You might also like
- Conditions of Reporting TermsDocument1 pageConditions of Reporting TermsPlatoNo ratings yet
- Evidencia de InglesDocument6 pagesEvidencia de InglesLaura Ximena BarraganNo ratings yet
- History of Perodua analysisDocument13 pagesHistory of Perodua analysisaishahrodziNo ratings yet
- Castillo ProfileDocument46 pagesCastillo ProfileprabhumanocNo ratings yet
- 1 s2.0 S0167931722002295 MainDocument14 pages1 s2.0 S0167931722002295 Mainaaron wileyNo ratings yet
- Shivani OfferDocument13 pagesShivani OfferVipul TyagiNo ratings yet
- NU711351053737252 EticketDocument2 pagesNU711351053737252 EticketFried RiceNo ratings yet
- GI20211107671Document6 pagesGI20211107671Rajubhai JasoliyaNo ratings yet
- Lubrex Product Catalog 2021Document73 pagesLubrex Product Catalog 2021Mohammed BabatinNo ratings yet
- 5 - Give It Up Social Marketing - 2022 PDFDocument22 pages5 - Give It Up Social Marketing - 2022 PDFSimran AgrawalNo ratings yet
- Final Kyc Form Epmuy 3Document2 pagesFinal Kyc Form Epmuy 3P RUDRA PRASANNANo ratings yet
- Boarding PassDocument3 pagesBoarding PassSusilNo ratings yet
- DEKA Russell Instruction ManualDocument13 pagesDEKA Russell Instruction ManualSafwan MohamadNo ratings yet
- Cash-In Cash-Out Cross-Country Analysis: Kenya: December 2020Document10 pagesCash-In Cash-Out Cross-Country Analysis: Kenya: December 2020Tsila SimpleNo ratings yet
- Macheli S2 ArchDocument4 pagesMacheli S2 ArchPhakiso MolelekiNo ratings yet
- NGIG Study Book Element 1 151122Document70 pagesNGIG Study Book Element 1 151122haroonraja579No ratings yet
- 2 CSC v. CortesDocument2 pages2 CSC v. CortesRexenne MarianoNo ratings yet
- Wallstreetjournal 20170218 The Wall Street JournalDocument50 pagesWallstreetjournal 20170218 The Wall Street Journalstefano100% (1)
- Session 1Document10 pagesSession 1Shams TabrezNo ratings yet
- Optimization of Wind Farm Yaw Offset Angle Using Online Genetic Algorithm With A Modified Elitism Strategy To Maximize Power ProductionDocument15 pagesOptimization of Wind Farm Yaw Offset Angle Using Online Genetic Algorithm With A Modified Elitism Strategy To Maximize Power ProductionKurniawan CorpNo ratings yet
- 865G&GV&PE7MF EN Manual V1.0 0404Document70 pages865G&GV&PE7MF EN Manual V1.0 0404David Alexander Ortiz RodriguezNo ratings yet
- Technological and Biological Properties of ButtermDocument10 pagesTechnological and Biological Properties of ButtermSaniaNo ratings yet
- Aplication For GEN & SPL RECRUITMENT 2022 - 23 1Document4 pagesAplication For GEN & SPL RECRUITMENT 2022 - 23 1Gautam KumarNo ratings yet
- ZE500KL RF Hardware Trouble Shooting GuideDocument59 pagesZE500KL RF Hardware Trouble Shooting GuideWilliam SequeraNo ratings yet
- Free Gprs Settings For Idea..Document28 pagesFree Gprs Settings For Idea..aghakhan1988No ratings yet
- 7805 Circuit AnalysisDocument25 pages7805 Circuit Analysisgrb2m2z92No ratings yet
- Uwa Mba BrochureDocument32 pagesUwa Mba BrochureSrihariRaoNo ratings yet
- Madhavi Bhatt-1 PDFDocument2 pagesMadhavi Bhatt-1 PDFMadhavi BhattNo ratings yet
- CT071-3-3-DDAC-Class Test Paper #2-AnswerDocument12 pagesCT071-3-3-DDAC-Class Test Paper #2-AnswerPurnima OliNo ratings yet
- Iso 27001 FBR ChecklistDocument9 pagesIso 27001 FBR Checklistk200341No ratings yet
- FRONX BrochureDocument16 pagesFRONX BrochureMK AutoNo ratings yet
- AdministrationGuide PDFDocument316 pagesAdministrationGuide PDFPercy SolizNo ratings yet
- Global Baby Cereals Market, 2009-2015Document3 pagesGlobal Baby Cereals Market, 2009-2015Axis Research MindNo ratings yet
- CS Form 100 - Revised September 2016Document2 pagesCS Form 100 - Revised September 2016MaximalistaNo ratings yet
- The Second Mile Annual Report 2010Document12 pagesThe Second Mile Annual Report 2010mosesloaf8619No ratings yet
