You might also like
- (Medical Masterclass) Coll.-Infectious Diseases and DermatologyDocument333 pages(Medical Masterclass) Coll.-Infectious Diseases and DermatologyVijay Mg100% (2)
- Proliferative Diabetic Retinopathy and Its Management: A Case SeriesDocument19 pagesProliferative Diabetic Retinopathy and Its Management: A Case SeriesAravind KumarNo ratings yet
- Managing retinal detachment and macular hole with AyurvedaDocument7 pagesManaging retinal detachment and macular hole with AyurvedaAravind KumarNo ratings yet
- IJCRR Nov2020 Vol12 Issue21Document7 pagesIJCRR Nov2020 Vol12 Issue21Aravind KumarNo ratings yet
- IJCRR Dec2020 Vol12 Issue24Document11 pagesIJCRR Dec2020 Vol12 Issue24Aravind KumarNo ratings yet
- Ayurvedic: Exudative Age-Related Macular Degeneration and Its Management: A Case SeriesDocument36 pagesAyurvedic: Exudative Age-Related Macular Degeneration and Its Management: A Case SeriesAravind KumarNo ratings yet
- An Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportDocument8 pagesAn Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportAravind KumarNo ratings yet
- IJCRR Nov2020 Vol12 Issue22Document9 pagesIJCRR Nov2020 Vol12 Issue22Aravind KumarNo ratings yet
- International Ayurvedic Medical Journal: Sreekala Nelliakkattu Parameswaran, Aravind Kumar, Krishnendu SukumaranDocument7 pagesInternational Ayurvedic Medical Journal: Sreekala Nelliakkattu Parameswaran, Aravind Kumar, Krishnendu SukumaranAravind KumarNo ratings yet
- Clinical Profile of Patients of Central Serous Chorioretinopathy Presented To The Tertiary Health Care CentreDocument4 pagesClinical Profile of Patients of Central Serous Chorioretinopathy Presented To The Tertiary Health Care CentreIJAR JOURNALNo ratings yet
- 3849 PDFDocument5 pages3849 PDFAravind KumarNo ratings yet
- Typical Optic Neuritis RevDocument6 pagesTypical Optic Neuritis RevAdhi AmertajayaNo ratings yet
- Case Report Diabetic Retinopaty in EnglishDocument13 pagesCase Report Diabetic Retinopaty in Englishsasha anka DilanNo ratings yet
- Sympathetic Ophthalmia After Vitreoretinal Surgery: A Report of Two CasesDocument11 pagesSympathetic Ophthalmia After Vitreoretinal Surgery: A Report of Two CasesAlexander RezaNo ratings yet
- Nurse-Led Diabetic Retinopathy ScreeningDocument3 pagesNurse-Led Diabetic Retinopathy Screeninganisarahma718No ratings yet
- Commentary: The Optic Neuritis Treatment TrialDocument2 pagesCommentary: The Optic Neuritis Treatment TrialEmmanuel Zótico Orellana JiménezNo ratings yet
- Prevalence and Profile of Central Serous Chorioretinopathy in Indian PatientsDocument6 pagesPrevalence and Profile of Central Serous Chorioretinopathy in Indian PatientsSalsa BillaNo ratings yet
- Application of Diagnostic Criteria For Optic NeuriDocument2 pagesApplication of Diagnostic Criteria For Optic NeuriDea CantikNo ratings yet
- Visual Acuity Approach To A Patient With A Rose-KDocument5 pagesVisual Acuity Approach To A Patient With A Rose-KRagni MishraNo ratings yet
- Approach To Optic Neuritis - An UpdateDocument11 pagesApproach To Optic Neuritis - An UpdateAlexandros GidarakosNo ratings yet
- Review of Optic Neuritis Treatment TrialDocument5 pagesReview of Optic Neuritis Treatment TrialsatrianiNo ratings yet
- Vitrectomy Results in Proliferative Diabetic RetinopathyDocument3 pagesVitrectomy Results in Proliferative Diabetic RetinopathyRohamonangan TheresiaNo ratings yet
- A Rare Complication of Combined Oral Contraceptives (Cocs) : Optic NeuritisDocument3 pagesA Rare Complication of Combined Oral Contraceptives (Cocs) : Optic NeuritisGufront MustofaNo ratings yet
- Northern India RD Risk FactorsDocument6 pagesNorthern India RD Risk Factorsrumaisyah alkatiriNo ratings yet
- Moon2019 PDFDocument7 pagesMoon2019 PDFGusti Zidni FahmiNo ratings yet
- International Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Document5 pagesInternational Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Aravind KumarNo ratings yet
