You might also like
- Medication - Chart ADHD PDFDocument2 pagesMedication - Chart ADHD PDFaayceeNo ratings yet
- Swedish Massage InfoDocument5 pagesSwedish Massage InfoJoy CelestialNo ratings yet
- 9 New Auto Loan Application Form 2019Document3 pages9 New Auto Loan Application Form 2019RenanNo ratings yet
- (Mebooksfree Net) Ric&vas&tra&ras&tai&3rd PDFDocument416 pages(Mebooksfree Net) Ric&vas&tra&ras&tai&3rd PDFAlexandru ChiriacNo ratings yet
- Empowerment Technologies: Quarter 1 - Module 2: NetiquettesDocument20 pagesEmpowerment Technologies: Quarter 1 - Module 2: NetiquettesClark Domingo86% (7)
- TFOE Members Application FormDocument4 pagesTFOE Members Application FormAndrei Dizon100% (1)
- Mobility and ImmobilityDocument37 pagesMobility and ImmobilityAndrea Huecas Tria100% (2)
- Reading The Brain by Caroline MarkolinDocument2 pagesReading The Brain by Caroline MarkolinCoraKiri100% (1)
- ABG Interpretation 3.0Document73 pagesABG Interpretation 3.0Jesus Mario Lopez100% (1)
- Rmu Surgery OspesDocument110 pagesRmu Surgery OspesHumna YounisNo ratings yet
- Local Government Unit: Photo 2 X 2Document1 pageLocal Government Unit: Photo 2 X 2Alexis Brian BrionesNo ratings yet
- Philhealth Identification Number (Pin) Important Reminders:: PurposeDocument3 pagesPhilhealth Identification Number (Pin) Important Reminders:: PurposeMhelaril AnneNo ratings yet
- MSI Application Form (ANTIDO)Document7 pagesMSI Application Form (ANTIDO)Raboni AntidoNo ratings yet
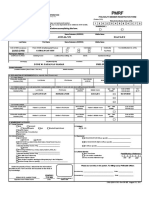
- PMRF - Final 2019Document2 pagesPMRF - Final 2019Silverghost Sun Dance Studio82% (17)
- Bryan Sundo MDRDocument1 pageBryan Sundo MDRDeanna GarciaNo ratings yet
- Fish R FormDocument1 pageFish R Formlibertygavarra1No ratings yet
- Member Data RecordDocument1 pageMember Data RecordTahinay KarlNo ratings yet
- Po1 Recruitment Application Form: Celedonio Joseph Gregorio Iguirindon San Remigo, Antique,, ANTIQUE, Region VI 5714Document1 pagePo1 Recruitment Application Form: Celedonio Joseph Gregorio Iguirindon San Remigo, Antique,, ANTIQUE, Region VI 5714Dark AngelNo ratings yet
- PhilHelath MDRDocument1 pagePhilHelath MDRDeanna GarciaNo ratings yet
- De Luna Heinrich Theraja Recaña - MDRDocument1 pageDe Luna Heinrich Theraja Recaña - MDROcir TenorioNo ratings yet
- Form MemberapplicationDocument3 pagesForm MemberapplicationRiannaNo ratings yet
- Langcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormDocument10 pagesLangcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormPaHm Iglesias LeeNo ratings yet
- Assessment Tool For ElderlyDocument4 pagesAssessment Tool For ElderlySheinna DuranNo ratings yet
- PMRF 012020Document2 pagesPMRF 012020Mam BoyNo ratings yet
- SET 2 TCAA 2021 DepEd Forms Above P500K and Autonomous v1.0Document14 pagesSET 2 TCAA 2021 DepEd Forms Above P500K and Autonomous v1.0Aynrand SalvadorNo ratings yet
- Lim, AntonioDocument4 pagesLim, AntonioJamika ReyesNo ratings yet
- Llanita, JulianDocument1 pageLlanita, JulianDonna Dela CruzNo ratings yet
- EPaycard - Customer Account Opening Form - 2015Document1 pageEPaycard - Customer Account Opening Form - 2015Drw ArcyNo ratings yet
- RAF Febie PDFDocument1 pageRAF Febie PDFFebie Cleni ArevaloNo ratings yet
- Application Form: Photo 1 X 1Document2 pagesApplication Form: Photo 1 X 1AlejoRaquelNo ratings yet
- Member Data Record: Philippine Health Insurance CorporationDocument1 pageMember Data Record: Philippine Health Insurance CorporationJonjie MiladoNo ratings yet
- Member Data Record: Mijares, Sheryl CasimeroDocument1 pageMember Data Record: Mijares, Sheryl CasimeroSheryl MijaresNo ratings yet
- PRF For PWDDocument1 pagePRF For PWDCarla MarianoNo ratings yet
