You might also like
- The No B.S. Guide To Anterior Pelvic Tilt: In-Depth Assessment and 6-Week ProgramDocument39 pagesThe No B.S. Guide To Anterior Pelvic Tilt: In-Depth Assessment and 6-Week ProgramKosar83% (6)
- Vince Gironda 8x8 RoutineDocument10 pagesVince Gironda 8x8 RoutineCLAVDIVS0% (2)
- De La Cruz, Et Al. (2015) Treatment of Children With ADHD and IrritabilityDocument12 pagesDe La Cruz, Et Al. (2015) Treatment of Children With ADHD and Irritabilityjuan100% (1)
- Care of The Hospitalized ChildDocument60 pagesCare of The Hospitalized ChildJSeasharkNo ratings yet
- Health 10: 3 Quarter Week 7Document10 pagesHealth 10: 3 Quarter Week 7Maria Rose Tariga Aquino50% (2)
- Led 2 EpidemiologyDocument6 pagesLed 2 Epidemiologyd3mooz13No ratings yet
- Welsing PositionDocument5 pagesWelsing PositionBering Frederick ChristianNo ratings yet
- Bharath Doke Resume PDFDocument2 pagesBharath Doke Resume PDFSonu DokeNo ratings yet
- Johayria B. Sumndad 2BSBA-A EXERCISE 1.2Document5 pagesJohayria B. Sumndad 2BSBA-A EXERCISE 1.2Johayria SumndadNo ratings yet
- 5 FunctionsDocument4 pages5 FunctionsADITHYA SNo ratings yet
- Qdoc - Tips Biology Investigatory ProjectDocument44 pagesQdoc - Tips Biology Investigatory ProjectVikas SolankiNo ratings yet
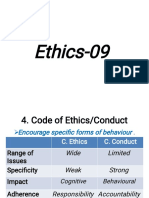
- Ethics Class 9Document30 pagesEthics Class 9suraj bhavsarNo ratings yet
- Reviewer 10Document15 pagesReviewer 10MarlouNo ratings yet
- Mirant V CaroDocument3 pagesMirant V CaroMarichelNo ratings yet
- DI Arrhea Part-1 Generali Nformati ON: I NDI VI Dualprofi LEDocument12 pagesDI Arrhea Part-1 Generali Nformati ON: I NDI VI Dualprofi LEsandeepNo ratings yet
- Final Annual Report 2020 PDFDocument32 pagesFinal Annual Report 2020 PDFFrancis d'souzaNo ratings yet
- 2018 GuideDocument6 pages2018 Guidekaung sanNo ratings yet
- Tort 01Document2 pagesTort 01slckmeetworkshopNo ratings yet
- Development: Economi CdevelopmentDocument5 pagesDevelopment: Economi CdevelopmentharinichristoberNo ratings yet
- Page 1Document1 pagePage 1rizwhanNo ratings yet
- Human Figure Drawing TestDocument17 pagesHuman Figure Drawing TestMuhammad ZubairNo ratings yet
- CIV G11 Note-1-1-1Document27 pagesCIV G11 Note-1-1-1Hamzaa Jamal JuwarNo ratings yet
- Vamshi 1Document2 pagesVamshi 1whatts app status videosNo ratings yet
- Strata I GraphyDocument13 pagesStrata I GraphyhishamlashennNo ratings yet
- ProfEd8 Week16&17 EstradaDocument2 pagesProfEd8 Week16&17 EstradaRandolf Aronales EstradaNo ratings yet
- Surveillance System in The PhilippinesDocument38 pagesSurveillance System in The PhilippinesFred C. MirandaNo ratings yet
- Notredameofmi Dsayapcol L Ege Ay:2020-2021Document5 pagesNotredameofmi Dsayapcol L Ege Ay:2020-2021Aljiya AhadainNo ratings yet
- Resume Format - CDocument3 pagesResume Format - Cnehanayaka25No ratings yet
- Indian Political SystemDocument12 pagesIndian Political SystemSharique RazaNo ratings yet
- Barangay SuyangDocument1 pageBarangay SuyangblairNo ratings yet
- Epidemiology WPS OfficeDocument8 pagesEpidemiology WPS OfficeSri WaerNo ratings yet
- Stonegroup Covid19 enDocument15 pagesStonegroup Covid19 enSimona SavaNo ratings yet
