You might also like
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 1 out of 5 stars1/5 (1)
- PYELONEPHRITISDocument16 pagesPYELONEPHRITISshenecajean carajayNo ratings yet
- Cholelithiasis When They Are in The Bile CholedocolithiasisDocument15 pagesCholelithiasis When They Are in The Bile Choledocolithiasishisabumohamed100% (1)
- GIT History ReportDocument4 pagesGIT History ReportYan Chan HaoNo ratings yet
- Case Presentation - GASTRODocument46 pagesCase Presentation - GASTROalidudeNo ratings yet
- Urinary Tract InfectionsDocument43 pagesUrinary Tract InfectionsAlishba MushtaqNo ratings yet
- CaseStudyTuberculosis Quindala TanoDocument102 pagesCaseStudyTuberculosis Quindala TanoLiz G. QuindalaNo ratings yet
- Case Report 2 - Ovarian CystDocument9 pagesCase Report 2 - Ovarian CystA MNo ratings yet
- Pathophysiology of GERD and Its ComplicationDocument25 pagesPathophysiology of GERD and Its ComplicationalmiraNo ratings yet
- APPENDICITISDocument69 pagesAPPENDICITISKim Alvarez100% (1)
- Grand ReportsDocument60 pagesGrand ReportsfilchibuffNo ratings yet
- Case Presentation CKDDocument35 pagesCase Presentation CKDKojo EgyirNo ratings yet
- Multinodular Goitre Case PresentationDocument19 pagesMultinodular Goitre Case PresentationTamilNo ratings yet
- Case Study On Angina PectorisDocument4 pagesCase Study On Angina Pectorismahi0% (1)
- HEPATOMEGALY CaseDocument5 pagesHEPATOMEGALY CaseKanwaljeet SinghNo ratings yet
- Case Writeup Albert Labores 9.24.2010 StrokeDocument6 pagesCase Writeup Albert Labores 9.24.2010 StrokeAJ RegaladoNo ratings yet
- GLOMERULONEPHRITIS (Bright's Disease)Document8 pagesGLOMERULONEPHRITIS (Bright's Disease)Anjitha K. JNo ratings yet
- CystitisDocument13 pagesCystitisTin VidovićNo ratings yet
- PCGH Opd Case Write UpDocument3 pagesPCGH Opd Case Write Uplionheart_gtrNo ratings yet
- Case Scenerio Nephrotic SyndromeDocument4 pagesCase Scenerio Nephrotic SyndromeEllen AngelNo ratings yet
- Nephrotic Syndrome: Dinesh Kumar PDocument42 pagesNephrotic Syndrome: Dinesh Kumar PRiya Sweetsolitude100% (1)
- Iga Nephropathy and Vasculitis: Dr. Rida Malik Nephrology ResidentDocument52 pagesIga Nephropathy and Vasculitis: Dr. Rida Malik Nephrology ResidentDr Rida And Shoaib VideosNo ratings yet
- Management of Patient With Meningitis and Encephalitis: ModeratorDocument71 pagesManagement of Patient With Meningitis and Encephalitis: ModeratorSachin DwivediNo ratings yet
- Cholecystitis: Bonoan, Camille Grace Chua, ManilynDocument29 pagesCholecystitis: Bonoan, Camille Grace Chua, ManilynCams BonoanNo ratings yet
- Long Case PresentationDocument3 pagesLong Case PresentationAkshat WaranNo ratings yet
- Case Write Up FibroidDocument17 pagesCase Write Up FibroidNadsri AmirNo ratings yet
- How Low Can You Endure The Pain, Mr. Bond?Document70 pagesHow Low Can You Endure The Pain, Mr. Bond?Venny VeronicaNo ratings yet
- Non Viral HepatitisDocument8 pagesNon Viral HepatitisKeith Wesley YbutNo ratings yet
- Pediatrics 2 LaboratoryDocument40 pagesPediatrics 2 LaboratoryAmaetenNo ratings yet
- Alcoholic Liver DiseaseDocument21 pagesAlcoholic Liver DiseaseInsta GrammerNo ratings yet
- Case Presentation: Paediatrics: by Tapan Jyoti Saikia 8 Sem Gauhati Medical CollegeDocument22 pagesCase Presentation: Paediatrics: by Tapan Jyoti Saikia 8 Sem Gauhati Medical CollegeArpit Mehta100% (1)
