button, and Kirschner
oral antibiotics and protective splinting of the distal wires as joysticks technique have all been de-
interphalangeal (DIP) joint alone for 10 to 14 days. scribed (Figs. 1 and 2).14,15 A recent multicenter
Healing of the bone, often by fibrous union, is predict- comparison of various surgical techniques for mal-
able and alleviates symptoms, although tenderness may let finger found no significant difference in out-
persist for many months.1 comes.13
Transverse fractures through the shaft of the distal “Jersey finger” is the apex-volar equivalent of mallet
phalanx may take on apex-volar angulation but are finger and involves avulsion of the flexor digitorum
typically stable owing to the nail plate dorsally and the profundus tendon. Surgery is generally indicated, and
pulp’s fibrous septae volarly. Conservative treatment is direct repair with a suture-over-button technique may
appropriate. Comminuted or longitudinal fractures may be accomplished in the first 2 weeks after injury. Lon-
be more likely to displace and may be fixed with ger delays may involve retraction and degeneration of
Kirschner wires.1 Recent case series highlight a subset the flexor tendon and are treated on a case-by-case
of patients who developed symptomatic nonunions of basis.16
Current Concepts
distal phalanx fractures. These were effectively treated
open with cortical miniscrews11 or percutaneously with
variable pitch headless screws.12 Middle and proximal phalanx
Dorsal epiphyseal avulsions of the distal phalanx Minimally displaced, stable, extra-articular fractures of
result in an apex-dorsal, “mallet finger” deformity. the middle and proximal phalanges, in a compliant
Conservative treatment involves extension splint- patient, may be “buddy-taped” to an adjacent, uninjured
ing and care of soft tissue injury. If avulsed, the finger. Figl et al17 have recently described a “conser-
nail plate should be reduced beneath the nail fold vative functional” modification of the buddy-taping
to reapproximate the nail matrix and stabilize the technique in which the wrist and MCP joints are
fracture.1 Greater involvement of the joint surface casted in the safe position for 4 weeks. Motion at the
JHS 䉬 Vol A, May
HAND FRACTURES: CURRENT TREATMENT STRATEGIES 1025
FIGURE 3: Percutaneous, intramedullary disimpaction technique for treatment of fractures at the base of the middle phalanx. A
Kirschner wire is inserted retrograde into the middle phalanx and used to reduce fragments at the phalangeal base under
fluoroscopic guidance. The reduced joint is block-pinned in flexion.
interphalangeal joints is encouraged, particularly ex- cal strategy should adhere to the treatment guide-
tension at the proximal interphalangeal (PIP) joint. lines proposed by Kiefhaber and Stern22: (1) that
Unstable fractures, especially in older patients and in gliding reduction of the PIP joint be restored and
the setting of digital arthritis, are likely to result in subluxation at the fracture site be eliminated, (2)
stiffness if treated conservatively. Other potentially op- that early motion be established, and (3) as a
erative fractures include displaced or intra-articular secondary goal, that the joint surface be restored.
fractures in general, volar base injuries to the middle Cheah et al23 report satisfactory results with a volar
phalanx, and longitudinal unicondylar fractures of the mini-plate and screw technique at short-term follow-up.
head of the proximal phalanx.1 With regard to the latter, Percutaneous Kirschner wire fixation with dorsal block
Tan et al18 demonstrated satisfactory short-term out- pinning has been described, as has a percutaneous in-
come with intra-articularly placed screws. For these tramedullary technique for disimpaction and reduction
fractures, and for all fractures of the middle and prox- of volar fragments, also with dorsal block pinning (Fig.
imal phalanx, a wide variety of procedures have been 3).20,24 Dynamic external fixation of the injured PIP
described, many involving the use of Kirschner wires.1 joint is one treatment option (Fig. 4). Advantages in-
Selection of an operative strategy is case-based and clude relative ease of application and the potential for
depends heavily on surgeon preference. Regardless of early motion25–28; however, these wire and elastic con-
which hardware is chosen, attention to soft tissue is structs are not foolproof. Finsen29 reports only modest
paramount, namely with careful operative technique, restoration of motion with Suzuki pins and rubber trac-
brief immobilization in the intrinsic-plus position, and tion, potentially related to their use of stiff vessel loops
early motion. Although anatomical fixation of middle rather than more pliable rubber bands.
and proximal phalangeal fractures with screws, with or For chronic PIP joint fracture dislocations, Hamada
without plates, is appealing, it is fraught with problems. et al30 describe a 2-stage procedure in which the injured
Namely, the intra- and postoperative disturbance of the joint is held in a distracted position for 1 week before
closely aligned extensor tendon mechanism portends either percutaneous or open reduction and fixation and
stiffness. This is particularly vexing when rigid fixation the placement of a second, articulating external fixator.
is not secured and is followed by a period of prolonged Initial outcomes were positive, although long-term
postoperative immobilization. It is better to accept a less studies are lacking.30
than perfect radiographic reduction and achieve early Displaced fractures at the base of the proximal pha-
motion. lanx typically assume an apex-volar angulation and
PIP joint fractures are problematic, especially given should be reduced. Malunion may lead to a pseudo-
the importance of the PIP joint to hand function in clawing of the digit with hyperextension at the fracture
general. As more of the volar base of the middle pha- site, extensor lag of the interphalangeal joints, and ad-
Current Concepts
lanx is detached, the collateral ligaments no longer herence of flexor tendons.28
prevent the middle phalanx from moving dorsally.19,20
Extensive comminution may complicate treatment and Metacarpal fractures
require osteochondral bone grafting. A number of es- Fractures of the metacarpal neck are among the most
tablished surgical options exist for these injuries, al- common fractures of the hand. These so-called “box-
though none is clearly superior.21 Much new literature er’s” fractures are typically incurred by young men, not
exists, as well, regarding novel or modified treat- necessarily boxers, who strike a solid object with a
ment of PIP joint fracture dislocations. Any surgi- clenched fist.1 The fifth metacarpal neck is the most
JHS 䉬 Vol A, May
1026 HAND FRACTURES: CURRENT TREATMENT STRATEGIES
FIGURE 4: Dynamic external fixation technique for treatment of fractures at the base of the middle phalanx. Kirschner wires are
inserted in the distal proximal phalanx, proximal middle phalanx, and distal middle phalanx. Leverage on a longitudinal Kirschner
wire may be used to reduce the fracture. Rubber bands are configured to provide longitudinal traction. The interphalangeal joints
are free and may be moved.
