You might also like
- House Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldFrom EverandHouse Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldNo ratings yet
- Ms Mbol 21Document63 pagesMs Mbol 21Sean Lloyd RigonNo ratings yet
- CDC: Improving Communications Around Vaccine Breakthrough and Vaccine EffectivenessDocument25 pagesCDC: Improving Communications Around Vaccine Breakthrough and Vaccine EffectivenessCNBC.com100% (1)
- CDC Internal COVID-19 Delta Variant DocumentDocument25 pagesCDC Internal COVID-19 Delta Variant DocumentAdam Forgie100% (3)
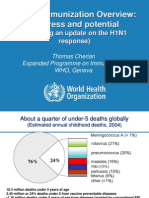
- Global Immunization Overview: Progress and PotentialDocument36 pagesGlobal Immunization Overview: Progress and PotentialPrabir Kumar ChatterjeeNo ratings yet
- LumpkinDocument55 pagesLumpkinSrikanthNo ratings yet
- xxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFDocument22 pagesxxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFRahen Rangan100% (1)
- COVID-19 - Landscape of Novel Coronavirus Candidate Vaccine Development WorldwideDocument13 pagesCOVID-19 - Landscape of Novel Coronavirus Candidate Vaccine Development WorldwideDeka AdeNo ratings yet
- Ending Aids Papua Aids ConferenceDocument48 pagesEnding Aids Papua Aids ConferenceStevanus Bob Arvianto AlwieNo ratings yet
- CCO HCV NOW Downloadable 3Document40 pagesCCO HCV NOW Downloadable 3luamsmarinsNo ratings yet
- Broomberg Shared-Value-HealthDocument23 pagesBroomberg Shared-Value-HealthChunliNo ratings yet
- March 17 Grand Forks Health Officer's DashboardDocument11 pagesMarch 17 Grand Forks Health Officer's DashboardJoe BowenNo ratings yet
- Covid19 The Impact On Healthcare ExpenditureDocument9 pagesCovid19 The Impact On Healthcare ExpenditureDavid ChueNo ratings yet
- Contemporary Management of HIV: Emerging Paradigms in ARTDocument45 pagesContemporary Management of HIV: Emerging Paradigms in ARTluamsmarinsNo ratings yet
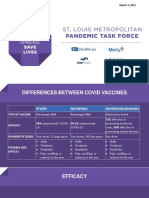
- Task Force Slides 3/3Document26 pagesTask Force Slides 3/3Sam ClancyNo ratings yet
- Deaths and Death Rate by Age Group For Last Two WeeksDocument2 pagesDeaths and Death Rate by Age Group For Last Two WeeksJohn WallerNo ratings yet
- Hospital COVID EMResource Snapshot - October 8th, 2020Document20 pagesHospital COVID EMResource Snapshot - October 8th, 2020The TexanNo ratings yet
- COVID 19 A Year Later AutosavedDocument20 pagesCOVID 19 A Year Later AutosavedALEX CORPORALNo ratings yet
- CCO 2020 Contemporary Management of HIV Emerging Approaches DownloadableDocument52 pagesCCO 2020 Contemporary Management of HIV Emerging Approaches Downloadableluis hernandezNo ratings yet
- Pediatric Bacterial Meningitis in PhilippinesDocument27 pagesPediatric Bacterial Meningitis in Philippinesdranita@yahoo.comNo ratings yet
- Challenges in VH Treatment: Fmoh 2021Document17 pagesChallenges in VH Treatment: Fmoh 2021Eleni HagosNo ratings yet
- 16.03.2021 Novel Coronavirus Landscape COVID-19Document19 pages16.03.2021 Novel Coronavirus Landscape COVID-19Irfan TaufikNo ratings yet
- Jupiter TrialDocument40 pagesJupiter TrialSaad KhanNo ratings yet
- Parasite Factors: Host FactorsDocument55 pagesParasite Factors: Host FactorsAnonymous wxrW6lKaINo ratings yet
- The Impact of Opioid Addiction On Children and FamiliesDocument26 pagesThe Impact of Opioid Addiction On Children and FamiliesNational Press FoundationNo ratings yet