- Ijo 68 1925Document4 pagesIjo 68 1925Afifah Siti NurNo ratings yet
- Optical Coherence Tomography - Macula in Diabetic Macular EdemaDocument6 pagesOptical Coherence Tomography - Macula in Diabetic Macular EdemaIJAR JOURNALNo ratings yet
- PJMS 32 1229Document5 pagesPJMS 32 1229Nurvita WidyastutiNo ratings yet
- Multiple Sclerosis With Ophthalmologic Onset - Case ReportDocument5 pagesMultiple Sclerosis With Ophthalmologic Onset - Case ReportVannyNo ratings yet
- A Clinical Study To Evaluate The Efficacy of Shigru Pallava-Madhu Ashcyotana in Kaphaja Abhishyanda W. S. R To Vernal Kerato ConjunctivitisDocument14 pagesA Clinical Study To Evaluate The Efficacy of Shigru Pallava-Madhu Ashcyotana in Kaphaja Abhishyanda W. S. R To Vernal Kerato Conjunctivitisshalakya007No ratings yet
- Ischemia Modified Albumin As A Useful Marker For Diagnoses and Management of Diabetic RetinopathyDocument5 pagesIschemia Modified Albumin As A Useful Marker For Diagnoses and Management of Diabetic RetinopathyMarcellia AngelinaNo ratings yet
- AIOC2006Document2 pagesAIOC2006Vidyut RajhansNo ratings yet
- Optometry: JournalDocument7 pagesOptometry: JournalsasyaprastiNo ratings yet
- Jurnal Anti VEFGDocument9 pagesJurnal Anti VEFGFitria Sirr Mu'thiarohmahNo ratings yet
- 1600-Article Text-5930-1-10-20231002Document12 pages1600-Article Text-5930-1-10-20231002Yunisa astiaraniNo ratings yet
- Posterior ScleritisDocument4 pagesPosterior ScleritisPande GustianaNo ratings yet
- Afan Diabetik RetinopatiDocument33 pagesAfan Diabetik Retinopatiglory haurissaNo ratings yet
- 1955-Article Text-4468-1-10-20210827Document4 pages1955-Article Text-4468-1-10-20210827DEVIKA RIZKY MAHARANINo ratings yet
- 317694Document16 pages317694Indra PudlianNo ratings yet
- Visual Function in Optic Neuritis and The Effects of Complementary Medicine in Their TreatmentDocument5 pagesVisual Function in Optic Neuritis and The Effects of Complementary Medicine in Their TreatmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Prospective Evaluation of Acupuncture As Treatment For GlaucomaDocument10 pagesProspective Evaluation of Acupuncture As Treatment For Glaucoma16.11Hz MusicNo ratings yet
- Magnetic Resonance Tractographyas A Method of Choice For Neuroimaging in Ocular Ischemic Syndrome Against The Background of HypertensionDocument4 pagesMagnetic Resonance Tractographyas A Method of Choice For Neuroimaging in Ocular Ischemic Syndrome Against The Background of HypertensionCentral Asian StudiesNo ratings yet
- Visual Outcomes Following Small Incision Cataract Surgery (SICS) in Wangaya HospitalDocument4 pagesVisual Outcomes Following Small Incision Cataract Surgery (SICS) in Wangaya HospitalKrisnhalianiNo ratings yet
- Rehabilitation and Treatment Algorithm For Patients With Ocular Ischemic Syndrome On The Background of Arterial HypertensionDocument3 pagesRehabilitation and Treatment Algorithm For Patients With Ocular Ischemic Syndrome On The Background of Arterial HypertensionCentral Asian StudiesNo ratings yet
- COMPLETODocument9 pagesCOMPLETOZarella Ramírez BorreroNo ratings yet
- 3Document10 pages3Omnia ZapharusNo ratings yet
- Eyes That Look Down and Out A Case Series On Isolated Third Nerve PalsyDocument4 pagesEyes That Look Down and Out A Case Series On Isolated Third Nerve PalsyIJAR JOURNALNo ratings yet
- Update on Diagnosis and Treatment of Idiopathic Intracranial HypertensionDocument13 pagesUpdate on Diagnosis and Treatment of Idiopathic Intracranial HypertensionMomeneo NeoNo ratings yet
- JAyurveda162161-15848 042408Document9 pagesJAyurveda162161-15848 042408Aravind KumarNo ratings yet
- Ayurvedic Management of Prurigo nodularis at scalp - A case reportDocument5 pagesAyurvedic Management of Prurigo nodularis at scalp - A case reportmskchoudhuriNo ratings yet
- Rheumatoid Arthritis Associated Episcleritis and Scleritis: An Update On Treatment PerspectivesDocument14 pagesRheumatoid Arthritis Associated Episcleritis and Scleritis: An Update On Treatment PerspectivesFenty IswarNo ratings yet