vulnerable and most frequently injured. The fifth meta- splinting. Although the surgical group reported greater
carpal is also the most mobile bone of the palm and, satisfaction with the appearance of the hand, hands
therefore, especially tolerant of the typical apex-dorsal were functionally similar in both groups.36 Hofmeister
deformity. Whereas up to 70° of angulation may be et al37 have also recently challenged the dogma that the
compensated for in the fifth metacarpal, only 10° is fifth MCP joint must be immobilized in flexion. In a
tolerated in the second and third rays.1,31 The Jahss prospective, randomized trial involving young, active
reduction maneuver involves flexion of the MCP joint, patients, the authors showed equivalent results with
PIP joint, and DIP joint and use of the curled finger to volar-outrigger-type and extension short-arm casts.37
push the metacarpal head dorsally.32 Immobilization of Anterograde pinning of the fractured fifth metacarpal
boxer’s fractures may be beneficial; however, success- has been recently recommended as an alternative to
ful treatment without immobilization has been de- traditional retrograde fixation (Fig. 5).38
scribed.31 Nonsurgical intervention may be particularly Metacarpal shaft fractures may be transverse, in
appropriate in patients unlikely to return for follow- which case, like their boxer’s fracture counterpart, de-
up.33 formity is typically apex-dorsal. As in boxer’s fractures,
Surgery is reserved for cases in which an ade- surgery is indicated when an acceptable reduction can-
quate reduction of both angular and rotational de- not be maintained. Again, greater deformity is allowed
formity cannot be maintained or where an adjacent in the more mobile fourth and fifth rays. Spiral and
ray is damaged. High functional demand also is not oblique fractures are more unstable, and reduction must
necessarily an indication for surgery because even restore rotational alignment as a first priority. Mild
Current Concepts
with neglect, residual disability is typically negli- shortening encountered in spiral or oblique fractures
gible to none. Fixation with Kirschner wires either may be tolerated to a degree because hands with this
down the medullary canal or transversely to an deformity often overcome initial extensor lag and de-
uninjured ray are both effective treatment methods formity-related weakness.39 In general, metacarpal
in properly selected patients.34,35 shaft fractures are biologically splinted by the interpal-
According to the incidence of this fracture, much mar plate ligament (intermetacarpal ligaments) and in-
continues to be written regarding its management. Strub terosseous muscles (less so the second and fifth ray).
et al36 performed a prospective study in which patients The presence of fractures in adjacent ray(s) is a relative
with boxer’s fractures were treated conservatively and indication for surgery.
without reduction or with reduction and intramedullary A variety of surgical strategies exist, including plate-
JHS 䉬 Vol A, May
HAND FRACTURES: CURRENT TREATMENT STRATEGIES 1027
FIGURE 5: Retrograde Kirschner wire technique for fixation of distal metacarpal fractures. With the metacarpophalangeal (MCP)
joints in flexion, parallel (not shown) Kirschner wires are inserted retrograde into the metacarpal shaft and exit the skin dorsally at
the metacarpal base. Under fluoroscopy, the distal ends of the Kirschner wires are positioned in the metacarpal head. The wrist
and protruding Kirschner wires are flexed into extension.
screw constructs and intramedullary fixation.1 Rhee et care. Geometric deformity, conversely, is well toler-
al40 recently described a retrograde, intramedullary ated. The slightly deformed thumb has no parallel digit
splinting technique in which 1 or more wire ends are with which to interfere, and the thumb’s range of mo-
left out dorsally at the phalangeal base. The authors tion makes it additionally resistant to malunion.1 Typ-
report the ability to stabilize different fracture configu- ical apex-dorsal angular deformity of the metacarpal
rations with few complications.40 seen radiographically is often masked clinically by con-
Despite the ease with which intramedullary devices tours of the surrounding intrinsic muscles. Because of
are implanted, they are not foolproof. In a study com- the thumb’s oblique orientation with respect to the
paring plate and screw fixation with a percutaneous palm, radiographs need to be taken orthogonally to the
nailing technique, Ozer et al41 identified a number of thumb, the lateral with the thumbnail perpendicular to
complications in the intramedullary group: loss of re- the x-ray film, and either the posteroanterior or the
duction, joint penetration, tendon irritation, and symp- anteroposterior (Robert) view with the thumbnail par-
tomatic hardware. Fewer such complications were en- allel to the cassette.
countered with plate and screw constructs.41 Plate
fixation has been shown to be effective in cases of Phalanges
multiple metacarpal head fractures.42 Simple fractures of the thumb phalanges may be treated
Fracture dislocations of the metacarpal bases are like other phalanx fractures: gentle reduction is fol-
unusual, particularly at the more stable second and lowed by immobilization, in this case with a thumb
third carpometacarpal joints. When they do occur, spica splint. Safe splinting of the thumb holds all joints
they may be missed.10 They are typically unstable in extension and the thumb in abduction. When conser-
and require Kirschner wire stabilization. When vative measures fail, percutaneous fixation is usually
treatment is delayed, open reduction is often nec- appropriate. Rarely do simple fractures of the thumb
essary. Late arthritis of the fifth MCP joint is require open reduction and internal fixation. Bony mal-
exceedingly rare; however, arthrodesis of this joint let injuries to the thumb pose no unique problems.