- Case Presentation: DR - Anbalagan II ND Year MEMDocument20 pagesCase Presentation: DR - Anbalagan II ND Year MEMDr mahi sNo ratings yet
- Large Bowel Obstruction by Nic MDocument42 pagesLarge Bowel Obstruction by Nic MRisky OpponentNo ratings yet
- Peptic Ulcer DiseaseDocument1 pagePeptic Ulcer DiseasecesiexieNo ratings yet
- Nephrotic SyndromeDocument56 pagesNephrotic SyndromeMurugesan100% (1)
- Pediatric Case StudyDocument29 pagesPediatric Case Studyapi-296281683No ratings yet
- History:: Chief Complaint: History of Present IllnessDocument4 pagesHistory:: Chief Complaint: History of Present IllnessIbrahem Y. NajjarNo ratings yet
- Renal Failure PresentationDocument110 pagesRenal Failure PresentationMusa yohana100% (1)
- Case Presentation Lump Right HypochondriumDocument22 pagesCase Presentation Lump Right HypochondriumNANDAN RAINo ratings yet
- Case Presentation Hernia 1 PDFDocument21 pagesCase Presentation Hernia 1 PDFMvs ramuNo ratings yet
- BPHDocument25 pagesBPHsurya mertayasaNo ratings yet
- Renal Failur E: Mamta Kumari Asst - Prof. Igims-ConDocument51 pagesRenal Failur E: Mamta Kumari Asst - Prof. Igims-ConMamta KumariNo ratings yet
- Case Presentation On MalariaDocument13 pagesCase Presentation On Malarialavate amol bhimraoNo ratings yet
- Case Write Up 1: Dengue Haemorrhagic Fever Saarah Huurieyah BT Wan Rosli 1050024 Year 4 Internal MedicineDocument16 pagesCase Write Up 1: Dengue Haemorrhagic Fever Saarah Huurieyah BT Wan Rosli 1050024 Year 4 Internal MedicineRoshandiep GillNo ratings yet
- Case Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Document49 pagesCase Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Izaac JdevNo ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- AppendicitisDocument49 pagesAppendicitisSeisa GumelarNo ratings yet
- Case Presentation On Copd: By, Thomas Eipe Pharm D InternDocument32 pagesCase Presentation On Copd: By, Thomas Eipe Pharm D InternThomas EipeNo ratings yet
- Benign Prostatic Hypertrophy: Pathophysiology and EtiologyDocument4 pagesBenign Prostatic Hypertrophy: Pathophysiology and EtiologyErnestomalamionNo ratings yet
- Bronchitis ReportDocument34 pagesBronchitis ReportRolinette DaneNo ratings yet
- Pud Case StudyDocument8 pagesPud Case Studyapi-346620455No ratings yet
- Acute Gastroenteritis in Paediatrics 1Document43 pagesAcute Gastroenteritis in Paediatrics 1Imran FaisalNo ratings yet
- Case Write-Up 2 - Suba Ramasamy (SB323827)Document29 pagesCase Write-Up 2 - Suba Ramasamy (SB323827)Bavithiran KaruppiahNo ratings yet
- Tracheoesophageal FistulaDocument6 pagesTracheoesophageal FistulaPankaj SinghNo ratings yet
- BPHDocument81 pagesBPHFlo Neri BerondoNo ratings yet
- Nephrology - Proteinuria - SOAP Note - Manish Suneja PDFDocument4 pagesNephrology - Proteinuria - SOAP Note - Manish Suneja PDFΝίκος ΣυρίγοςNo ratings yet
- TonsilitisDocument31 pagesTonsilitisJayson King Legaspi CruzNo ratings yet
- Case StudyDocument84 pagesCase Studyalcojonic0% (1)
- Diagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDocument8 pagesDiagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDiskta W RonicaNo ratings yet
- Gastroesophageal Reflux: Natural Evolution, Diagnostic Approach and TreatmentDocument7 pagesGastroesophageal Reflux: Natural Evolution, Diagnostic Approach and TreatmentYanis Widhiya NingrumNo ratings yet