- Prevalence of Glaucoma in North Costal Andhra PradeshDocument7 pagesPrevalence of Glaucoma in North Costal Andhra PradeshIJAR JOURNALNo ratings yet
- Idiopathic Orbital in Ammation (2) : Delhi Journal of Ophthalmology November 2022Document4 pagesIdiopathic Orbital in Ammation (2) : Delhi Journal of Ophthalmology November 2022SuvratNo ratings yet
- Current Management of Diabetic MaculopathyDocument8 pagesCurrent Management of Diabetic MaculopathyraniNo ratings yet
- Research Article: Ayurvedic Management of Acute Anterior Uveitis (Pittaja Adhimantha) : A Case StudyDocument5 pagesResearch Article: Ayurvedic Management of Acute Anterior Uveitis (Pittaja Adhimantha) : A Case StudySiddesh bn SidNo ratings yet
- Rhegmatogenous Retinal DetachmentDocument6 pagesRhegmatogenous Retinal DetachmentPutri kartiniNo ratings yet
- Retinal Detachment After Intravitreal Injections: 13-Case SeriesDocument6 pagesRetinal Detachment After Intravitreal Injections: 13-Case SeriesPutri kartiniNo ratings yet
- Optic Neuritis: Clinical PR ActiceDocument8 pagesOptic Neuritis: Clinical PR ActiceafbmgNo ratings yet
- Case Report of Diethyl Carbamazine Induced Anterior Uveitis With Raised Intraocular Pressure in Known Case of Lymphatic FilariasisDocument4 pagesCase Report of Diethyl Carbamazine Induced Anterior Uveitis With Raised Intraocular Pressure in Known Case of Lymphatic FilariasisIJAR JOURNALNo ratings yet
- Diabetic Retinopathy: Introduction to Novel Treatment StrategiesFrom EverandDiabetic Retinopathy: Introduction to Novel Treatment StrategiesNo ratings yet
- PDR With RD - PublishedDocument4 pagesPDR With RD - PublishedAravind KumarNo ratings yet
- JAyurveda162161-15848 042408Document9 pagesJAyurveda162161-15848 042408Aravind KumarNo ratings yet
- 3849 PDFDocument5 pages3849 PDFAravind KumarNo ratings yet
- JAyurvedaCaseRep 2021 4 4 138 337115Document9 pagesJAyurvedaCaseRep 2021 4 4 138 337115Aravind KumarNo ratings yet
- How To Be Indexed in PubMedDocument4 pagesHow To Be Indexed in PubMedAravind KumarNo ratings yet
- International Ayurvedic Medical JournalDocument5 pagesInternational Ayurvedic Medical JournalAravind KumarNo ratings yet
- Kriyakalpa in Netra Cikitsa-2Document41 pagesKriyakalpa in Netra Cikitsa-2Aravind KumarNo ratings yet
- NIH Public Access: Author ManuscriptDocument36 pagesNIH Public Access: Author ManuscriptAravind KumarNo ratings yet
- 70Document5 pages70Aravind KumarNo ratings yet
- An Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportDocument8 pagesAn Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportAravind KumarNo ratings yet
- International Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Document5 pagesInternational Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Aravind KumarNo ratings yet
- International Ayurvedic Medical Journal: Sreekala Nelliakkattu Parameswaran, Aravind Kumar, Krishnendu SukumaranDocument7 pagesInternational Ayurvedic Medical Journal: Sreekala Nelliakkattu Parameswaran, Aravind Kumar, Krishnendu SukumaranAravind KumarNo ratings yet
- IJCRR Nov2020 Vol12 Issue22Document9 pagesIJCRR Nov2020 Vol12 Issue22Aravind KumarNo ratings yet
- IJCRR Nov2020 Vol12 Issue22Document9 pagesIJCRR Nov2020 Vol12 Issue22Aravind KumarNo ratings yet
- An Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportDocument8 pagesAn Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportAravind KumarNo ratings yet
- International Ayurvedic Medical Journal: Sreekala Nelliakkattu Parameswaran, Aravind Kumar, Krishnendu SukumaranDocument7 pagesInternational Ayurvedic Medical Journal: Sreekala Nelliakkattu Parameswaran, Aravind Kumar, Krishnendu SukumaranAravind KumarNo ratings yet
- An Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportDocument8 pagesAn Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportAravind KumarNo ratings yet
- International Ayurvedic Medical JournalDocument5 pagesInternational Ayurvedic Medical JournalAravind KumarNo ratings yet