- GPH Tutok Gamutan Davao OrientalDocument3 pagesGPH Tutok Gamutan Davao Orientalrizza RiveraNo ratings yet
- TYRX BrochureDocument28 pagesTYRX Brochureleo chiuNo ratings yet
- WHD InfographicDocument2 pagesWHD InfographicAnonymous 0Mnt71No ratings yet
- Maine ILIweek 2014Document5 pagesMaine ILIweek 2014NEWS CENTER MaineNo ratings yet
- Ministry of Health-Status UpdateDocument24 pagesMinistry of Health-Status UpdateAndre MahardhikaNo ratings yet
- Omicron VaccinneDocument3 pagesOmicron VaccinnePatrick CommettantNo ratings yet
- VACCINES COVID-19 INVIGORATES A STAGNANT INDUSTRYresDocument22 pagesVACCINES COVID-19 INVIGORATES A STAGNANT INDUSTRYresiyad.alsabiNo ratings yet
- Infection Control 1Document63 pagesInfection Control 1Garvit batraNo ratings yet
- WHO Malaria Report 2016 PDFDocument186 pagesWHO Malaria Report 2016 PDFNisa 'Icha' ElNo ratings yet
- May 24 2021 Grand Forks COVID-19 ChangesDocument21 pagesMay 24 2021 Grand Forks COVID-19 ChangesJoe BowenNo ratings yet
- HCV - Best Practice.Document86 pagesHCV - Best Practice.ntnquynhproNo ratings yet
- Presentasi DKT - Aditya - Kontrasepsi Di Masa Pandemi PDFDocument24 pagesPresentasi DKT - Aditya - Kontrasepsi Di Masa Pandemi PDFAnna Ukhti ILaNo ratings yet
- 31.08.2021 Novel Covid 19 Vaccine TrackerDocument22 pages31.08.2021 Novel Covid 19 Vaccine TrackerEvhi KurniaNo ratings yet
- A Challenge For Wolrd Economy PakistanDocument5 pagesA Challenge For Wolrd Economy PakistanZubair AhmedNo ratings yet
- 30 March 2023 - Novel COVID-19 Vaccine Tracker 2Document37 pages30 March 2023 - Novel COVID-19 Vaccine Tracker 2joelomboto815No ratings yet
- The Potential Impact of Different Vaccination PoliciesDocument14 pagesThe Potential Impact of Different Vaccination PoliciesAshwinee KadelNo ratings yet
- India - HIV - 2018 - OverviewDocument23 pagesIndia - HIV - 2018 - OverviewpratyushNo ratings yet
- Static AveXis FinancesDocument16 pagesStatic AveXis FinancessultanmsajidmNo ratings yet
- Hand Hygine Guideline WHODocument6 pagesHand Hygine Guideline WHORiriz AfiantoNo ratings yet
- Effects of Covid 19 - MyraWelleslyCorreia - 02Document26 pagesEffects of Covid 19 - MyraWelleslyCorreia - 02Myra CorreiaNo ratings yet
- Massachusetts Department of Public Health COVID-19 DashboardDocument24 pagesMassachusetts Department of Public Health COVID-19 DashboardJohn WallerNo ratings yet
- Diseases and Illnesses Transmitted to Humans By Animals, Insects And Contaminated Food And Water, 1st Ed.From EverandDiseases and Illnesses Transmitted to Humans By Animals, Insects And Contaminated Food And Water, 1st Ed.No ratings yet
- Healthcare Finance: Modern Financial Analysis for Accelerating Biomedical InnovationFrom EverandHealthcare Finance: Modern Financial Analysis for Accelerating Biomedical InnovationNo ratings yet
- Banking Systems Simulation: Theory, Practice, and Application of Modeling Shocks, Losses, and ContagionFrom EverandBanking Systems Simulation: Theory, Practice, and Application of Modeling Shocks, Losses, and ContagionNo ratings yet
- Pharmaceutical Lifecycle Management: Making the Most of Each and Every BrandFrom EverandPharmaceutical Lifecycle Management: Making the Most of Each and Every BrandNo ratings yet
- How to Arm Yourself Against Vaccine Injuries And What to Do If Things Go WrongFrom EverandHow to Arm Yourself Against Vaccine Injuries And What to Do If Things Go WrongNo ratings yet
