You might also like
- Modele HealthDocument12 pagesModele HealthalelaNo ratings yet
- Internal and External Resources As Determinants of Health and Quality of LifeDocument9 pagesInternal and External Resources As Determinants of Health and Quality of LifenesquivelgNo ratings yet
- Do Better Health and Education Enhance Economic DevelopmentDocument15 pagesDo Better Health and Education Enhance Economic Developmentahmed_driouchiNo ratings yet
- New and Emerging Data Initiatives: Page 1 of 26Document26 pagesNew and Emerging Data Initiatives: Page 1 of 26Martinus PutraNo ratings yet
- The Association Between Physical Activity and Subjective Well-Being Among Adolescents in Southwest China by Parental Absence A Moderated Mediation ModelDocument21 pagesThe Association Between Physical Activity and Subjective Well-Being Among Adolescents in Southwest China by Parental Absence A Moderated Mediation ModelbarrylyuccNo ratings yet
- Lifestyle Factors and Psychological Well Being: 10 Year Follow Up Study in Lithuanian Urban PopulationDocument12 pagesLifestyle Factors and Psychological Well Being: 10 Year Follow Up Study in Lithuanian Urban PopulationSyed TouseefNo ratings yet
- Is Marital Status Associated With Quality of Life?: Research Open AccessDocument10 pagesIs Marital Status Associated With Quality of Life?: Research Open Accessmariya khanNo ratings yet
- An Impact of Perceived Social Support On Old AgeDocument18 pagesAn Impact of Perceived Social Support On Old Agekunto ajiNo ratings yet
- Health-Seeking Behaviour Studies: A Literature Review of Study Design and Methods With A Focus On CambodiaDocument17 pagesHealth-Seeking Behaviour Studies: A Literature Review of Study Design and Methods With A Focus On Cambodiakarl_poorNo ratings yet
- HealthcareDocument12 pagesHealthcareArgonne Robert AblanqueNo ratings yet
- Factors Influencing Health Knowledge and Behaviors Among The Elderly in Rural ChinaDocument17 pagesFactors Influencing Health Knowledge and Behaviors Among The Elderly in Rural ChinaDilaArdaNiNo ratings yet
- Health-Seeking Behaviour Studies: A Literature Review of Study Design and Methods With A Focus On Cambodia (WP7)Document17 pagesHealth-Seeking Behaviour Studies: A Literature Review of Study Design and Methods With A Focus On Cambodia (WP7)Nossal Institute for Global HealthNo ratings yet
- The Relationship Between Life Satisfaction and Health Behavior: A Cross-Cultural Analysis of Young AdultsDocument10 pagesThe Relationship Between Life Satisfaction and Health Behavior: A Cross-Cultural Analysis of Young AdultsJesus GuerreroNo ratings yet
- Job Satisfaction Work Stress and Turnover IntentioDocument11 pagesJob Satisfaction Work Stress and Turnover IntentioPeter GirasolNo ratings yet
- Living Alone (Depression)Document10 pagesLiving Alone (Depression)Lidwina DewiNo ratings yet
- 3,11205 2021 Article 2810Document24 pages3,11205 2021 Article 2810AZAM TARIQNo ratings yet
- Does Education Induce Healthy LifestyleDocument16 pagesDoes Education Induce Healthy LifestyleThiago HenriqueNo ratings yet
- Baidin2021 Article HowSelf RatedIsSelf RatedHealtDocument22 pagesBaidin2021 Article HowSelf RatedIsSelf RatedHealtGabriel MacielNo ratings yet
- Emerging Issues in Geriatric Care: Aging and Public Health PerspectivesDocument6 pagesEmerging Issues in Geriatric Care: Aging and Public Health PerspectiveslynhareeNo ratings yet
- Gender and Health - The Effects of Constrained Choices and Social Policies (PDFDrive)Document317 pagesGender and Health - The Effects of Constrained Choices and Social Policies (PDFDrive)Iness Billyon34No ratings yet
- Healing Across Cultures: Pathways to Indigenius Health EquityFrom EverandHealing Across Cultures: Pathways to Indigenius Health EquityNo ratings yet
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsFrom EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNo ratings yet
- Emerging Theories Into The Social Determinants of Health: Implications For Oral Health PromotionDocument7 pagesEmerging Theories Into The Social Determinants of Health: Implications For Oral Health PromotionEmmanuel PìnheiroNo ratings yet
- Nutrients 11 01224Document24 pagesNutrients 11 01224Alisa Nabila RahmahNo ratings yet
- SDOH Evidence ReviewDocument30 pagesSDOH Evidence ReviewKhalid AlhemyariNo ratings yet
- Health Economics of Obesity: A Cross-Cultural Examination of Markets and Psychographic FactorsFrom EverandHealth Economics of Obesity: A Cross-Cultural Examination of Markets and Psychographic FactorsNo ratings yet