- Proofreading and Editing Activity 1Document1 pageProofreading and Editing Activity 1Ruary CajucomNo ratings yet
- Social PharmacyDocument5 pagesSocial PharmacyAbhas MahatoNo ratings yet
- (PEDIA) History ChecklistDocument7 pages(PEDIA) History ChecklistReggie Lyn BaricanNo ratings yet
- Informative Speech About Teenage PregnancyDocument2 pagesInformative Speech About Teenage Pregnancychristianraiz540No ratings yet
- TestDocument10 pagesTestDeepali ChaubeyNo ratings yet
- Diwit Health Declaration FormDocument2 pagesDiwit Health Declaration FormBhell MendiolaNo ratings yet
- Artikel Sugesti Dwi Retno - Id.enDocument7 pagesArtikel Sugesti Dwi Retno - Id.enSugesti RetnoNo ratings yet
- Handout PDFDocument1 pageHandout PDFspotify2018 gmNo ratings yet
- E&D and Treatment Plan FormDocument8 pagesE&D and Treatment Plan FormNURUL AFIRA BINTI MOHD SALEHNo ratings yet
- Sobbing Souls Absoliom MDocument128 pagesSobbing Souls Absoliom MNdumiso Mike NdlovuNo ratings yet
- Rohit CVDocument2 pagesRohit CVRohit NegiNo ratings yet
- GL Obal L I Zat I Onandregi Onal I SM I Ntrodacti OnDocument7 pagesGL Obal L I Zat I Onandregi Onal I SM I Ntrodacti OnGizachew AbeshaNo ratings yet
- Donebyk. PR Asant H Kumar: Case Presentati OnDocument4 pagesDonebyk. PR Asant H Kumar: Case Presentati OnRekhaNo ratings yet
- Comflict Resolution in MarriagesDocument9 pagesComflict Resolution in MarriagesBaCharles MatekeNo ratings yet
- Early Vedic AgeDocument22 pagesEarly Vedic AgeMd. Samiul IslamNo ratings yet
- How Do Org. Repro. (Sexual Reproduction)Document9 pagesHow Do Org. Repro. (Sexual Reproduction)VVS. BS.S1995No ratings yet
- My Reaction PaperDocument2 pagesMy Reaction PaperQuindap JonalineNo ratings yet
- Module 4 Human Person and Death859Document11 pagesModule 4 Human Person and Death859Lax ReignNo ratings yet
- HIV in South AfricaDocument17 pagesHIV in South AfricaMadelineNo ratings yet
- Jeet Roy Part 2 May 22, 2021Document6 pagesJeet Roy Part 2 May 22, 2021YAZI 77No ratings yet
- Share 2-BSABE-B - YBAÑEZ, RM. - Module 2-L1Document2 pagesShare 2-BSABE-B - YBAÑEZ, RM. - Module 2-L1Rene Mark YbañezNo ratings yet
- STD VI Chapter 2 Geography NCERT SolutionsDocument4 pagesSTD VI Chapter 2 Geography NCERT SolutionsSK TAZUDDINNo ratings yet
- L5-Aedes Aegypti and Vectors of DEN YF and CHIK-PVMMDocument94 pagesL5-Aedes Aegypti and Vectors of DEN YF and CHIK-PVMMjcr42051No ratings yet
- Contemporaryworld: PR Epar Edby: I Bañezjeni Fer, Lozadajoyandrodr I Gochar L Es Bs.I Nformati Onsystem3CDocument21 pagesContemporaryworld: PR Epar Edby: I Bañezjeni Fer, Lozadajoyandrodr I Gochar L Es Bs.I Nformati Onsystem3CJayr FloresNo ratings yet
- Eco FinalDocument4 pagesEco FinalRohit SinghNo ratings yet
- Guide 16 Phil GovtDocument1 pageGuide 16 Phil GovtSharmaine MirandaNo ratings yet
- Fuji Television Network Vs Espiritu Digest - CompressDocument10 pagesFuji Television Network Vs Espiritu Digest - CompressJona Phoebe MangalindanNo ratings yet
- د.جمال المشوليAcute diarrhoea&dehydratin 81085Document9 pagesد.جمال المشوليAcute diarrhoea&dehydratin 81085zizoNo ratings yet
- Be Lazy & Still Score A's Lite VersionDocument48 pagesBe Lazy & Still Score A's Lite VersionLight House Learning GroupNo ratings yet