- PDR With RD - PublishedDocument4 pagesPDR With RD - PublishedAravind KumarNo ratings yet
- Ayurvedic treatment improves vision in retinal vein occlusion caseDocument4 pagesAyurvedic treatment improves vision in retinal vein occlusion caseAravind KumarNo ratings yet
- Chapter 5 Normal Microbial Flora and Pathogenic Bacteria HardDocument14 pagesChapter 5 Normal Microbial Flora and Pathogenic Bacteria HardRizalyn Padua ReyNo ratings yet
- Community Question Bank (N.a)Document41 pagesCommunity Question Bank (N.a)Sumaya AfifyNo ratings yet
- TRAFFIC JAM in EVERESTDocument18 pagesTRAFFIC JAM in EVERESTSB100% (1)
- Clinical Course Discussion: Oregon Health & Science University, Portland, OregonDocument1 pageClinical Course Discussion: Oregon Health & Science University, Portland, OregonperjadanutNo ratings yet
- Different Iv FluidsDocument2 pagesDifferent Iv FluidsBeverly DatuNo ratings yet
- Specialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDocument18 pagesSpecialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDeborah RiskinNo ratings yet
- 2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Document11 pages2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Anggi RiyaniNo ratings yet
- Sexual Health Awareness ScaleDocument17 pagesSexual Health Awareness ScaleezazpsychologistNo ratings yet
- Skilled Birth Attendant (SBA) : State Institute of Health & Family Welfare JaipurDocument32 pagesSkilled Birth Attendant (SBA) : State Institute of Health & Family Welfare JaipurDurga NaikNo ratings yet
- Treatment of Acute BronchitisDocument3 pagesTreatment of Acute BronchitisjokosudibyoNo ratings yet
- Sia DH FinalDocument26 pagesSia DH FinalJennifer DixonNo ratings yet
- Garner 1511222Document17 pagesGarner 1511222Bj LongNo ratings yet
- Child Health COURSE PLAN M.SC 2 YEARDocument49 pagesChild Health COURSE PLAN M.SC 2 YEARSanthosh.S.UNo ratings yet
- NCP Activity NavidasDocument2 pagesNCP Activity NavidasFran LanNo ratings yet
- Hydrotherapy Principles & TechniquesDocument75 pagesHydrotherapy Principles & TechniquesSANLAPAN SAHOONo ratings yet
- Phlebotomy Essentials 7th EditionDocument61 pagesPhlebotomy Essentials 7th Editioneric.rodriguez669100% (44)
- Rabbithematology PDFDocument12 pagesRabbithematology PDFHuda HudaNo ratings yet
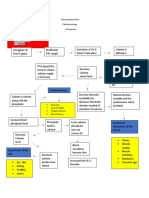
- Hypoparathyroidism PathophysiologyDocument1 pageHypoparathyroidism PathophysiologymaricarNo ratings yet
- Eat Yourself Smart: Britain Faces Airlift DeadlineDocument64 pagesEat Yourself Smart: Britain Faces Airlift DeadlineNidhi BhartiNo ratings yet
- M.Sc Psychology Syllabus Provides Comprehensive CoverageDocument55 pagesM.Sc Psychology Syllabus Provides Comprehensive CoverageRashmi NNo ratings yet
- Podcast Script "Hustle Culture" OPENING: Haiii I'am Hidayah Malika and Welcome To Speak Up' PodcastDocument3 pagesPodcast Script "Hustle Culture" OPENING: Haiii I'am Hidayah Malika and Welcome To Speak Up' PodcastMas'adatul HidayahNo ratings yet
- International Journal of Cardiology May 2021 Issue 1Document275 pagesInternational Journal of Cardiology May 2021 Issue 1Fareesha KhanNo ratings yet
- 13 AntibioticsAntiRetroviralsAIDS PDFDocument90 pages13 AntibioticsAntiRetroviralsAIDS PDFjenniferluzonNo ratings yet
- Pentasa Tablets and Sachets PIDocument14 pagesPentasa Tablets and Sachets PIGeo GeoNo ratings yet
- Activity - Nutrition On The Internet Worksheet 3Document2 pagesActivity - Nutrition On The Internet Worksheet 3Carlo FernandoNo ratings yet
- Methods of Social Work Practice: February 2019Document17 pagesMethods of Social Work Practice: February 2019said abubakar100% (1)
- Script Komik : SectorsDocument31 pagesScript Komik : SectorsTricia OfeliaNo ratings yet
- English: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentDocument33 pagesEnglish: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentShiela Tecson Gamayon40% (5)
- A Survey On Data Mining Techniques For COVID PredictionDocument6 pagesA Survey On Data Mining Techniques For COVID PredictionWARSE Journals100% (2)