is a theoretical solution.1 Intra-articular fractures of the thumb deserve special
attention. Fractures at the thumb MCP joint are likely to
Thumb fractures involve the collateral ligaments, and testing their integ-
Many thumb fractures are treated like finger fractures. rity is critical. An intact radial collateral ligament is
The thumb is distinct from the other digits, however, necessary for joint stability. Injury to the ulnar collateral
Current Concepts
and special consideration is due. The thumb’s unique ligament or its attachment to the base of the proximal
orientation gives the hand great capability and predis- phalanx (gamekeeper’s thumb), prevents effective
poses the thumb to certain injuries, particularly of the pinch and should be corrected. If reapproximation of
metacarpal base. Whereas adjacent fingers can compen- bony fragments is impossible or fails, debridement of
sate for one another, there is no surrogate for the thumb. bone with reinsertion of the ligament end is possible.
Likewise, there are few functions of the hand in which Arthrodesis of the thumb MCP joint, owing to the great
the thumb does not participate. Given these demands, range of motion at the thumb base, is an acceptable
intra-articular fractures of the thumb demand the utmost salvage procedure.1
JHS 䉬 Vol A, May
1028 HAND FRACTURES: CURRENT TREATMENT STRATEGIES
FIGURE 6: Tension-band technique for fixation of Bennett’s fractures. The fracture is reduced with distraction and pronation of
the thumb. Counterpressure from a clamp is applied while a Kirschner wire is passed across the fracture. A tension band is fixed
in a figure of eight.
First metacarpal (Fig. 6). They offered that the tension band allows for
Extra-articular fractures near the base of the thumb are compression at the fracture site and earlier motion than
common, and deforming forces are more complex here with Kirschner wires alone. An obligatory second sur-
than in other metacarpals. The abductor pollicis brevis, gery to remove hardware is a notable drawback.44 Used
adductor pollicis, and flexor pollicis brevis muscles flex with many fixation techniques, an arthroscope may help
the distal fragment, and the abductor pollicis longus ensure anatomical reduction of the basal joint.45
distracts and extends the proximal fragment. Mild de- Rolando fractures leave the shaft of the first meta-
formation of this sort is accommodated by the trapezio- carpal in an essentially anatomical position, but without
metacarpal joint, although excessive deformity forces bony connection to the basal joint. Surgical reduction
this joint into hyperextension. Closed reduction by vo- and fixation is required in most cases, but it may be
larly directed pressure on the fracture apex followed by difficult in these fractures that, by definition, are com-
percutaneous Kirschner wire fixation is useful when minuted. In these cases, external fixation is advanta-
angulation exceeds 30°.1 geous, and various configurations have been advocated.
Fracture dislocations at the base of the first metacar- Marshland et al46 have described a monolateral external
pal are known by 2 eponyms. Bennett fractures are fixation technique with good results.
avulsions of the ulnar metacarpal base. Rolando frac-
tures are impaction injuries in which both the ulnar and Severe and combined injuries
the radial elements of the thumb base are fractured from The hand may be severely traumatized in motor vehicle
the shaft. At the base of the thumb, the abductor pollicis or industrial accidents. Whether the skin is open or
longus tendon inserts radially and the deep anterior closed, compartment syndrome may develop, necessi-
oblique ligament inserts ulnarly. In Rolando fractures, tating fasciotomies and release of the carpal tunnel,
both of these soft tissue attachments are separated from either for existing symptoms or preemptively.47 Open
the shaft. fractures should be irrigated, covered, reduced where
Current Concepts
In Bennett fractures, the shaft is pulled proximally by possible, and immobilized.48 Antibiotic and tetanus
the intact abductor pollicis longus tendon. Given this prophylaxis may be administered on a case-by-case
deforming force, nonoperative treatment of Bennett basis. In addition to skin, tendons, vessels, nerves, and
fractures is frequently unsuccessful.43 Fractures with other soft tissue are often injured. Repair and recovery
less displacement may be reduced with longitudinal of these tissues is facilitated by a rigid underlying
traction and fixed with a Kirschner wire through the skeleton, and the doctrine of closed, conservative, frac-
trapezium, adjacent metacarpal, or both. More displace- ture care may be inapplicable. True rigidity is achieved
ment necessitates open reduction and internal fixation. with plate and screw constructs or an external fixator.
Zhang et al44 recently described a Kirschner wire and Locking plate and screw constructs may be used to fix
tension band technique for displaced Bennett fractures comminuted, metaphyseal, or osteoporotic bone. These
JHS 䉬 Vol A, May
HAND FRACTURES: CURRENT TREATMENT STRATEGIES 1029
invasive techniques are readily carried out in the setting ing surgical correction, and fracture through a pin track.
of open fractures that must be thoroughly washed out. Six percent of pins were complicated by superficial
Bannasch et al49 showed that postoperative infection infection. Infections were more likely in the metacar-
rates after open reduction and internal fixation of open pals and phalanges than they were in the wrist. Poor
and closed hand fractures are equally low. Despite the compliance with pin care was the only other reliable
necessity of more aggressive treatment in combined risk factor for infection. Notably, medical comorbidities
injuries, early movement, wherever feasible, remains did not increase rates of infection.52 Skin tension on a
the rule.3 Kirschner wire with repeated motion will lead to skin
necrosis and infection. Strategic choice of the Kirschner
Care of the healing fracture wire’s entry point through the skin, and sharp relief of
Early movement is once again emphasized. Uninvolved residual tension minimizes these problems.