- Reyes, Jamika Antonette P.Document4 pagesReyes, Jamika Antonette P.Jamika ReyesNo ratings yet
- MDR 080508446768 PDFDocument1 pageMDR 080508446768 PDFJeycel LubuguinNo ratings yet
- Membership Update Form PICPADocument2 pagesMembership Update Form PICPAJennilyn HenaresNo ratings yet
- ISIP Application Form 2020Document1 pageISIP Application Form 2020subyNo ratings yet
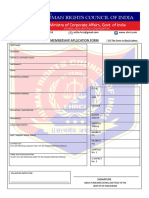
- Membership Apllication FormDocument1 pageMembership Apllication FormSuvamNo ratings yet
- MDR 190898891708Document1 pageMDR 190898891708mj digitalNo ratings yet
- MDR 030267636601Document1 pageMDR 030267636601enconicaNo ratings yet
- MDR 010256550690Document1 pageMDR 010256550690mathhew bepplerNo ratings yet
- Know Your Client (KYC) Application Form (For Individuals Only) Application No.Document1 pageKnow Your Client (KYC) Application Form (For Individuals Only) Application No.RamaseshuNo ratings yet
- Information Form: Maldives Islamic BankDocument5 pagesInformation Form: Maldives Islamic BankyrafeeuNo ratings yet
- Buyer Info Sheet 1Document1 pageBuyer Info Sheet 1api-636430593No ratings yet
- Po1 Recruitment Application Form: Gonsay Jonathan Binwag P-3 Gabriela Silang, DIFFUN, QUIRINO, Region II 3401Document1 pagePo1 Recruitment Application Form: Gonsay Jonathan Binwag P-3 Gabriela Silang, DIFFUN, QUIRINO, Region II 3401Hahak DougNo ratings yet
- MDR 112526338920Document1 pageMDR 112526338920JOSEPH PUASANNo ratings yet
- Modified KRA SBIsmartDocument1 pageModified KRA SBIsmartShiftinchargeengineer dadri coal0% (1)
- MSWD Form IIDocument3 pagesMSWD Form IIDanicaNo ratings yet
- Member Data Record: de Lara, Bianca Jesmine AlcantaraDocument1 pageMember Data Record: de Lara, Bianca Jesmine AlcantaraaliannaNo ratings yet
- BPLO - Application Form For Occupational Permit Revised 07012022 1 - EditableDocument1 pageBPLO - Application Form For Occupational Permit Revised 07012022 1 - EditableLeofred LozanoNo ratings yet
- MDR 150503604622Document1 pageMDR 150503604622Deanna GarciaNo ratings yet
- MDR 212506714262Document1 pageMDR 212506714262Charilyn SaragaNo ratings yet
- UPDATED CIF Jul 2021 SAMPLE ONLYDocument2 pagesUPDATED CIF Jul 2021 SAMPLE ONLYChristine Anne PostradoNo ratings yet
- Member Data Record: Medalla, Aileen TamayoDocument1 pageMember Data Record: Medalla, Aileen TamayoGerald Manaig PaquiaNo ratings yet
- QF Maf 171 Professional Staff Application PDFDocument7 pagesQF Maf 171 Professional Staff Application PDFAJNCNo ratings yet
- MDR EncaboDocument1 pageMDR EncabobernelencaboNo ratings yet
- Loan-Application Pahiram12 PDFDocument1 pageLoan-Application Pahiram12 PDFKim CarloNo ratings yet
- MDR 020275418111Document1 pageMDR 020275418111Christian BitoyNo ratings yet
- Non-Immigrant Visa - Review Personal, Address, Phone, and Passport InformationDocument2 pagesNon-Immigrant Visa - Review Personal, Address, Phone, and Passport InformationCesar RosaNo ratings yet
- MDR 082531799263Document1 pageMDR 082531799263eric zozobradoNo ratings yet
- Non-Immigrant Visa - Review Personal, Address, Phone, and Passport InformationDocument2 pagesNon-Immigrant Visa - Review Personal, Address, Phone, and Passport InformationTie PereiraNo ratings yet
- Vargas, Santa - DS160 Pag.1Document2 pagesVargas, Santa - DS160 Pag.1Kelly VargasNo ratings yet
- MDR 130252308475Document1 pageMDR 130252308475Joseroy RosaupanNo ratings yet
- B. Finance - Q1-Week 6-8 - AssignmentDocument6 pagesB. Finance - Q1-Week 6-8 - AssignmentBrix AguasonNo ratings yet
- Random Variables Probability DistributionsDocument23 pagesRandom Variables Probability DistributionsBrix AguasonNo ratings yet
