You might also like
- Anemia of Chronic Disease - Inflammation - UpToDateDocument36 pagesAnemia of Chronic Disease - Inflammation - UpToDateDomenica MurilloNo ratings yet
- FLCCC Protocols - A Guide To The Management of COVID 19Document61 pagesFLCCC Protocols - A Guide To The Management of COVID 19cceng06100% (2)
- Vitamin Pharmacogenomics New Insight Into Individual Differences in Diseases and Drug ResponsesDocument7 pagesVitamin Pharmacogenomics New Insight Into Individual Differences in Diseases and Drug ResponsesFadil Indra SanjayaNo ratings yet
- ReportDocument10 pagesReportAnkita GoyalNo ratings yet
- Prep 2023Document909 pagesPrep 2023Imran A. Isaac100% (7)
- Vit D 300000Document6 pagesVit D 300000Kay Kim100% (1)
- 1 s2.0 S2214623714000040 MainDocument7 pages1 s2.0 S2214623714000040 MainSagita DarmasariNo ratings yet
- Vitamin D and Human Health: Molecular SciencesDocument6 pagesVitamin D and Human Health: Molecular SciencesRuth WibowoNo ratings yet
- Anemia of Chronic Disease - Anemia of Inflammation - UpToDateDocument37 pagesAnemia of Chronic Disease - Anemia of Inflammation - UpToDateanweridrisejazNo ratings yet
- The Role of Vitamin D in Enhancing Immunity and Its RecommendationsDocument4 pagesThe Role of Vitamin D in Enhancing Immunity and Its RecommendationsWarstek TVNo ratings yet
- Artigo Ingles SalomanDocument8 pagesArtigo Ingles SalomanBiomédica Fabiane IngrideNo ratings yet
- Current Perspectives Immune System and Chronic DiseasesDocument6 pagesCurrent Perspectives Immune System and Chronic DiseasesHenry LahoreNo ratings yet
- 1 Jurnal Vit DDocument11 pages1 Jurnal Vit DDelvia AuroraNo ratings yet
- 8156 142v58vDocument14 pages8156 142v58vsajantkNo ratings yet
- Iron Deficiency Anaemia Revisited: M. D. Cappellini, K. M. Musallam & A. T. TaherDocument18 pagesIron Deficiency Anaemia Revisited: M. D. Cappellini, K. M. Musallam & A. T. TaherJhonyHinojosaNo ratings yet
- Vitamin D: Modulator of The Immune SystemDocument15 pagesVitamin D: Modulator of The Immune SystemJosé Antonio Silva NetoNo ratings yet
- Relationship-Between VitD AndThyroidDocument15 pagesRelationship-Between VitD AndThyroidAmazing SecretsNo ratings yet
- HHS Public AccessDocument17 pagesHHS Public Accessdowntolevel1No ratings yet
- Vitamin Role PD MainDocument15 pagesVitamin Role PD Mainhuseikha velayazulfahdNo ratings yet
- Vitamin D: The Unknown Cure For Autoimmune DiseasesDocument1 pageVitamin D: The Unknown Cure For Autoimmune DiseasesCristiana IliescuNo ratings yet
- Management of Preoperative Anemia: Laura Mendez-Pino,, Andrés Zorrilla-Vaca,, David L. HepnerDocument9 pagesManagement of Preoperative Anemia: Laura Mendez-Pino,, Andrés Zorrilla-Vaca,, David L. HepneryenuginNo ratings yet
- Anemia Ferropenica Rev2019Document18 pagesAnemia Ferropenica Rev2019Albamis MojicaNo ratings yet
- Nutrients: Vitamin D: Nutrient, Hormone, and ImmunomodulatorDocument14 pagesNutrients: Vitamin D: Nutrient, Hormone, and ImmunomodulatorAffan ElahiNo ratings yet
- Vitamin D Resistance As A Possible Cause of Autoimmune Diseases: A Hypothesis Con Firmed by A Therapeutic High-Dose Vitamin D ProtocolDocument11 pagesVitamin D Resistance As A Possible Cause of Autoimmune Diseases: A Hypothesis Con Firmed by A Therapeutic High-Dose Vitamin D Protocoldr belaidi nadirNo ratings yet
- Omega 3 Terapia COVID 19Document11 pagesOmega 3 Terapia COVID 19Carlos MendozaNo ratings yet
- Vitamin D Deficiency and Anemia Risk in ChildrenDocument9 pagesVitamin D Deficiency and Anemia Risk in ChildrenRandy SuryawanNo ratings yet
