You might also like
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Case Write Up 1: Dengue Haemorrhagic Fever Saarah Huurieyah BT Wan Rosli 1050024 Year 4 Internal MedicineDocument16 pagesCase Write Up 1: Dengue Haemorrhagic Fever Saarah Huurieyah BT Wan Rosli 1050024 Year 4 Internal MedicineRoshandiep GillNo ratings yet
- Toxic multinodular goiter exam findingsDocument2 pagesToxic multinodular goiter exam findingsAngie MandeoyaNo ratings yet
- Peds Case 3Document5 pagesPeds Case 3Mohammed AhmedNo ratings yet
- Patient Medical ReportDocument20 pagesPatient Medical ReportDimpal ChoudharyNo ratings yet
- Surgery 2 Case ReportDocument12 pagesSurgery 2 Case ReportElvis NgNo ratings yet
- Internal Medicine Write Up 1Document16 pagesInternal Medicine Write Up 1Ariff MahdzubNo ratings yet
- CaseStudyTuberculosis Quindala TanoDocument102 pagesCaseStudyTuberculosis Quindala TanoLiz G. QuindalaNo ratings yet
- PATIENT's ProfileDocument9 pagesPATIENT's Profilerockeyci28No ratings yet
- Preterm Contraction History ReviewDocument19 pagesPreterm Contraction History ReviewAiman ArifinNo ratings yet
- Community-Acquired Pneumonia DiagnosisDocument102 pagesCommunity-Acquired Pneumonia DiagnosisJay Kumar100% (1)
- Surgery Case AppendicitisDocument30 pagesSurgery Case AppendicitisSarahNo ratings yet
- History Taking OBS GYNDocument10 pagesHistory Taking OBS GYNzvkznhsw2tNo ratings yet
- Tuberculosis and Nephrotic Syndrome in a ChildDocument34 pagesTuberculosis and Nephrotic Syndrome in a ChildAldo YustiantoNo ratings yet
- Case Presentation On Copd: By, Thomas Eipe Pharm D InternDocument32 pagesCase Presentation On Copd: By, Thomas Eipe Pharm D InternThomas EipeNo ratings yet
- Neonatal Case Presentation-1Document16 pagesNeonatal Case Presentation-1Ananya SampathNo ratings yet
- Epilepsy CaseDocument17 pagesEpilepsy CaseSuresh ThanneruNo ratings yet
- Case Report MartaDocument10 pagesCase Report MartadenekeNo ratings yet
- 2.APH 2 To PP + Multiple Myoma + PreeclampsiaDocument14 pages2.APH 2 To PP + Multiple Myoma + PreeclampsiaBerhanu Digamo100% (1)
- Case Write Up FibroidDocument17 pagesCase Write Up FibroidNadsri AmirNo ratings yet
- Essential HTN in PregnancyDocument13 pagesEssential HTN in PregnancyAiman ArifinNo ratings yet
- Pancreatic CancerDocument15 pagesPancreatic CancerMutiana Muspita JeliNo ratings yet
- Ong Case Sheet Sem7Document13 pagesOng Case Sheet Sem7Uchiha AnzarNo ratings yet
- Collin Grimes Patient Write Up June 14Document4 pagesCollin Grimes Patient Write Up June 14CollinNo ratings yet
- Case Write Up Obstetrics Gestational Diabetes MellitusDocument13 pagesCase Write Up Obstetrics Gestational Diabetes MellitusRoshandiep GillNo ratings yet
- Managing Hypertension in PregnancyDocument18 pagesManaging Hypertension in PregnancyAiman ArifinNo ratings yet
- Case Discussion-FibroidDocument17 pagesCase Discussion-FibroidNazee NazreenNo ratings yet
- Presentation of Nephrotic Syndrome ICKADocument16 pagesPresentation of Nephrotic Syndrome ICKABagas NovandyNo ratings yet
- Chief ComplaintDocument10 pagesChief ComplaintVivekanandaNo ratings yet
- Multinodular Goitre Case PresentationDocument19 pagesMultinodular Goitre Case PresentationTamilNo ratings yet
- Case Presentation On MalariaDocument13 pagesCase Presentation On Malarialavate amol bhimraoNo ratings yet
- PEDIA Case 3.1. Acute BronchiolitisDocument75 pagesPEDIA Case 3.1. Acute Bronchiolitisotartil_nimanNo ratings yet
- Name: Wong Wai Kheong Matrix No: BMS12081154Document13 pagesName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNo ratings yet
- Nursing Process 3Document10 pagesNursing Process 3Shubhra Sheoran100% (1)
- ICU Case: Septic Shock from Hospital-Acquired PneumoniaDocument13 pagesICU Case: Septic Shock from Hospital-Acquired PneumoniaHana FauziNo ratings yet