- Caring for Others Amid Covid-19: Recruitment and Retention in Long Term CareFrom EverandCaring for Others Amid Covid-19: Recruitment and Retention in Long Term CareNo ratings yet
- A 1753 9801Document9 pagesA 1753 9801Mohammad ShaikhaniNo ratings yet
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 20Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 20EDWIN WIJAYANo ratings yet
- Empyema: An Uncommon Complication of Common Pneumonia: Heather Hsu, HMS III Gillian Lieberman, MDDocument0 pagesEmpyema: An Uncommon Complication of Common Pneumonia: Heather Hsu, HMS III Gillian Lieberman, MDAldo EmeraldNo ratings yet
- Pruritus and Neurocutaneous DermatosesDocument17 pagesPruritus and Neurocutaneous DermatosesgamhaelNo ratings yet
- Medical BooksDocument3 pagesMedical BooksAnh HiềnNo ratings yet
- MCQ PTDocument5 pagesMCQ PTAsobo-khan NkengNo ratings yet
- Surgical Emphysema and Pneumomediastinum Complicating Dental ExtractionDocument2 pagesSurgical Emphysema and Pneumomediastinum Complicating Dental Extractionnewa yudisitaNo ratings yet
- Benign Tumors of Female Genital OrgansDocument37 pagesBenign Tumors of Female Genital Organssimi yNo ratings yet
- Pengkajian LukaDocument27 pagesPengkajian LukabayuNo ratings yet
- Liaison Menu PDFDocument2 pagesLiaison Menu PDFJobany Flores Vertty100% (1)
- แนวข้อสอบ National license - Hematology PDFDocument7 pagesแนวข้อสอบ National license - Hematology PDFTanawat SingboonNo ratings yet
- Barium Meal & EnemaDocument3 pagesBarium Meal & Enemamarvin kyerehNo ratings yet
- Risk Factors of DiabetesDocument29 pagesRisk Factors of DiabetesFarrukh Ali BaigNo ratings yet
- Liceo de Cagayan University: College of NursingDocument18 pagesLiceo de Cagayan University: College of NursingJulie Ann Obenza GaiteraNo ratings yet
- Question Papers 2Document9 pagesQuestion Papers 2Anonymous hYMWbA100% (1)
- Management of Patients With Special NeedsDocument4 pagesManagement of Patients With Special NeedsSophia MolinaNo ratings yet
- JCM 09 00743 v2 PDFDocument20 pagesJCM 09 00743 v2 PDFGordon BongNo ratings yet
- Tuberculosis in Infancy and ChildhoodDocument32 pagesTuberculosis in Infancy and ChildhoodArvin E. PamatianNo ratings yet
- Trauma (Notes)Document26 pagesTrauma (Notes)Priyanka GosaiNo ratings yet
- Dzino's SurgeryDocument718 pagesDzino's SurgeryHuram SeremaniNo ratings yet
- Chronic ParonychiaDocument3 pagesChronic ParonychiaMuhammad Awwalul AkramNo ratings yet
- Gamo - Case Write-Up (TMC OB - Pre-LR 2)Document6 pagesGamo - Case Write-Up (TMC OB - Pre-LR 2)JUAN VICTOR GAMONo ratings yet
- Medical First Aids FinalDocument38 pagesMedical First Aids Finalmedo alaaNo ratings yet
- Metformin Patient HandoutDocument3 pagesMetformin Patient HandoutsilvanaanggraeniNo ratings yet
- Functional Outcome of Surgical Management of Floating Knee Injuries in Adults (Ipsilateral Femoral and Tibia Fractures) and Its Prognostic IndicatorsDocument4 pagesFunctional Outcome of Surgical Management of Floating Knee Injuries in Adults (Ipsilateral Femoral and Tibia Fractures) and Its Prognostic IndicatorsManiDeep ReddyNo ratings yet
- Synopsis PallaviDocument31 pagesSynopsis PallaviSanjeet DuhanNo ratings yet
- Breast LumpDocument17 pagesBreast LumpgaganNo ratings yet
- Weekly Field Epidemiology ReportDocument5 pagesWeekly Field Epidemiology ReportQadeer AfridiNo ratings yet