- The Clinical Implications of Adult-Onset Henoch-Schonelin PurpuraDocument7 pagesThe Clinical Implications of Adult-Onset Henoch-Schonelin PurpuraAndhika DNo ratings yet
- Factors Associated With 30-Day Readmission For Patients Hospitalized For SeizuresDocument10 pagesFactors Associated With 30-Day Readmission For Patients Hospitalized For SeizuresAndhika DNo ratings yet
- Attention Disorders in Adults With Epilepsy. Determinants and Therapeutic StrategiesDocument6 pagesAttention Disorders in Adults With Epilepsy. Determinants and Therapeutic StrategiesAndhika DNo ratings yet
- Heart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesDocument10 pagesHeart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesAndhika DNo ratings yet
- Riginal Tudy: Sexually Transmitted Diseases Volume 43, Number 10, October 2016Document9 pagesRiginal Tudy: Sexually Transmitted Diseases Volume 43, Number 10, October 2016Andhika DNo ratings yet
- Chest: Passive Smoking Exposure Is Associated With Increased Risk of COPD in Never SmokersDocument7 pagesChest: Passive Smoking Exposure Is Associated With Increased Risk of COPD in Never SmokersAndhika DNo ratings yet
- Risk Factors For Hypertension Among Young Adults (18-35) YearsDocument8 pagesRisk Factors For Hypertension Among Young Adults (18-35) YearsAndhika DNo ratings yet
- The Prevalence and Risk Factors of Type 2 Diabetes Mellitus (DMT2) in A Semi-Urban Saudi PopulationDocument8 pagesThe Prevalence and Risk Factors of Type 2 Diabetes Mellitus (DMT2) in A Semi-Urban Saudi PopulationAndhika DNo ratings yet
- Prevalence of Depression Symptoms in US Adults Before and During The COVID-19 PandemicDocument12 pagesPrevalence of Depression Symptoms in US Adults Before and During The COVID-19 PandemicAndhika DNo ratings yet
- Preview 2Document1 pagePreview 2Andhika DNo ratings yet
- Effects of COVID-19 On College Students' Mental Health in The United States: Interview Survey StudyDocument14 pagesEffects of COVID-19 On College Students' Mental Health in The United States: Interview Survey StudyAndhika DNo ratings yet
- Chap 37Document13 pagesChap 37buatadekNo ratings yet
- Botulism Is A Serious Illness Caused by The Botulinum ToxinDocument10 pagesBotulism Is A Serious Illness Caused by The Botulinum ToxinReyNo ratings yet
- ZZ Infrastructure Sector - WebpubDocument65 pagesZZ Infrastructure Sector - WebpubJennyvil NuñezNo ratings yet
- Hydrometeorological Hazard StudentDocument26 pagesHydrometeorological Hazard StudentMargaret Nicole100% (1)
- The Persons With Disabilities 1995Document27 pagesThe Persons With Disabilities 1995siva ramanNo ratings yet
- Gene Regulation: Made By: Diana Alhazzaa Massah AlhazzaaDocument17 pagesGene Regulation: Made By: Diana Alhazzaa Massah AlhazzaaAmora HZzNo ratings yet
- Acupuntura - GráficosDocument41 pagesAcupuntura - GráficosHeribertoNo ratings yet
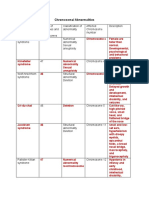
- Table On Chromosomal AbnormalitiesDocument3 pagesTable On Chromosomal AbnormalitiesJoanne Mary RomoNo ratings yet
- TNPIndianaDocument8 pagesTNPIndianaInes Arias PazNo ratings yet
- Swedish Neutral Neutral Earthing Resistor Specification PDFDocument12 pagesSwedish Neutral Neutral Earthing Resistor Specification PDFRazvan CostacheNo ratings yet