rays should be unencumbered in order to encourage Cold intolerance is a known complication of hand
early use, and minimally stable parts (eg, reduced joint trauma in general, may linger long after the inciting
surfaces) should be moved when healing is sufficient to injury, and affects up to 38% of hand fracture pa-
resist displacement, typically at 2 to 3 weeks for me- tients.53 This complication may prompt questions of the
taphyseal bone. Pain should be aggressively managed, treating physician, and there are few good answers at
meaning the best modality at a given time should be present. Smits et al,54 using thermal imaging, identified
sought, if even reassurance and long courses of opioids no difference in rewarming patterns between previously
are avoided. A more comfortable patient has a psycho- fractured hands and their uninjured counterparts.
logical and physical reason to follow her or his doctor’s Even bony injuries that may seem trivial clinically
instructions. These instructions should be explained and radiographically may require many months for
clearly, and patients’ questions should be addressed. maximal recovery of soft tissue gliding, suppleness, and
Effective communication invests patients in their own comfort. Advising the patient of this pre-emptively al-
care, and this motivation is perhaps the most powerful lays anxiety and builds trust.
rehabilitative tool. In summary, fractures of the phalanges and
metacarpals are common and at least temporarily
COMPLICATIONS debilitating. They call attention to the hand’s great
Stiffness is a far more common and difficult to treat capability, vulnerability, and resilience. Most hand
complication of metacarpal and phalangeal fractures fractures may be treated without an operation;
than are malunion, nonunion, and arthrosis combined. however, conservative treatment must be exercised
Each of these complications may occur with or without with care and may in fact require greater skill and
an operation, and each is more easily prevented than sustained attention. Mobilization is vital to support
treated. Strictly surgical complications— hardware soft tissue healing, which is often more problem-
prominence, hardware infection, and wound break- atic than healing of underlying bone. In properly
down—are often primarily related to technique. Man- selected cases, surgery may speed recovery and
agement of complications lies on a broad spectrum avoid complications such as malunion and arthro-
from the simple to the complex. A comprehensive ac- sis. A variety of procedures offer either relative or
counting of these procedures is outside the scope of this absolute stability, the latter necessary only after
manuscript, and the reader is referred to more detailed more severe trauma. Postoperative care is at least
sources.1– 4 Several specific hand fracture complica- as important as the operation itself. Properly man-
tions have been addressed in recent literature and they aged, many fractured hands return essentially to
are presented later. normal—a relief to the patient and satisfaction to
In a small case series, Ozcelik et al50 described the his or her doctor.
successful treatment of distal phalanx nonunions with
Current Concepts
olecranon bone graft. Meijs et al51 have treated thumb REFERENCES
distal phalanx nonunions with a percutaneous compres-
1. Day C, Stern P. Fractures of the metacarpals and phalanges. In:
sion screw. Wolfe S, ed. Green’s Operative Hand Surgery. 6th ed. Philadelphia:
Hsu et al,52 in a review of 408 smooth Kirschner Elsevier Churchill Livingstone; 2011.
wires implanted for fractures of the hand and wrist, 2. Calandruccio J, Jobe M. Fractures, dislocations, and ligamentous
injuries. In: Canale S, Beaty J, eds. Campbell’s Operative Ortho-
identified few complications. Only 3% of pins were
paedics. 11th ed. Philadelphia: Mosby; 2008.
associated with a “major complication”: infection re- 3. Henry M. Hand fractures and dislocations. In: Bucholz R, Heckman
quiring surgical drainage, nonunion or malunion requir- J, Court-Brown C, Tornetta P, eds. Rockwood and Green’s Fractures
JHS 䉬 Vol A, May
1030 HAND FRACTURES: CURRENT TREATMENT STRATEGIES
in Adults. 7th ed. Philadelphia: Lippincott Williams & Wilkins; treatment of proximal interphalangeal joint fracture dislocations.
2010. Arch Orthop Trauma Surg. 2009;129(1):29 –37.
4. Jupiter J, Axelrod T, Belsky M. Fractures and dislocations of the 28. Ellis S, Cheng R, Prokopis P, et al. Treatment of proximal interpha-
hand. In: Browner B, Jupiter J, eds. Skeletal Trauma: Basic Science, langeal dorsal fracture-dislocation injuries with dynamic external
Management, and Reconstruction. 4th ed. Philadelphia: Saunders; fixation: a pins and rubber band system. J Hand Surg Am. 2007;
2009. 32(8):1242–1250.
5. Van Derelst E. Les debuts de l’osteosynthese en Belgique. Brussels: 29. Finsen V. Suzuki’s pins and rubber traction for fractures of the base
Societe Belge de Chirurgie Orthopedique et de Traumatologie, Im- of the middle phalanx. J Plast Surg Hand Surg. 2010;44(4 –5):209 –
primerie des Sciences; 1973. 213.
6. Lambotte A. Chirurgie: operatoire des fractures. Paris: Masson & 30. Hamada Y, Hibino N, Tonogai I, Konishi T, Satoura M, Yamano M.
Cie; 1913. Staged external fixation for chronic fracture-dislocation of the prox-
7. Harness N, Meals R. History of fracture fixation of the hand and imal interphalangeal joint: outcomes of patients with a minimum
wrist. Clin Orthop Relat Res. 2006;445:19 –29. 2-year follow-up. J Hand Surg Am. 2012;37(3):434 – 439.
8. Stanton J, Dias J, Burke F. Fractures of the tubular bones of the hand. 31. Statius Muller M, Poolman R, van Hoogstraten M, Steller E. Imme-
J Hand Surg Eur Vol. 2007;32(6):626 – 636. diate mobilization gives good results in boxer’s fractures with volar
9. Tuncer S, Aksu N, Dilek H, Ozkan T, Hamzaoglu A. Fractures of the angulation up to 70 degrees: a prospective randomized trial compar-
fingers missed or misdiagnosed on poorly positioned or poorly taken ing immediate mobilization with cast immobilization. Arch Orthop
radiographs: a retrospective study. J Trauma. 2011;71(3):649 – 655. Trauma Surg. 2003;123(10):534 –537.
