You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Human Diseases 8th Edition Ebook PDFDocument41 pagesHuman Diseases 8th Edition Ebook PDFchad.archuleta889100% (37)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Admission of Patient For SurgeryDocument5 pagesAdmission of Patient For SurgeryMADEL CAGARA DONDOYANONo ratings yet
- Diagnostic Radiology and Imaging For TechniciansDocument314 pagesDiagnostic Radiology and Imaging For Techniciansscribangelof50% (2)
- 2016 1 74chirurgiaDocument7 pages2016 1 74chirurgiaAnitei GabrielaNo ratings yet
- BreastDocument14 pagesBreastAnitei GabrielaNo ratings yet
- Practical Cardio-Oncology (2019, CRC Press)Document261 pagesPractical Cardio-Oncology (2019, CRC Press)Anitei GabrielaNo ratings yet
- Bile Duct Programme Nov 2020Document1 pageBile Duct Programme Nov 2020Anitei GabrielaNo ratings yet
- Abdominoperineal Extralevator ResectionDocument4 pagesAbdominoperineal Extralevator ResectionAnitei GabrielaNo ratings yet
- J Gastrointest SurgDocument6 pagesJ Gastrointest SurgAnitei GabrielaNo ratings yet
- Desser 2007. Simulation-Based Training The Next Revolution in Radiology EducationDocument9 pagesDesser 2007. Simulation-Based Training The Next Revolution in Radiology EducationArmin AriasNo ratings yet
- Quality of Periapical Radiographs Taken by Undergraduate Dental Students at Qassim UniversityDocument7 pagesQuality of Periapical Radiographs Taken by Undergraduate Dental Students at Qassim UniversitySekarSukomasajiNo ratings yet
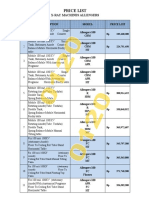
- Daftar Harga Allengers - 012020Document8 pagesDaftar Harga Allengers - 012020Bintang Rejeki AlkesindoNo ratings yet
- Radiology FactSheet ICN907164Document4 pagesRadiology FactSheet ICN907164Vevi VarcetyNo ratings yet
- Analisis Kesesuaian Lapangan Kolimasi Pada Alat Digital RadiografiDocument6 pagesAnalisis Kesesuaian Lapangan Kolimasi Pada Alat Digital RadiografiWidya ChesarNo ratings yet
- Answer All MCQ Questions From No. 1 To 50. Each Question Will Carry 2 MarksDocument4 pagesAnswer All MCQ Questions From No. 1 To 50. Each Question Will Carry 2 MarksRick DasNo ratings yet
- Diseases of The Chest, Breast, Heart and Vessels 2019-2022: Juerg Hodler Rahel A. Kubik-Huch Gustav K. Von SchulthessDocument237 pagesDiseases of The Chest, Breast, Heart and Vessels 2019-2022: Juerg Hodler Rahel A. Kubik-Huch Gustav K. Von SchulthessMinh đăng ĐỗNo ratings yet
- Comparison Between Discrete Cosine and Wave Let TransformDocument6 pagesComparison Between Discrete Cosine and Wave Let TransformMichaelNo ratings yet
- Planning and Management of Clinical Service DepartmentDocument41 pagesPlanning and Management of Clinical Service DepartmentDrPriyanka Prashant PawsheNo ratings yet
- Emailing Nuclear Medicine - The Requisites 3rd EditionDocument606 pagesEmailing Nuclear Medicine - The Requisites 3rd EditionIrinaMariaStrugariNo ratings yet
- RadtechDocument3 pagesRadtechKlarissa Nebit JavierNo ratings yet
- Medical Radiation Dosimetrist - UicDocument4 pagesMedical Radiation Dosimetrist - Uicapi-247959633No ratings yet
- Reflections On 60 Years of Development in Medical PhysicsDocument7 pagesReflections On 60 Years of Development in Medical PhysicsJavier MorenoNo ratings yet
- Artificialintelligence Applicationsfor Workflow, Process Optimizationandpredictive AnalyticsDocument15 pagesArtificialintelligence Applicationsfor Workflow, Process Optimizationandpredictive AnalyticsSantosh Kumar TataNo ratings yet
- Australian Dental Journal: Contemporary Medico-Legal Dental RadiologyDocument7 pagesAustralian Dental Journal: Contemporary Medico-Legal Dental RadiologyVsh SngNo ratings yet
- Previous Years Question PapersDocument19 pagesPrevious Years Question PapersViraj ShahNo ratings yet
- Common Postmortem Computed Tomography Findings Following Atraumatic Death - Differentiation Between Normal Postmortem Changes and Pathologic LesionsDocument12 pagesCommon Postmortem Computed Tomography Findings Following Atraumatic Death - Differentiation Between Normal Postmortem Changes and Pathologic LesionsFrédérique ThicotNo ratings yet
- Unistrut: Medical Support Structure GuideDocument25 pagesUnistrut: Medical Support Structure Guidedeviationz100% (1)
- Ai Care: Artificial Intelligence Healthcare Solution Provider COMSATS University IslamabadDocument17 pagesAi Care: Artificial Intelligence Healthcare Solution Provider COMSATS University IslamabadRohail SiddiqueNo ratings yet
- Brochure Detector Family 202002Document4 pagesBrochure Detector Family 202002JaimeNo ratings yet
- Genral SurgeryDocument24 pagesGenral SurgeryaravNo ratings yet
- Rad TechDocument3 pagesRad TechJulia CampomanesNo ratings yet
- Mercy Hospital - Crystal Lake ReviewDocument33 pagesMercy Hospital - Crystal Lake ReviewNorthwest HeraldNo ratings yet
- P03-010-CPQ.627.03.01.02 s.viaViewGO VA15A DS 152104899Document12 pagesP03-010-CPQ.627.03.01.02 s.viaViewGO VA15A DS 152104899sony sutrisnoNo ratings yet
- Sample Radiology Application FormDocument28 pagesSample Radiology Application Formjoedeegan_No ratings yet
- Periostalne ReakcijeDocument9 pagesPeriostalne ReakcijeVesna PavlovicNo ratings yet
- RANZCR Policy (Clinical Radiology)Document29 pagesRANZCR Policy (Clinical Radiology)AhmedNo ratings yet