- AA-7000 Series: Shimadzu Atomic Absorption SpectrophotometersDocument28 pagesAA-7000 Series: Shimadzu Atomic Absorption Spectrophotometersosklav100% (1)
- 5 PDFDocument4 pages5 PDFDrNiladri RoyNo ratings yet
- FASH181 Answer 5Document4 pagesFASH181 Answer 5Go CheckNo ratings yet
- MHIEC Ash Extractor Specification ReviewDocument109 pagesMHIEC Ash Extractor Specification ReviewNguyễn Linh100% (1)
- Formato Irrevocable Master FeeDocument6 pagesFormato Irrevocable Master FeeNelson GavilanesNo ratings yet
- U.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993Document7 pagesU.S. Food & Drug Administration 10903 New Hampshire Avenue: Silver Spring, MD 20993api-237132031No ratings yet
- Akkaya Katalog EN 2019Document66 pagesAkkaya Katalog EN 2019Juan MendozaNo ratings yet
- Loan Term Sheet - 20 - 12 - 42Document21 pagesLoan Term Sheet - 20 - 12 - 42Md riyaj ali KhanNo ratings yet
- Mint Delhi 28-10-2022Document20 pagesMint Delhi 28-10-2022sushilpal161No ratings yet
- Fixed-Rate Loans Up To $100k: Baisakh 2080 Apr/May 2023Document3 pagesFixed-Rate Loans Up To $100k: Baisakh 2080 Apr/May 2023Building SolutionNo ratings yet
- Sparc t5-4 ManualDocument212 pagesSparc t5-4 ManualStevan NikolicNo ratings yet
- Alfursan Membership Guide - EnglishDocument28 pagesAlfursan Membership Guide - EnglishPramod Govind SalunkheNo ratings yet
- Grain and Feed Annual - Dhaka - Bangladesh - 03-27-2021 PDFDocument28 pagesGrain and Feed Annual - Dhaka - Bangladesh - 03-27-2021 PDFDr. Suman PaulNo ratings yet
- KALRE ESE Lightning Protection System CatalogDocument20 pagesKALRE ESE Lightning Protection System CatalogEd Macusi AsuncionNo ratings yet
- Rajkot To Mahesana ST BUS TIME TABLEDocument2 pagesRajkot To Mahesana ST BUS TIME TABLERahul PatelNo ratings yet
- Manual Firmware de Hikvision PDFDocument9 pagesManual Firmware de Hikvision PDFjlherreratNo ratings yet
- Change in Broker CAMSDocument2 pagesChange in Broker CAMSpooja katariyaNo ratings yet
- Samsung Tv8Document65 pagesSamsung Tv8Enrile Labiano BaduaNo ratings yet
- GeM Bidding 4427054Document7 pagesGeM Bidding 4427054santaji dhanwadeNo ratings yet
- BOKARO, JHARKHAND-829132: English Project WorkDocument32 pagesBOKARO, JHARKHAND-829132: English Project WorkTanishq AryanNo ratings yet
- Og 22 9906 1801 00068245Document7 pagesOg 22 9906 1801 00068245RAJALINGAM SNo ratings yet
- American Innovation and Choice Online ActDocument22 pagesAmerican Innovation and Choice Online ActAlex KantrowitzNo ratings yet
- Ethnicity and Sexuality - NagelDocument28 pagesEthnicity and Sexuality - NagelFernando UrreaNo ratings yet
- Data Kontrak PKM TepselDocument18 pagesData Kontrak PKM Tepselria mustikaNo ratings yet
- Reliance Health Claim FormDocument4 pagesReliance Health Claim FormSumit BhallaNo ratings yet
- Summary of Rajiv Dixit's Lectures On Ayurveda BasedDocument11 pagesSummary of Rajiv Dixit's Lectures On Ayurveda Basedarijitnirmal100% (1)
- Quadratic 1Document2 pagesQuadratic 1arijitnirmalNo ratings yet
- Water Reflection PhotoshopDocument1 pageWater Reflection PhotoshoparijitnirmalNo ratings yet
- Owners Manual LG SIGNAGE ENGDocument32 pagesOwners Manual LG SIGNAGE ENGarijitnirmalNo ratings yet
- Edu Code 25 04 13Document505 pagesEdu Code 25 04 13arijitnirmalNo ratings yet
- Some Terms About FailDocument1 pageSome Terms About FailarijitnirmalNo ratings yet
- Start Stop TNSListner in OracleDocument2 pagesStart Stop TNSListner in OraclearijitnirmalNo ratings yet
- Enterprise Java BeansDocument7 pagesEnterprise Java BeansarijitnirmalNo ratings yet
- Advanced RenamerDocument2 pagesAdvanced RenamerarijitnirmalNo ratings yet
- Mca Assignment 2013 14 - IV SemDocument17 pagesMca Assignment 2013 14 - IV SemarijitnirmalNo ratings yet