10. Gaheer R, Ferdinand R. Fracture dislocation of carpometacarpal 32. Jahss S. Fractures of the metacarpals: a new method of reduction and
joints: a missed injury. Orthopedics. 2011;34(5):399. immobilization. J Bone Joint Surg Am. 1938;20(1):178 –186.
11. Chim H, Teoh L, Yong F. Open reduction and interfragmentary 33. ten Berg P, Ring D. Patients lost to follow-up after metacarpal
screw fixation for symptomatic nonunion of distal phalangeal frac- fractures. J Hand Surg Am. 2012;37(1):42– 46.
tures. J Hand Surg Eur Vol. 2008;33(1):71–76. 34. Beredjiklian P. Small finger metacarpal neck fractures. J Hand Surg
12. Henry M. Variable pitch headless compression screw treatment of Am. 2009;34(8):1524 –1526.
distal phalangeal nonunions. Tech Hand Up Extrem Surg. 2010; 35. Mohammed R, Farook M, Newman K. Percutaneous elastic in-
14(4):230S–233S. tramedullary nailing of metacarpal fractures: surgical technique and
13. Lucchina S, Badia A, Dornean V, Fusetti C. Unstable mallet frac- clinical results study. J Orthop Surg Res. 2011;6:37.
tures: a comparison between three different techniques in a multi- 36. Strub B, Schindele S, Sonderegger J, Sproedt J, von Campe A,
center study. Chin J Traumatol. 2010;13(4):195–200. Gruenert J. Intramedullary splinting or conservative treatment for
14. Lee S, Kim K, Yang D, Moon K, Choy W. Modified extension-block displaced fractures of the little finger metacarpal neck? A prospec-
K-wire fixation technique for the treatment of bony mallet finger. tive study. J Hand Surg Eur Vol. 2010;35(9):725–729.
Orthopedics. 2010;33(10):728. 37. Hofmeister E, Kim J, Shin A. Comparison of 2 methods of immo-
15. Lee S, Kim H, Lee K, Kim K, Choy W. Modified pull-out wire bilization of fifth metacarpal neck fractures: a prospective random-
suture technique for the treatment of chronic bony mallet finger. Ann ized study. J Hand Surg Am. 2008;33(8):1362–1368.
Plast Surg. 2010;65(5):466 – 470. 38. Schädel-Höpfner M, Wild M, Windolf J, Linhart W. Antegrade
16. Tuttle H, Olvey S, Stern P. Tendon avulsion injuries of the distal intramedullary splinting or percutaneous retrograde crossed pinning
phalanx. Clin Orthop Relat Res. 2006;445:157–168. for displaced neck fractures of the fifth metacarpal? Arch Orthop
17. Figl M, Weninger P, Hofbauer M, Pezzei C, Schauer J, Leixnering Trauma Surg. 2007;127(6):435– 440.
M. Results of dynamic treatment of fractures of the proximal phalanx 39. Al-Qattan M. Outcome of conservative management of spiral/long
of the hand. J Trauma. 2011;70(4):852– 856. oblique fractures of the metacarpal shaft of the fingers using a palmar
18. Tan J, Foo A, Chew W, Teoh L. Articularly placed interfragmentary wrist splint and immediate mobilisation of the fingers. J Hand Surg
screw fixation of difficult condylar fractures of the hand. J Hand Eur Vol. 2008;33(6):723–727.
Surg Am. 2011;36(4):604 – 609. 40. Rhee S, Lee S, Lee S, Kim J, Baek G, Lee Y. Prospective multicenter
19. Dias J. Intraarticular injuries of the distal and proximal interphalan- trial of modified retrograde percutaneous intramedullary Kirschner
geal joints. In: Berger R, Weiss A, eds. Hand Surgery. 1st ed. wire fixation for displaced metacarpal neck and shaft fractures. Plast
Philadelphia: Lippincott Williams & Wilkins; 2004. Reconstr Surg. 2012;129(3):694 –703.
20. Vitale M, White N, Strauch R. A percutaneous technique to treat 41. Ozer K, Gillani S, Williams A, Peterson S, Morgan S. Compar-
unstable dorsal fracture-dislocations of the proximal interphalangeal ison of intramedullary nailing versus plate-screw fixation of ex-
joint. J Hand Surg Am. 2011;36(9):1453–1459. tra-articular metacarpal fractures. J Hand Surg Am. 2008;33(10):
21. McAuliffe J. Dorsal fracture dislocation of the proximal interpha- 1724 –1731.
langeal joint. J Hand Surg Am. 2008;33(10):1885–1888. 42. Souer J, Mudgal C. Plate fixation in closed ipsilateral multiple
22. Kiefhaber T, Stern P. Fracture dislocations of the proximal inter- metacarpal fractures. J Hand Surg Eur Vol. 2008;33(6):740 –744.
pahlangeal joint. J Hand Surg Am. 1998;23(3):369 –380. 43. Livesley P. The conservative management of Bennetts fracture sub-
23. Cheah A, Tan D, Chong A, Chew W. Volar plating for unstable luxation: a 26-year follow-up. J Hand Surg Br. 1990;15(3):291–294.
Current Concepts
proximal interphalangeal joint dorsal fracture-dislocations. J Hand 44. Zhang X, Shao X, Zhang Z, Wen S, Sun J, Wang B. Treatment of a
Surg Am. 2012;37(1):28 –33. Bennett fracture using tension band wiring. J Hand Surg Am. 2012;
24. Waris E, Alanen V. Percutaneous, intramedullary fracture reduction 37(3):427– 433.
and extension block pinning for dorsal proximal interphalangeal 45. Culp R, Johnson J. Arthroscopically assisted percutaneous fixation
fracture-dislocations. J Hand Surg Am. 2010;35(12):2046 –2052. of Bennett fractures. J Hand Surg Am. 2010;35(1):137–140.