- Vitamin DResistanceasa Possible Causeof Autoimmune Diseases Lemke 2021Document12 pagesVitamin DResistanceasa Possible Causeof Autoimmune Diseases Lemke 2021NathanNo ratings yet
- Vitamin D in Health and Disease A Literature ReviewDocument7 pagesVitamin D in Health and Disease A Literature Reviewfihum1hadej2100% (1)
- PDF 6Document26 pagesPDF 6Ajeng Nur NabillahNo ratings yet
- CKD N Vit DDocument4 pagesCKD N Vit DaziezahajeNo ratings yet
- Vitamin D3 Protects Against Diabetic Retinopathy by Inhibiting High-Glucose-Induced Activation of The ROS:TXNIP:NLRP3 Inflammasome PathwayDocument12 pagesVitamin D3 Protects Against Diabetic Retinopathy by Inhibiting High-Glucose-Induced Activation of The ROS:TXNIP:NLRP3 Inflammasome PathwayEzra MargarethNo ratings yet
- The Role of Vitamin D in The Immunopathogenesis of Allergic Skin DiseasesDocument6 pagesThe Role of Vitamin D in The Immunopathogenesis of Allergic Skin DiseasesAndre FerdianNo ratings yet
- Vitamin D Deficiency and Myocardial DiseasesDocument11 pagesVitamin D Deficiency and Myocardial DiseasesDr. AyshaNo ratings yet
- Vitamin D Deficiency Is Associated With Anaemia Among African Americans in A Us CohortDocument9 pagesVitamin D Deficiency Is Associated With Anaemia Among African Americans in A Us Cohortmeiimei meilienhaNo ratings yet
- Hypertension JournalDocument5 pagesHypertension JournalYola SurbaktiNo ratings yet
- Vitamind - TB PDFDocument7 pagesVitamind - TB PDFmustikaarumNo ratings yet
- Nutrients: Vitamin D and Immunity in Infants and ChildrenDocument29 pagesNutrients: Vitamin D and Immunity in Infants and ChildrenAbdaud RasyidNo ratings yet
- Agarwal 2009Document6 pagesAgarwal 2009Cristian CozmaNo ratings yet
- Vitamin D in Behcet's Disease, A Brief Review of The LiteratureDocument5 pagesVitamin D in Behcet's Disease, A Brief Review of The Literaturerhf.turki6877No ratings yet
- Voulgaris2017 Article VitaminDAndAspectsOfFemaleFertDocument17 pagesVoulgaris2017 Article VitaminDAndAspectsOfFemaleFertLinnette AnaniasNo ratings yet
- The Antisickling Effects of Some Micronutrients and Antioxidant Vitamins in Sickle Cell Disease ManagementDocument7 pagesThe Antisickling Effects of Some Micronutrients and Antioxidant Vitamins in Sickle Cell Disease ManagementVeraNo ratings yet
- Vitamin D and Aspects of Female Fertility: ReviewDocument17 pagesVitamin D and Aspects of Female Fertility: ReviewOumaima Ben MerrakchiNo ratings yet
- Hypertensionaha 113 02298Document3 pagesHypertensionaha 113 02298fenix projectNo ratings yet
- Vitamina D e ImunidadeDocument4 pagesVitamina D e ImunidadeVitória FreitasNo ratings yet
- Molecular and Cellular Endocrinology: EditorialDocument2 pagesMolecular and Cellular Endocrinology: EditorialSheila GouveiaNo ratings yet
- A Practical Approach To Diagnose and Treat Rickets: Journal of Clinical Medicine of Kazakhstan (E-ISSN 2313-1519)Document7 pagesA Practical Approach To Diagnose and Treat Rickets: Journal of Clinical Medicine of Kazakhstan (E-ISSN 2313-1519)goppalNo ratings yet
- The Role of Inflammation in Chronic Kidney DiseaseDocument10 pagesThe Role of Inflammation in Chronic Kidney Diseasesarah alatasNo ratings yet
- Analysis of Association of Vitamin D3, Hemoglobin and Ferritin With Special Respect To Libyan PatientsDocument5 pagesAnalysis of Association of Vitamin D3, Hemoglobin and Ferritin With Special Respect To Libyan PatientsMediterr J Pharm Pharm SciNo ratings yet
- Vitamin D: An Evidence-Based ReviewDocument9 pagesVitamin D: An Evidence-Based ReviewWill TohallinoNo ratings yet