- JHA 12 - Complete - 4 CopiesDocument15 pagesJHA 12 - Complete - 4 CopiesSaravanan krishnanNo ratings yet
- AstmDocument5 pagesAstmandresNo ratings yet
- Freeman Aortic RegurgitationDocument102 pagesFreeman Aortic RegurgitationJose Ignacio Tarton SisimitNo ratings yet
- Squash (Cucurbita Pepo L.) Growth and Yield in Response To Different Types of Fertilizers (Farmyard, Chicken Manures, Urea and NPK Granules) PDFDocument112 pagesSquash (Cucurbita Pepo L.) Growth and Yield in Response To Different Types of Fertilizers (Farmyard, Chicken Manures, Urea and NPK Granules) PDFJonabelleVictorianoNo ratings yet
- Chapter 4 Case StudyDocument2 pagesChapter 4 Case StudyPrafulla Man PradhanNo ratings yet
- Schuetziana 5 2014 1Document41 pagesSchuetziana 5 2014 1Vladimir RadenkovicNo ratings yet
- Suicide by Firearm Toolkit For ChangeDocument28 pagesSuicide by Firearm Toolkit For ChangeSara WilliamsNo ratings yet
- Tony Robbins - The Power of LeverageDocument8 pagesTony Robbins - The Power of Leverageabbaslasania98% (42)
- Database AdministratorDocument3 pagesDatabase Administratorapi-78697982No ratings yet
- Basic Principles of Animal Form and Function: For Campbell Biology, Ninth EditionDocument66 pagesBasic Principles of Animal Form and Function: For Campbell Biology, Ninth EditionASEEL AHMADNo ratings yet
- Granda-Ramírez2017 Article DegradationOfRecalcitrantSafraDocument12 pagesGranda-Ramírez2017 Article DegradationOfRecalcitrantSafraLeidy StefanyNo ratings yet
- Answers For Practice Problems in Lesson 5: Practice Problem #1: Specific Gravity Calculation For Coarse AggregateDocument2 pagesAnswers For Practice Problems in Lesson 5: Practice Problem #1: Specific Gravity Calculation For Coarse AggregateDjonraeNarioGalvezNo ratings yet
- Convergent Plate BoundariesDocument45 pagesConvergent Plate Boundariesjherwinperez2007No ratings yet
- Taxation ProjectDocument23 pagesTaxation ProjectAkshata MasurkarNo ratings yet
- Flood Mitigation in AssamDocument4 pagesFlood Mitigation in AssamAnju ParmarNo ratings yet
- GeoCon DavaodelEq Jsperez 02dec2020Document22 pagesGeoCon DavaodelEq Jsperez 02dec2020Kym Buena-RegadoNo ratings yet
- Key Competence Diagnostic Tests: PrimaryDocument13 pagesKey Competence Diagnostic Tests: PrimaryebumbahotmaicomNo ratings yet
- Possums 1Document6 pagesPossums 1tillyannNo ratings yet
- (Way People Live) Keeley, Jennifer - The Way People Live - Life in The Hitler Youth (2000, Lucent Books)Document118 pages(Way People Live) Keeley, Jennifer - The Way People Live - Life in The Hitler Youth (2000, Lucent Books)Ciprian CipNo ratings yet
- Chapter 1Document6 pagesChapter 1kenetic0186% (7)
- The Storyteller: Expanded: ...Because There's More to the StoryFrom EverandThe Storyteller: Expanded: ...Because There's More to the StoryRating: 5 out of 5 stars5/5 (13)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (158)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (251)
- Bare Bones: I'm Not Lonely If You're Reading This BookFrom EverandBare Bones: I'm Not Lonely If You're Reading This BookRating: 4 out of 5 stars4/5 (11)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (141)
- Summary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisFrom EverandSummary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (6)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)