25. Körting O, Facca S, Diaconu M, Liverneaux P. Treatment of com- 46. Marsland D, Sanghrajka A, Goldie B. Static monolateral external
plex proximal interphalangeal joint fractures using a new dynamic fixation for the Rolando fracture: a simple solution for a complex
external fixator: 15 cases. Chir Main. 2009;28(3):153–157. fracture. Ann R Coll Surg Engl. 2012;94(2):112–115.
26. Ruland R, Hogan C, Cannon D, Slade J. Use of dynamic distraction 47. Al-Qattan M. The triad of multiple metacarpal fractures and/or
external fixation for unstable fracture-dislocations of the proximal dislocations of the fingers, severe hand swelling and clinical evi-
interphalangeal joint. J Hand Surg Am. 2008;33(1):19 –25. dence of acute median nerve dysfunction. J Hand Surg Eur Vol.
27. Kneser U, Goldberg E, Polykandriotis E, et al. Biomechanical and 2008;33(3):298 –304.
functional analysis of the pins and rubbers tractions system for 48. Capo J, Hall M, Nourbakhsh A, Tan V, Henry P. Initial management
JHS 䉬 Vol A, May
HAND FRACTURES: CURRENT TREATMENT STRATEGIES 1031
of open hand fractures in an emergency department. Am J Orthop fracture: treatment with a percutaneous compression screw. J Hand
(Belle Mead NJ). 2011;40(12):E243–E248. Surg Am. 2009;34(6):1127–1129.
49. Bannasch H, Heermann A, Iblher N, Momeni A, Schulte-Mönting J, 52. Hsu L, Schwartz E, Kalainov D, Chen F, Makowiec R. Complica-
Stark G. Ten years stable internal fixation of metacarpal and pha- tions of K-wire fixation in procedures involving the hand and wrist.
langeal hand fractures-risk factor and outcome analysis show no J Hand Surg Am. 2011;36(4):610 – 616.
increase of complications in the treatment of open compared with 53. Nijhuis T, Smits E, Jaquet J, Van Oosterom F, Selles R, Hovius S.
closed fractures. J Trauma. 2010;68(3):624 – 628. Prevalence and severity of cold intolerance in patients after hand
50. Ozçelik I, Kabakas F, Mersa B, Purisa H, Sezer I, Ertürer E. fracture. J Hand Surg Eur Vol. 2010;35(4):306 –311.
Treatment of nonunions of the distal phalanx with olecranon bone 54. Smits E, Nijhuis T, Huygen F, Selles R, Hovius S, Niehof S.
graft. J Hand Surg Eur Vol. 2009;34(5):638 – 642. Rewarming patterns in hand fracture patients with and without cold
51. Meijs C, Verhofstad M. Symptomatic nonunion of a distal phalanx intolerance. J Hand Surg Am. 2011;36(4):670 – 676.
JOURNAL CME QUESTIONS
Hand Fractures: A Review of Current How many degrees are compensated for in index
Treatment Strategies finger metacarpal neck fractures?
a. 10
Which of the following is appropriate in
b. 20
nonoperative treatment of hand fractures?
c. 50
a. Fiberglass is better for holding fracture reduction
than molded plaster. d. 70
b. Manipulation is aided by flexion of the metacar- e. 100
pophalangeal and wrist joints.
c. Immobilization of the wrist should be in flex-
ion.
d. A splint should maintain the metacarpophalangeal
joint in neutral position.
e. Hand fractures are not aided by nerve blocks.
To take the online test and receive CME credit, go to http://www.jhandsurg.org/CME/home.
Current Concepts
JHS 䉬 Vol , May
You might also like
- Suh 2013Document3 pagesSuh 2013Juan HoyosNo ratings yet
- 2013 Prevention and Treatment of Elbow StiffnessDocument12 pages2013 Prevention and Treatment of Elbow StiffnessGajendra ShahNo ratings yet
- Physical Examination of The Hand: Cme Information and DisclosuresDocument11 pagesPhysical Examination of The Hand: Cme Information and DisclosuresDesrainy InhardiniNo ratings yet
- Pi Is 0363502321003075Document7 pagesPi Is 0363502321003075Deborah SalinasNo ratings yet
- Elbow Instability Anatomy BiomechanicsDocument9 pagesElbow Instability Anatomy BiomechanicsSPerOrtNo ratings yet
- Management Thumb Tip Injuries - Germann - JHS 2015Document9 pagesManagement Thumb Tip Injuries - Germann - JHS 2015Professeur Christian DumontierNo ratings yet
- Complex Injuries of The HandDocument285 pagesComplex Injuries of The HandWilson A. Quintero100% (1)
- 4-12-23 Trauma - 2Document18 pages4-12-23 Trauma - 2anateresalopez271No ratings yet
- Crista Udo 2016Document12 pagesCrista Udo 2016Allison DiêgoNo ratings yet
- Penetrating Duodenal Trauma: A 19-Year Experience: AAST Continuing Medical Education ArticleDocument5 pagesPenetrating Duodenal Trauma: A 19-Year Experience: AAST Continuing Medical Education ArticleLaiz DecampsNo ratings yet
- Sample Journal Review PaperDocument14 pagesSample Journal Review PaperWharren DañoNo ratings yet
- Ta 86 722Document15 pagesTa 86 722Pratama InsaniNo ratings yet
- Surgical ConscienceDocument2 pagesSurgical ConscienceRPMFA RPMFANo ratings yet
- NB - Systematic Approach To The Management of Post-Traumatic Segmental Diaphyseal Long Bone Defect - NandoDocument12 pagesNB - Systematic Approach To The Management of Post-Traumatic Segmental Diaphyseal Long Bone Defect - NandoSerenna DehalooNo ratings yet