- Accepted Manuscript: 10.1016/j.ghir.2017.02.002Document35 pagesAccepted Manuscript: 10.1016/j.ghir.2017.02.002mammon mammonovNo ratings yet
- The Evolving Role of Selenium in The Treatment of PDFDocument7 pagesThe Evolving Role of Selenium in The Treatment of PDFAkun TerorNo ratings yet
- 8 PDFDocument8 pages8 PDFSofia FurtadoNo ratings yet
- Ijpab 2017 5 6 208 214 PDFDocument7 pagesIjpab 2017 5 6 208 214 PDFDrRameem BlochNo ratings yet
- Vitamin D and Thyroid Disease: To D or Not To D?: Mini ReviewDocument6 pagesVitamin D and Thyroid Disease: To D or Not To D?: Mini Reviewmammon mammonovNo ratings yet
- 2019 Article 1840 PDFDocument18 pages2019 Article 1840 PDFmammon mammonovNo ratings yet
- Vitamin D and Growth Hormone in Children: A Review of The Current Scientific KnowledgeDocument18 pagesVitamin D and Growth Hormone in Children: A Review of The Current Scientific Knowledgemammon mammonovNo ratings yet
- 2019 - Benefit Risk Balance of Native Vitamin D Supplementation in Chronic Hemodialysis What Can We Learn From The Major Clinical Trials and InternationalDocument10 pages2019 - Benefit Risk Balance of Native Vitamin D Supplementation in Chronic Hemodialysis What Can We Learn From The Major Clinical Trials and InternationalMg GfNo ratings yet
- 10.1038@s41598 019 51498 XDocument8 pages10.1038@s41598 019 51498 XJTNo ratings yet
- Narsum 3. Peran Mikronutrien Pada Pasien Dengan Sindrom MetabolikDocument22 pagesNarsum 3. Peran Mikronutrien Pada Pasien Dengan Sindrom MetabolikbimaNo ratings yet
- Protective HistidineDocument15 pagesProtective HistidinenizaNo ratings yet
- New Insights About Vitamin D and CV DiseaseDocument8 pagesNew Insights About Vitamin D and CV DiseaseMario LosadaNo ratings yet
- Use of Vitamin D in Clinical Practice: Review ArticleDocument15 pagesUse of Vitamin D in Clinical Practice: Review ArticleBimantoro SaputroNo ratings yet
- Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding QuestionsDocument43 pagesSkeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding QuestionsLetícia ScalioniNo ratings yet
- Chowdhury, 2018Document19 pagesChowdhury, 2018Ruth WibowoNo ratings yet
- Saponaro, 2020Document19 pagesSaponaro, 2020Ruth WibowoNo ratings yet
- Review Article: Malignant Pleural Effusion: Diagnosis and ManagementDocument11 pagesReview Article: Malignant Pleural Effusion: Diagnosis and ManagementRuth WibowoNo ratings yet
- Shuey, 2005Document2 pagesShuey, 2005Ruth WibowoNo ratings yet
- Antony, 2001Document18 pagesAntony, 2001Ruth WibowoNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleRuth WibowoNo ratings yet
- Journal Pre-Proof: American Journal of OphthalmologyDocument14 pagesJournal Pre-Proof: American Journal of OphthalmologyRuth WibowoNo ratings yet
- Ophthalmology and Ethics in The COVID-19 Era: ErspectiveDocument5 pagesOphthalmology and Ethics in The COVID-19 Era: ErspectiveRuth WibowoNo ratings yet
- A Surgical Technique To Repair Perineal Body Disruption Secondary To Sexual AssaultDocument5 pagesA Surgical Technique To Repair Perineal Body Disruption Secondary To Sexual AssaultRuth WibowoNo ratings yet
- Review Article: Intravitreal Therapy For Diabetic Macular Edema: An UpdateDocument23 pagesReview Article: Intravitreal Therapy For Diabetic Macular Edema: An UpdateRuth WibowoNo ratings yet
- Dermatological Indications and Usage of Topical CorticosteroidDocument18 pagesDermatological Indications and Usage of Topical CorticosteroidRuth WibowoNo ratings yet