- Brix Aguason Abm 2: Activity 1: Reaction PleaseDocument4 pagesBrix Aguason Abm 2: Activity 1: Reaction PleaseBrix AguasonNo ratings yet
- The Dust in Your Place: ClaireDocument9 pagesThe Dust in Your Place: ClaireBrix AguasonNo ratings yet
- Character Trait ExamplesDocument4 pagesCharacter Trait ExamplesPatricia Anne Nicole Cuaresma100% (1)
- 06 LCD Slides 1Document39 pages06 LCD Slides 1Brix AguasonNo ratings yet
- Sample! Sample!: Property of STI Weeks 7 - 9 SH1923Document26 pagesSample! Sample!: Property of STI Weeks 7 - 9 SH1923Brix AguasonNo ratings yet
- Property of STI Weeks 5 - 6 SH1923Document21 pagesProperty of STI Weeks 5 - 6 SH1923Brix AguasonNo ratings yet
- Sample! Sample!: Property of STI Weeks 7 - 9 SH1923Document26 pagesSample! Sample!: Property of STI Weeks 7 - 9 SH1923Brix AguasonNo ratings yet
- The Scoring Clinical Index For OnychomycosisDocument4 pagesThe Scoring Clinical Index For OnychomycosisPatricia Avalos C.No ratings yet
- Glossary and Acronyms of FreedivingDocument2 pagesGlossary and Acronyms of FreedivingIvo XNo ratings yet
- PhysioEx Exercise 7 Activity 1Document6 pagesPhysioEx Exercise 7 Activity 1Jorge CuevaNo ratings yet
- Respiratory Best RDocument5 pagesRespiratory Best RfrabziNo ratings yet
- Daftar Sampel ReadyDocument6 pagesDaftar Sampel ReadydindaNo ratings yet
- Clincal Trial Sun PharmaDocument2 pagesClincal Trial Sun PharmaChitresh MotwaniNo ratings yet
- AMG Curs 3Document2 pagesAMG Curs 3Maria PalNo ratings yet
- Examination of A Case of Ctev PDFDocument3 pagesExamination of A Case of Ctev PDFAnkit KarkiNo ratings yet
- Methodist Dallas Medical Center ExpansionDocument6 pagesMethodist Dallas Medical Center ExpansionrappletonNo ratings yet
- In Favour of An Investigation of The Relationship Between Vitamin B12 Deficiency and HIV InfectionDocument3 pagesIn Favour of An Investigation of The Relationship Between Vitamin B12 Deficiency and HIV InfectionPJ 123No ratings yet
- Iem India Perspective N B Kumta MaharashtraDocument8 pagesIem India Perspective N B Kumta Maharashtraavijitcu2007No ratings yet
- Herpesviruses, Poxviruses & Human Papilloma Virus: Fort SalvadorDocument33 pagesHerpesviruses, Poxviruses & Human Papilloma Virus: Fort SalvadorFort SalvadorNo ratings yet
- Macrophages - A Review of Their Role in Wound Healing and Their Therapeutic UseDocument17 pagesMacrophages - A Review of Their Role in Wound Healing and Their Therapeutic UseklaumrdNo ratings yet
- What It Takes To Be A Doctor?Document11 pagesWhat It Takes To Be A Doctor?Marion YaoNo ratings yet
- Psychiatric Nursing KaplanDocument27 pagesPsychiatric Nursing KaplanrochmahNo ratings yet
- Irna - Existing RS Type DDocument17 pagesIrna - Existing RS Type DUcrit TralalaNo ratings yet
- Traumatic Ulcerative Granuloma With Stromal Eosinophilia: Case ReportDocument4 pagesTraumatic Ulcerative Granuloma With Stromal Eosinophilia: Case ReportFandy MuhammadNo ratings yet
- 2023 Ada Diabete Standards of Care in Diabetes Diab CareDocument16 pages2023 Ada Diabete Standards of Care in Diabetes Diab CareJ Cristian Martinez RodríguezNo ratings yet
- Physician CertificationDocument1 pagePhysician CertificationcwadotorgNo ratings yet
- The Direct Antiglobulin Test: Indications, Interpretation, and PitfallsDocument6 pagesThe Direct Antiglobulin Test: Indications, Interpretation, and Pitfallsabbhyasa5206No ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- Thyroid Disease Anesthetic ConsiderationsDocument30 pagesThyroid Disease Anesthetic ConsiderationsmirzaoctaNo ratings yet
- Body Mechanics and Positioning: Health Assessment' (NCM 101) Skills Mr. Jhonee F. BalmeoDocument66 pagesBody Mechanics and Positioning: Health Assessment' (NCM 101) Skills Mr. Jhonee F. Balmeobevzie datuNo ratings yet