- 2011 JAAD Vitiligo A Comprehensive OverviewDocument22 pages2011 JAAD Vitiligo A Comprehensive OverviewGOURINANDHANo ratings yet
- Perilunate Dislocations: Cme Information and DisclosuresDocument5 pagesPerilunate Dislocations: Cme Information and DisclosuresClaudio LimaNo ratings yet
- A Protocol For The Management of Adhesive Small Bowel ObstructionDocument9 pagesA Protocol For The Management of Adhesive Small Bowel ObstructiontanyasisNo ratings yet
- Arm ContouringDocument11 pagesArm ContouringfumblefumbleNo ratings yet
- Kozar 2018Document4 pagesKozar 2018DH SiriruiNo ratings yet
- Zhang 2020Document8 pagesZhang 2020Viviana GeraldinNo ratings yet
- Perioperative Safety Culture Principles, PracticeDocument3 pagesPerioperative Safety Culture Principles, PracticeShakira Fe RodrigoraNo ratings yet
- Guideline 2013 Breast Recon Expanders ImplantsDocument23 pagesGuideline 2013 Breast Recon Expanders ImplantsBogdan TudorNo ratings yet
- Articulo en InglesDocument10 pagesArticulo en InglesLaura Cristina Sierra FuentesNo ratings yet
- Hand Burns: Karen J. Kowalske, MD, David G. Greenhalgh, MD, Scott R. Ward, PHD, PTDocument4 pagesHand Burns: Karen J. Kowalske, MD, David G. Greenhalgh, MD, Scott R. Ward, PHD, PTsantizptNo ratings yet
- WTACriticalDecisionsEsophagealInjuries PDFDocument7 pagesWTACriticalDecisionsEsophagealInjuries PDFprekos 65No ratings yet
- Medicamentos Na GravidezDocument14 pagesMedicamentos Na GravidezOdilon MangeronaNo ratings yet
- Gravidez e Medicamentos Parte 2 JaadDocument10 pagesGravidez e Medicamentos Parte 2 JaadMarcia ZampeseNo ratings yet
- Official JTACS Lethal DiamondDocument6 pagesOfficial JTACS Lethal DiamondMileidys LopezNo ratings yet
- Trauma Surgery and Acute Care Surgery: Evolution in The Eye of The StormDocument3 pagesTrauma Surgery and Acute Care Surgery: Evolution in The Eye of The StormDeddy WidjajaNo ratings yet
- Journal Orthopedi 3Document5 pagesJournal Orthopedi 3Nur SulistiyaningsihNo ratings yet
- Fractura Radio Distal ReviewDocument5 pagesFractura Radio Distal ReviewUn SerNo ratings yet
- Hickson 2018Document12 pagesHickson 2018Luigi Paolo Zapata DelgadoNo ratings yet
- Melasma: A Comprehensive Update: Ontinuing Medical EducationDocument9 pagesMelasma: A Comprehensive Update: Ontinuing Medical EducationHugh MantaNo ratings yet
- Classification of Non-Union Scoring Disc Calori2008Document5 pagesClassification of Non-Union Scoring Disc Calori2008KlausNo ratings yet
- Guía Hemorragia Intestino DelgadoDocument8 pagesGuía Hemorragia Intestino DelgadoSMIBA MedicinaNo ratings yet
- Rushton 2014Document7 pagesRushton 2014Martín Seijas GonzálezNo ratings yet
- Complicationsoffracturehealing AReviewDocument9 pagesComplicationsoffracturehealing AReviewMuhamad vero SyatiaNo ratings yet
- Final AcrDocument30 pagesFinal AcrAnaLauraJiménezNo ratings yet
- 10 1002@aorn 12722Document10 pages10 1002@aorn 12722Francisco NenteNo ratings yet
- SJX 218Document11 pagesSJX 218Equipo AsoinmedNo ratings yet
- Management of Fingertip Injuries: A Survey of Opinions of Surgeons WorldwideDocument7 pagesManagement of Fingertip Injuries: A Survey of Opinions of Surgeons Worldwidefadhil03No ratings yet
- Cervical Spine Clearance - Inaba Trauma and Acute Care - 2016Document9 pagesCervical Spine Clearance - Inaba Trauma and Acute Care - 2016Simon HendelNo ratings yet
- Safe Patient HandlingDocument2 pagesSafe Patient Handlingapi-3697326No ratings yet
- Belcher2016 (1) - 2Document10 pagesBelcher2016 (1) - 2msl497No ratings yet
- Critical Role of The Surgeon-Anesthesiologist Relationship For Patient SafetyDocument4 pagesCritical Role of The Surgeon-Anesthesiologist Relationship For Patient SafetyPablo Segales BautistaNo ratings yet
- Design Principles For Health WearablesDocument11 pagesDesign Principles For Health WearablesIgnacio NolascoNo ratings yet
- The SAGES Manual of Quality, Outcomes and Patient SafetyDocument1,006 pagesThe SAGES Manual of Quality, Outcomes and Patient SafetyAngelita Flores LizárragaNo ratings yet
- Changing The Work Environment inDocument8 pagesChanging The Work Environment inKassiani LavidaNo ratings yet
- 10 1016@j JHT 2020 03 024Document10 pages10 1016@j JHT 2020 03 024eduar yecid duarte gomezNo ratings yet
- Kassir 2021Document10 pagesKassir 2021kwpang1No ratings yet
- Identifying Factors That Inhibit Self-Care Behavior Among Individuals With Severe Spinal Cord InjuryDocument16 pagesIdentifying Factors That Inhibit Self-Care Behavior Among Individuals With Severe Spinal Cord Injurydemi84No ratings yet
- LSM 23201Document21 pagesLSM 23201juan carlos pradaNo ratings yet
- Nonsurgical Management of Facial Masculinization and Feminization PDFDocument15 pagesNonsurgical Management of Facial Masculinization and Feminization PDFImanuel CristiantoNo ratings yet