- PEDIATRICS CASEDocument12 pagesPEDIATRICS CASEAmaetenNo ratings yet
- Case Write-Up 2 - Suba Ramasamy (SB323827)Document29 pagesCase Write-Up 2 - Suba Ramasamy (SB323827)Bavithiran KaruppiahNo ratings yet
- Case StudyDocument84 pagesCase Studyalcojonic0% (1)
- Epilepsy in ChildhoodDocument20 pagesEpilepsy in ChildhoodRizky Indah SorayaNo ratings yet
- My Cwu OphthalDocument16 pagesMy Cwu OphthalSalsabila Al-BasheerNo ratings yet
- Difficulty in Speech After StrokeDocument6 pagesDifficulty in Speech After StrokeAJ RegaladoNo ratings yet
- Case Presentation CKDDocument35 pagesCase Presentation CKDKojo EgyirNo ratings yet
- Everything You Need to Know About Anemia in PregnancyDocument9 pagesEverything You Need to Know About Anemia in PregnancyAiman ArifinNo ratings yet
- History:: Chief Complaint: History of Present IllnessDocument4 pagesHistory:: Chief Complaint: History of Present IllnessIbrahem Y. NajjarNo ratings yet
- How Phototherapy WorksDocument4 pagesHow Phototherapy WorksmaramNo ratings yet
- Case ReportDocument19 pagesCase ReportvivitaslimNo ratings yet
- Seminar 2 (Paeds)Document31 pagesSeminar 2 (Paeds)Jonathan YeohNo ratings yet
- Cirrhosis Case For PrintingDocument12 pagesCirrhosis Case For PrintingSean Mercado100% (1)
- IUFDDocument33 pagesIUFDIrwin FitriansyahNo ratings yet
- Pediatric Case PresentationDocument71 pagesPediatric Case PresentationJoan Luis100% (1)
- Management of patients with meningitis and encephalitisDocument71 pagesManagement of patients with meningitis and encephalitisSachin DwivediNo ratings yet
- Case Study of Renal FailurDocument15 pagesCase Study of Renal FailurYousef Jafar0% (1)
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- Case Write Up on Moderate Acne VulgarisDocument9 pagesCase Write Up on Moderate Acne VulgarisAmbhi GanaNo ratings yet
- Case Presentation On Pharyngitis2Document10 pagesCase Presentation On Pharyngitis2kamini ChoudharyNo ratings yet
- Sharon Owuor Case Study Rh1Document19 pagesSharon Owuor Case Study Rh1Kuto Yvonne CheronoNo ratings yet
- Decompensated Liver DiseaseDocument16 pagesDecompensated Liver Diseasedk.clinicalresearchNo ratings yet
- Gestational Diabetes MellitusDocument9 pagesGestational Diabetes MellitusAiman ArifinNo ratings yet
- Case Write 5 ObgynDocument7 pagesCase Write 5 ObgynMaryam AlahbabiNo ratings yet
- CASE REPORT ON MYOMA UTERINEDocument12 pagesCASE REPORT ON MYOMA UTERINENiki Rizqi rachmawatiNo ratings yet
- Case 5 NotesDocument16 pagesCase 5 NotesA MNo ratings yet
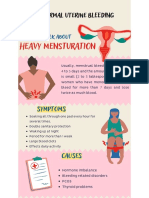
- Heavy Mensturation: Abnormal Uterine BLEEDINGDocument1 pageHeavy Mensturation: Abnormal Uterine BLEEDINGA MNo ratings yet
- Case Report Preterm LaborDocument12 pagesCase Report Preterm LaborA MNo ratings yet
- CBD 5 - NstemiDocument11 pagesCBD 5 - NstemiA MNo ratings yet
- Lower Limb WeaknessDocument15 pagesLower Limb WeaknessA MNo ratings yet
- Case Write-Up Influenza ADocument17 pagesCase Write-Up Influenza AA MNo ratings yet
- Psych Discharge SummaryDocument5 pagesPsych Discharge SummaryA MNo ratings yet
- Case Write UpDocument10 pagesCase Write UpA MNo ratings yet
- Casewrite Up CellulitisDocument10 pagesCasewrite Up CellulitisA MNo ratings yet
- Hashimoto's Thyroiditis: Causes, Symptoms, and TreatmentDocument10 pagesHashimoto's Thyroiditis: Causes, Symptoms, and TreatmentSan RedkarNo ratings yet
- Black's Veterinary DictionaryDocument801 pagesBlack's Veterinary DictionaryGeorgiana Rosu88% (8)
- Enterovirus 71 Outbreaks, Taiwan: Occurrence and RecognitionDocument3 pagesEnterovirus 71 Outbreaks, Taiwan: Occurrence and RecognitionAdhi SyukriNo ratings yet
- Delivery DrugsDocument2 pagesDelivery DrugsBernardNo ratings yet
- Lung Anatomy Physiology PDFDocument6 pagesLung Anatomy Physiology PDFCharmie GandaNo ratings yet