- Nutraceuticals in Te Prevention of Viral Infection Includin COVID-19Document25 pagesNutraceuticals in Te Prevention of Viral Infection Includin COVID-19David VázquezNo ratings yet
- MANOJ KHERAJANI-Male50 Years-12446Document3 pagesMANOJ KHERAJANI-Male50 Years-12446dr.menganeNo ratings yet
- Vitamin D Deficiency Among Patients With COVID-19: Case Series and Recent Literature ReviewDocument7 pagesVitamin D Deficiency Among Patients With COVID-19: Case Series and Recent Literature ReviewA A Christina AquerilaNo ratings yet
- Liver and Liver Transplant Program Nutrition GuidelinesDocument15 pagesLiver and Liver Transplant Program Nutrition GuidelinesRobert G. Gish, MDNo ratings yet
- Vitamin D Deficiency and Its Repletion A Review 2167 7921.1000105Document11 pagesVitamin D Deficiency and Its Repletion A Review 2167 7921.1000105octusNo ratings yet
- Prevention & Early Outpatient Treatment Protocol For Covid-19Document4 pagesPrevention & Early Outpatient Treatment Protocol For Covid-19jack mehiffNo ratings yet
- Vitamind Sohailfinal 151116051750 Lva1 App6892Document104 pagesVitamind Sohailfinal 151116051750 Lva1 App6892Umema ZafarNo ratings yet
- Vitamin D Deficiency Metabolism and Routine Measurement of Itsmetabolites 25ohd2 and 25ohd3 2157 7064 1000276Document5 pagesVitamin D Deficiency Metabolism and Routine Measurement of Itsmetabolites 25ohd2 and 25ohd3 2157 7064 1000276anandita putriNo ratings yet
- MayoTestCatalog Rochester SortedByTestName Duplex InterpretiveDocument2,763 pagesMayoTestCatalog Rochester SortedByTestName Duplex InterpretiveLaboratorium RS BELLANo ratings yet
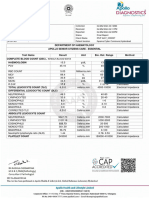
- Apollo247 250313622 Labreport 220 1709549589491Document4 pagesApollo247 250313622 Labreport 220 1709549589491mariarubyjohn18No ratings yet
- Optimalisasi Imunitas Di Masa Pandemi Covid-19Document13 pagesOptimalisasi Imunitas Di Masa Pandemi Covid-19renybejoNo ratings yet
- I CARE Early COVID Protocol 2023 03 30Document34 pagesI CARE Early COVID Protocol 2023 03 30BugMagnetNo ratings yet
- Vitamin D and Skin Diseases - A ReviewDocument12 pagesVitamin D and Skin Diseases - A ReviewMai Anh NguyễnNo ratings yet
- Avian ExaminerDocument24 pagesAvian ExaminerJojo GaranganaoNo ratings yet
- ReportDocument16 pagesReportprachiNo ratings yet
- JPNR - S09 - 1114Document7 pagesJPNR - S09 - 1114arunkumar kumararunNo ratings yet
- CCM TabletsDocument9 pagesCCM TabletssajantkNo ratings yet
- Vitamin D Deficiency ThesisDocument4 pagesVitamin D Deficiency Thesisangelagibbsdurham100% (2)
- Vitamin D Effects On Pregnancy and The PlacentaDocument8 pagesVitamin D Effects On Pregnancy and The Placentayoga paripurnaNo ratings yet
- Vitamin D Metabolism... Mechanism of Action and Clinical Appllications.Document11 pagesVitamin D Metabolism... Mechanism of Action and Clinical Appllications.asalizwa ludlalaNo ratings yet
- F8.full Vitamina D ReviewDocument21 pagesF8.full Vitamina D ReviewGabriela ValarezoNo ratings yet
- Lesson 8 - Vitamin D and Health - The Missing Vitamin in Humans - pp.1-3Document3 pagesLesson 8 - Vitamin D and Health - The Missing Vitamin in Humans - pp.1-3Cláudia FranzãoNo ratings yet
- ChandanKumar 632972Document11 pagesChandanKumar 632972Chandan JhaNo ratings yet
- Combating COVID-19 and Building Immune Resilience: A Potential Role For Magnesium Nutrition?Document10 pagesCombating COVID-19 and Building Immune Resilience: A Potential Role For Magnesium Nutrition?witaNo ratings yet
- Vit DDocument36 pagesVit DConstantin MarioaraNo ratings yet
- Vitamin D SupplementsDocument11 pagesVitamin D SupplementsPetra JobovaNo ratings yet