- Quality of Care Before, During, and After Casting: A Cross-Sectional StudyDocument7 pagesQuality of Care Before, During, and After Casting: A Cross-Sectional StudyChristian SierNo ratings yet
- WTA 2019 - Evaluation and Management of Abdominal Gunshot WoundsDocument8 pagesWTA 2019 - Evaluation and Management of Abdominal Gunshot WoundsKevin QuinterosNo ratings yet
- Medical CannabisDocument6 pagesMedical CannabisJUAN JOSE BOTIA NARANJONo ratings yet
- MELASMAsheth 2011Document16 pagesMELASMAsheth 2011luanareichertNo ratings yet
- High Definition Body Sculpting ArtDocument2 pagesHigh Definition Body Sculpting ArtmdwilliamsNo ratings yet
- Effectiveness of Edema Management Techniques For Subacute Hand EdemaDocument14 pagesEffectiveness of Edema Management Techniques For Subacute Hand EdemaRiky SetyawanNo ratings yet
- Ow Pakistan Offers Quota For Kashmiri Students Geelani S Resignation From HurriyatDocument21 pagesOw Pakistan Offers Quota For Kashmiri Students Geelani S Resignation From HurriyatABHINAV DEWALIYANo ratings yet
- What Is Subject Verb AgreementDocument3 pagesWhat Is Subject Verb AgreementMarkNo ratings yet
- Software Development Plan TemplateDocument5 pagesSoftware Development Plan TemplateArvada Solutions0% (1)
- Report On Descriptive Statistics and Item AnalysisDocument21 pagesReport On Descriptive Statistics and Item Analysisapi-3840189100% (1)
- Hypothesis Test - Difference in MeansDocument4 pagesHypothesis Test - Difference in Meansr01852009paNo ratings yet
- Tutorial Sheet Unit V 3Document3 pagesTutorial Sheet Unit V 3rakesh507No ratings yet
- Chapter - Motivation: Md. Imran Hossain Assistant Professor Dept: of Finance Jagannath UniversityDocument43 pagesChapter - Motivation: Md. Imran Hossain Assistant Professor Dept: of Finance Jagannath Universityjh shuvoNo ratings yet
- Public Policy PDFDocument525 pagesPublic Policy PDFMutemwa Emmanuel Tafira93% (15)
- Impact of Bread and Pastry Production To Senior High School Student of Baclayon National High School 1Document60 pagesImpact of Bread and Pastry Production To Senior High School Student of Baclayon National High School 1Joanna Mari HubacNo ratings yet
- Lesson PlanDocument8 pagesLesson PlanMarvi Joyce Caballero100% (1)
- Fundamentals of Accounting 1 (Week 4) OnlineDocument14 pagesFundamentals of Accounting 1 (Week 4) OnlineElla Blanca BuyaNo ratings yet
- Minutes of Meeting Class Schedule Parents Orientation LAC Plan and School Recovery Learning PLan August 17 2022Document5 pagesMinutes of Meeting Class Schedule Parents Orientation LAC Plan and School Recovery Learning PLan August 17 2022Janette BolanteNo ratings yet
- Assesel 1 First MeetingDocument10 pagesAssesel 1 First MeetingNORALYN VELASCONo ratings yet
- Fundamentals of Digital MarketingDocument6 pagesFundamentals of Digital Marketingsajjad sharifNo ratings yet
- Files/keplers - Laws - Es - PDF: Kepler Activity SourceDocument5 pagesFiles/keplers - Laws - Es - PDF: Kepler Activity SourceREGINA SANTIAGONo ratings yet
- Hnology and Livelihood Education: Quarter 1 - Module 3: CookeryDocument28 pagesHnology and Livelihood Education: Quarter 1 - Module 3: CookeryDomeng Karo100% (2)
- SPS 143 Psychology 3 (Question and Answer)Document10 pagesSPS 143 Psychology 3 (Question and Answer)Qistina ShahrilNo ratings yet
- Aliaga National High School Poblacion East II, Aliaga, Nueva EcijaDocument3 pagesAliaga National High School Poblacion East II, Aliaga, Nueva EcijaSarah RiveraNo ratings yet
- Timeline Thesis ProposalDocument6 pagesTimeline Thesis Proposalafknufgbn100% (1)
- Rochester College Lesson Plan TemplateDocument14 pagesRochester College Lesson Plan Templateapi-348350634No ratings yet
- Exam DLLDocument2 pagesExam DLLlalhang47No ratings yet
- Grammatical Competence and Models of L2 LearningDocument11 pagesGrammatical Competence and Models of L2 LearningMorten Oddvik100% (6)
- Egyptian ArabicDocument2 pagesEgyptian ArabicIyesusgetanewNo ratings yet
- English ProjectDocument15 pagesEnglish Projectpranit.saluja.ps.2324No ratings yet
- Healthmeans 20 Ways To Build Resilience UpdatedDocument23 pagesHealthmeans 20 Ways To Build Resilience UpdatedSofia BouçadasNo ratings yet
- English 9 Q4 Module 2Document30 pagesEnglish 9 Q4 Module 2Karla Javier Padin60% (5)
- Work Load Distribution-2016Document11 pagesWork Load Distribution-2016Sindh Jobs HelperNo ratings yet
- Lesson Plan For EnglishDocument8 pagesLesson Plan For EnglishNOOR AZNINo ratings yet
- Craap Test WorksheetDocument5 pagesCraap Test Worksheetapi-272946391No ratings yet
- University of Vermont Diversity and Inclusion Action Plan SurveyDocument17 pagesUniversity of Vermont Diversity and Inclusion Action Plan SurveyThe College FixNo ratings yet