- Clear Coughs with EOs and PhysiotherapyDocument19 pagesClear Coughs with EOs and PhysiotherapyAleen ZakiNo ratings yet
- DADS - Solutions For Anxiety & Depression E-BookDocument18 pagesDADS - Solutions For Anxiety & Depression E-BookChristine DaaéNo ratings yet
- Introduction A&sDocument7 pagesIntroduction A&sMajaNo ratings yet
- Intoxicación Por VoriconazolDocument2 pagesIntoxicación Por VoriconazolMariana fotos FotosNo ratings yet
- Myeloproliferative Neoplasms: Diagnostic Workup of The Cythemic PatientDocument9 pagesMyeloproliferative Neoplasms: Diagnostic Workup of The Cythemic PatientHashim AhmadNo ratings yet
- Depictions of Mental Health Topics in Malayalam CinemaDocument8 pagesDepictions of Mental Health Topics in Malayalam Cinemagion.nandNo ratings yet
- MAALOX (Drug Study)Document3 pagesMAALOX (Drug Study)Kian HerreraNo ratings yet
- Guidelines For Preventive Activities in General PracticeDocument382 pagesGuidelines For Preventive Activities in General PracticeDr. Serin KuriakoseNo ratings yet
- Chronic Pain-2Document5 pagesChronic Pain-2api-549219188No ratings yet
- Kyyrönen IidaDocument114 pagesKyyrönen IidaNopri JayaNo ratings yet
- Chapter1 Abnormal PsychologyDocument10 pagesChapter1 Abnormal PsychologyKAYLE NICOLE ILIJAYNo ratings yet
- Public Health Emergency Management GuidelinesDocument140 pagesPublic Health Emergency Management GuidelinesAbbi NathiNo ratings yet
- Renal ColicDocument14 pagesRenal ColicIsabela OlgaNo ratings yet
- MCQs From All Subjects For Medical PG EntranceDocument16 pagesMCQs From All Subjects For Medical PG EntranceEMIN3MNo ratings yet
- Gout Presentation Group 2 Defines Metabolic Disorder and ManagementDocument10 pagesGout Presentation Group 2 Defines Metabolic Disorder and ManagementVon Valentine MhuteNo ratings yet
- Heartburn, Acid Reflux, or GERD (Gastroesophageal Reflux Disease) Are Probably Some of The Most Common Diseases in The WorldDocument5 pagesHeartburn, Acid Reflux, or GERD (Gastroesophageal Reflux Disease) Are Probably Some of The Most Common Diseases in The WorldDrake SuyatNo ratings yet
- Arterial Tortuosity SyndromeDocument11 pagesArterial Tortuosity SyndromeNawal RaiNo ratings yet
- Trigeminal Neuralgia - Diagnosis and Treatment: Stine Maarbjerg, Giulia Di Stefano, Lars Bendtsen and Giorgio CruccuDocument10 pagesTrigeminal Neuralgia - Diagnosis and Treatment: Stine Maarbjerg, Giulia Di Stefano, Lars Bendtsen and Giorgio CruccuAjeng RetnoNo ratings yet
- Eosinophilic Granulomatosis With Polyangiitis Complete ArticleDocument7 pagesEosinophilic Granulomatosis With Polyangiitis Complete ArticleVeronicaNo ratings yet
- Krok 2 Stomatology: Test Items For Licensing ExaminationDocument30 pagesKrok 2 Stomatology: Test Items For Licensing ExaminationjimmyNo ratings yet
- Toprank Nursing: Patrick Migel Mercado, RNDocument126 pagesToprank Nursing: Patrick Migel Mercado, RNNoreen PadillaNo ratings yet
- Patient Identification and Care PlanDocument8 pagesPatient Identification and Care Plananimesh panda100% (3)
- Root Canal Cover-Up by MEINIG G - DesconhecidoDocument216 pagesRoot Canal Cover-Up by MEINIG G - DesconhecidoOswaldorfNo ratings yet
- Peripheral Nerve Injury in Upper LimbDocument29 pagesPeripheral Nerve Injury in Upper Limbvenkata ramakrishnaiahNo ratings yet
- Nelson MCQs BloodDocument16 pagesNelson MCQs Bloodshahera rosdi50% (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- CBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerFrom EverandCBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- How To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeFrom EverandHow To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Inmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedFrom EverandInmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)