- The Changing Demographic Profile of Eating Disorder Behaviors in The Community 2.23.16 PMDocument9 pagesThe Changing Demographic Profile of Eating Disorder Behaviors in The Community 2.23.16 PMShera LopezNo ratings yet
- Ijerph 19 13877 v2Document10 pagesIjerph 19 13877 v2jigyansa ipsitaNo ratings yet
- P3 Health StatusDocument9 pagesP3 Health StatusNovita Mariani GlekoNo ratings yet
- BPH UnderstandingTheRelationshipDocument25 pagesBPH UnderstandingTheRelationshipXiiAhnChoiPenjahatKunukNo ratings yet
- Written Assignment 2Document8 pagesWritten Assignment 2bnvjNo ratings yet
- Longitudinal Evidence On Social Trust and Happiness in China: Causal Effects and MechanismsDocument18 pagesLongitudinal Evidence On Social Trust and Happiness in China: Causal Effects and MechanismsPicolas CageNo ratings yet
- The Influence of Education On Health: An Empirical Assessment of OECD Countries For The Period 1995 - 2015Document18 pagesThe Influence of Education On Health: An Empirical Assessment of OECD Countries For The Period 1995 - 2015thyb2015571No ratings yet
- 2022 Depresi Lifestle KoreaDocument10 pages2022 Depresi Lifestle KoreaNhana IchsanNo ratings yet
- Research Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionFrom EverandResearch Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionNo ratings yet
- Ill-Health and Poverty A Literature Review On Health in Informal SettlementsDocument10 pagesIll-Health and Poverty A Literature Review On Health in Informal Settlementsc5m07hh9No ratings yet
- Ijerph 16 02592Document14 pagesIjerph 16 02592KikimariaNo ratings yet
- HSH207 ThiThuyTrangLY AT1Document9 pagesHSH207 ThiThuyTrangLY AT1Huong NguyenNo ratings yet
- How Does Social Development Influence Life Expectancy? A Geographically Weighted Regression Analysis in ChinaDocument10 pagesHow Does Social Development Influence Life Expectancy? A Geographically Weighted Regression Analysis in ChinaRizky Ahmad YudanegaraNo ratings yet
- Relationship Between Health LiDocument13 pagesRelationship Between Health Liarifrahman.fikNo ratings yet
- Gupta & Coffey 2020Document48 pagesGupta & Coffey 2020Indra WahyudiNo ratings yet
- 2015 - Article - 1020 Konsep Epidemiologi Sosial, Health SecvisDocument4 pages2015 - Article - 1020 Konsep Epidemiologi Sosial, Health SecvisYuly PeristiowatiNo ratings yet
- D. Bok (Ed) : The Politics of Happiness. What Government Can Learn From The New Research On Well-BeingDocument6 pagesD. Bok (Ed) : The Politics of Happiness. What Government Can Learn From The New Research On Well-BeingJames WeirNo ratings yet
- 2020 Article 352Document13 pages2020 Article 352miss betawiNo ratings yet
- FTADocument3 pagesFTAAlyssar GhandourNo ratings yet
- Income Health Poverty FullDocument70 pagesIncome Health Poverty FullGesler Pilvan SainNo ratings yet
- Religions 10 00532 v2Document16 pagesReligions 10 00532 v2Anne MonsaludNo ratings yet
- Gender Difference in The Association Between Education and Schizophrenia in Chinese AdultsDocument7 pagesGender Difference in The Association Between Education and Schizophrenia in Chinese AdultsFitri anaNo ratings yet
- Structural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of HealthFrom EverandStructural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of HealthNo ratings yet
- The Effect of Housing Tenure On Health Status of Migrant Populations in China: Are Health Service Utilization and Social Integration Mediating Factors?Document9 pagesThe Effect of Housing Tenure On Health Status of Migrant Populations in China: Are Health Service Utilization and Social Integration Mediating Factors?Ziyad NandoNo ratings yet
- First DraftDocument9 pagesFirst DraftLouisse EsteraNo ratings yet
- Week 2 Social ClassDocument2 pagesWeek 2 Social ClassSaadia AHMAD SHAHEENNo ratings yet
- AloneDocument8 pagesAloneOsiris Mark CaducoyNo ratings yet
- Determinant Factors of Life Expectancy at Birth in The European Union CountriesDocument11 pagesDeterminant Factors of Life Expectancy at Birth in The European Union CountriesYuukii ChiiNo ratings yet
- Nowatzki - Sex Is Not Enough The Need For Gender Based Analysis in Health ResearchDocument16 pagesNowatzki - Sex Is Not Enough The Need For Gender Based Analysis in Health ResearchmariaconstanzavasqueNo ratings yet