- Graccie - Intro To PhiloDocument4 pagesGraccie - Intro To PhiloGraccie lei ReynoNo ratings yet
- Title - Jeepney-WPS Office PDFDocument1 pageTitle - Jeepney-WPS Office PDFangel cantonjosNo ratings yet
- Office Administration MCQDocument3 pagesOffice Administration MCQJanmejay BrishketuNo ratings yet
- Presented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Document17 pagesPresented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Akanksha KapoorNo ratings yet
- Liver & Kidney Transplant - A5 Folder - Digital - 2022Document4 pagesLiver & Kidney Transplant - A5 Folder - Digital - 2022lakshminivas PingaliNo ratings yet
- Medicowesome Glasgow Coma Scale Mnemonic 2Document1 pageMedicowesome Glasgow Coma Scale Mnemonic 2KC Dela RosaNo ratings yet
- Greenwood Village Vaping Ordinance ProposalDocument2 pagesGreenwood Village Vaping Ordinance ProposalMichael_Lee_RobertsNo ratings yet
- Brasso Metal Polish v1.3 D8340649 PDFDocument10 pagesBrasso Metal Polish v1.3 D8340649 PDFNia PuanNo ratings yet
- Book StickerDocument4 pagesBook Stickerilanabiela90No ratings yet
- Kinds of Blood. Differences Between Men and WomenDocument11 pagesKinds of Blood. Differences Between Men and WomenTiagoSantosNo ratings yet
- Child Health Services-1Document44 pagesChild Health Services-1francisNo ratings yet
- Material Safety Data Sheet: 1 Identification of SubstanceDocument5 pagesMaterial Safety Data Sheet: 1 Identification of SubstanceRey AgustinNo ratings yet
- Summary of Wind Turbine Accident Data To 31 December 2016Document6 pagesSummary of Wind Turbine Accident Data To 31 December 2016أحمد دعبسNo ratings yet
- Analysis of GRIHA Certified BuildingsDocument26 pagesAnalysis of GRIHA Certified BuildingsAnshul Sharma100% (7)
- Crisis Management and Human Behaviour Mca ApprovedDocument2 pagesCrisis Management and Human Behaviour Mca ApprovedVinil Gupta100% (1)
- The Dandenong Dossier 2010Document243 pagesThe Dandenong Dossier 2010reshminNo ratings yet
- Glycerol MsdsDocument6 pagesGlycerol MsdsJX Lim0% (1)
- Murawski 2009Document6 pagesMurawski 2009Sofia Valeria MonrealNo ratings yet
- Group 3 Oral Bioavailability EditedDocument10 pagesGroup 3 Oral Bioavailability EditedBaguma MichaelNo ratings yet
- M Fajar Alwi Muchsin - D3TGDocument7 pagesM Fajar Alwi Muchsin - D3TGNugi AshterNo ratings yet
- PDF 20221013 211252 0000Document1 pagePDF 20221013 211252 0000Meann جرابيللوNo ratings yet
- Wu 2008Document8 pagesWu 2008SergioNo ratings yet
- Engl7 Q4 W4 Determining-Accuracy Villanueva Bgo Reviewed-1Document18 pagesEngl7 Q4 W4 Determining-Accuracy Villanueva Bgo Reviewed-1johbaguilatNo ratings yet
- Bias, Confounding and Fallacies in EpidemiologyDocument68 pagesBias, Confounding and Fallacies in EpidemiologyShakir KhanNo ratings yet
- Hypo - RT PC TrialDocument37 pagesHypo - RT PC TrialnitinNo ratings yet
- AssignmentDocument2 pagesAssignmentReserva, ArchelleNo ratings yet
- Gallstone, Choledocholithiasis, Ascending CholangistisDocument12 pagesGallstone, Choledocholithiasis, Ascending CholangistisNurulasyikin MAA100% (1)
- Ultrafiltration and Its Application in Food Processing: October 2015Document15 pagesUltrafiltration and Its Application in Food Processing: October 2015Doina PolisciucNo ratings yet