- Socio-Economic Inequalities in Health and Health Service Use Among Older Adults in India - Results From The WHO Study On Global AGEing and Adult Health SurveyDocument10 pagesSocio-Economic Inequalities in Health and Health Service Use Among Older Adults in India - Results From The WHO Study On Global AGEing and Adult Health SurveyAnindita BalaganesanNo ratings yet
- Gale Researcher Guide for: Introduction to Health, Illness, and Health CareFrom EverandGale Researcher Guide for: Introduction to Health, Illness, and Health CareNo ratings yet
- Post-Approval Safety Data Management: Definitions and Standards For Expedited Reporting ICH Harmonised Tripartite Guideline DraftDocument12 pagesPost-Approval Safety Data Management: Definitions and Standards For Expedited Reporting ICH Harmonised Tripartite Guideline DraftasdasNo ratings yet
- Presidential Decree No. 603 (Child and Youth Welfare Code)Document3 pagesPresidential Decree No. 603 (Child and Youth Welfare Code)Love Bordamonte92% (13)
- Factor V Leiden Thrombophilia Causing Recurrent ThrombosisDocument5 pagesFactor V Leiden Thrombophilia Causing Recurrent ThrombosisAtiquzzaman RinkuNo ratings yet
- Fresh Air Camp Application 2010Document13 pagesFresh Air Camp Application 2010Morgan Memorial Goodwill IndustriesNo ratings yet
- Stages of Labor & Leopold's Maneuver First Stage: Dilating StageDocument11 pagesStages of Labor & Leopold's Maneuver First Stage: Dilating StagePanJan BalNo ratings yet
- Basic In-Home Colon Cleansing - An Illustrated Guide 0962296538Document134 pagesBasic In-Home Colon Cleansing - An Illustrated Guide 0962296538autonomist100% (21)
- MsdsDocument5 pagesMsdsRizqi S RohmandaniNo ratings yet
- Natco 2016 PDFDocument101 pagesNatco 2016 PDFSagar BhardwajNo ratings yet
- Study and Managemet of Blunt Injury AbdomenDocument128 pagesStudy and Managemet of Blunt Injury Abdomendevireddy bruhathiNo ratings yet
- This Study Resource Was: On 1. Put Yourself in Hardina Smythe's Place and Systematically Evaluate The ThreeDocument1 pageThis Study Resource Was: On 1. Put Yourself in Hardina Smythe's Place and Systematically Evaluate The ThreeElad BreitnerNo ratings yet
- St. Patrick's Day Parade: Program & Line-UpDocument4 pagesSt. Patrick's Day Parade: Program & Line-UpMaple Lake MessengerNo ratings yet
- Consumer Studies Nov 2021 MG EngDocument19 pagesConsumer Studies Nov 2021 MG EngMphoentle LekabaNo ratings yet
- How Doppelgänger Brand Images Influence The Market Creation Process: Longitudinal Insights From The Rise of Botox CosmeticDocument14 pagesHow Doppelgänger Brand Images Influence The Market Creation Process: Longitudinal Insights From The Rise of Botox Cosmeticmgiesler5229100% (1)
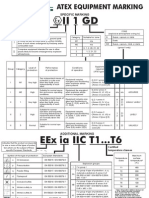
- Atex MarkingDocument1 pageAtex Markinggangotri05No ratings yet
- Reliance Health Claim FormDocument4 pagesReliance Health Claim FormarijitnirmalNo ratings yet
- Safety Norms in Construction SiteDocument13 pagesSafety Norms in Construction Sitesantoshspav100% (1)
- RIQAS ExplainedDocument36 pagesRIQAS Explainedthien pham duc100% (1)
- Implementing Guidelines For The Conduct of Classes 21 22Document7 pagesImplementing Guidelines For The Conduct of Classes 21 22Ace ClarkNo ratings yet
- Amazing Presentation Number 777Document13 pagesAmazing Presentation Number 777api-552813162No ratings yet
- PTS 60.2210 PDFDocument106 pagesPTS 60.2210 PDFpmnasimNo ratings yet
- Bioprogressive Therapy: Overbite Reduction With The Lower Utility ArchDocument4 pagesBioprogressive Therapy: Overbite Reduction With The Lower Utility ArchMeguja jithinNo ratings yet
- DNS - Sport III Part1Document6 pagesDNS - Sport III Part1jole000100% (1)
- Fill in The Blanks With A Suitable Contrast Connector (WhereasDocument2 pagesFill in The Blanks With A Suitable Contrast Connector (WhereasGLENN SUAREZNo ratings yet
- Essay Writing Vocabulary IndexDocument15 pagesEssay Writing Vocabulary IndexMithun RajNo ratings yet
- Booklet On Technology Options DewatsDocument52 pagesBooklet On Technology Options DewatsAl Patrick Dela CalzadaNo ratings yet
- Proposal For Construction of A Central Medical StoreDocument14 pagesProposal For Construction of A Central Medical StoreSele KondoNo ratings yet
- Severe Vata DisordersDocument3 pagesSevere Vata DisordersAkhila VijayakumarNo ratings yet
- Semi-Solid Applications 101Document1 pageSemi-Solid Applications 101CHARLES RONALD GENATONo ratings yet
- FSBGD Written Study Questions 2003Document201 pagesFSBGD Written Study Questions 2003velangniNo ratings yet
- Vibrio & Aeromonas & PlesiomonasDocument48 pagesVibrio & Aeromonas & PlesiomonasOscar PeñaNo ratings yet