- Start Stop TNSListner in OracleDocument2 pagesStart Stop TNSListner in OraclearijitnirmalNo ratings yet
- MP, Bca, Mca & Soet - 1Document3 pagesMP, Bca, Mca & Soet - 1arijitnirmalNo ratings yet
- Application Form For Re-Evaluation of Answer ScriptsDocument3 pagesApplication Form For Re-Evaluation of Answer ScriptsarijitnirmalNo ratings yet
- Photoshop CS6Document1 pagePhotoshop CS6arijitnirmalNo ratings yet
- A Software System Development Life Cycle Model For ImprovedDocument22 pagesA Software System Development Life Cycle Model For ImprovedPutri KrismayanthiNo ratings yet
- Systems Development Life Cycle: Objectives and Requirements - Bender RBT Inc.Document60 pagesSystems Development Life Cycle: Objectives and Requirements - Bender RBT Inc.ybert@verizon.net100% (6)
- Emergency Numbers - Surat Municipal CorporationDocument1 pageEmergency Numbers - Surat Municipal CorporationarijitnirmalNo ratings yet
- Graphs DeterminationDocument4 pagesGraphs DeterminationarijitnirmalNo ratings yet
- Structuring Database For Accounting: 504 AccountancyDocument50 pagesStructuring Database For Accounting: 504 AccountancyrajsalgyanNo ratings yet
- MCA TimeDocument2 pagesMCA TimearijitnirmalNo ratings yet
- Where To Contact For WhatDocument3 pagesWhere To Contact For WhatarijitnirmalNo ratings yet
- Topological Sort Algorithm (TSADocument9 pagesTopological Sort Algorithm (TSAarijitnirmalNo ratings yet
- SeDocument5 pagesSearijitnirmalNo ratings yet
- IGNOU MCA MCS-33 Solved Assignment 2011Document5 pagesIGNOU MCA MCS-33 Solved Assignment 2011arijitnirmalNo ratings yet
- The AVL Tree Rotations Tutorial: by John Hargrove Version 1.0.1, Updated Mar-22-2007Document7 pagesThe AVL Tree Rotations Tutorial: by John Hargrove Version 1.0.1, Updated Mar-22-2007arijitnirmalNo ratings yet
- Where To Contact For WhatDocument3 pagesWhere To Contact For WhatarijitnirmalNo ratings yet
- Merry ChristmasDocument1 pageMerry ChristmasarijitnirmalNo ratings yet
- CCE Certificate-2009-11-A3 Size (Coloured) - 13-10-2010Document4 pagesCCE Certificate-2009-11-A3 Size (Coloured) - 13-10-2010Deepika KhoslaNo ratings yet
- 2sem Assig 11 New SyllabusDocument14 pages2sem Assig 11 New Syllabusmandrake2k79213No ratings yet
- Istoric Cont: Criterii de CautareDocument4 pagesIstoric Cont: Criterii de CautareRyō Sumy0% (1)
- Statement of Account: Hifadhi Current Account (CDI) 0100511846350 (KES)Document2 pagesStatement of Account: Hifadhi Current Account (CDI) 0100511846350 (KES)AdiEzz100% (1)
- Final Project Icici SegmentDocument38 pagesFinal Project Icici SegmentNitinAgnihotriNo ratings yet
- International Economics 15th Edition Robert Carbaugh Test BankDocument26 pagesInternational Economics 15th Edition Robert Carbaugh Test BankCassandraHarrisyanb100% (62)
- 50100500407621_1711954613447Document11 pages50100500407621_1711954613447iblfinserv0No ratings yet
- CN Unit 1Document81 pagesCN Unit 1Hitesh PatelNo ratings yet
- Analiz Sovremenn H Metodov I Sredstv Pov Sheniya Spektralnoy Effektivnosti Sistem SvyaziDocument19 pagesAnaliz Sovremenn H Metodov I Sredstv Pov Sheniya Spektralnoy Effektivnosti Sistem SvyaziAn TASNo ratings yet
- XINGUODU - NEXGO Company Profile 2022Document25 pagesXINGUODU - NEXGO Company Profile 2022Ibnu SaefullahNo ratings yet
- RC - DS - ISCOM HT803G Series Bridge ONT (Rel - 02)Document3 pagesRC - DS - ISCOM HT803G Series Bridge ONT (Rel - 02)Георги ПоповNo ratings yet
- EXERCISE 1.2 ACCOUNTING CYCLE (No.2) FABM2Document3 pagesEXERCISE 1.2 ACCOUNTING CYCLE (No.2) FABM2Abijane Ilagan DarucaNo ratings yet
- Walmart Case StudyDocument11 pagesWalmart Case StudyBb DianaNo ratings yet
- Urban Transportation Planning MCQsDocument8 pagesUrban Transportation Planning MCQsWacky Amora ValenciaNo ratings yet
- ERGO PolicyDocument2 pagesERGO Policyranju93No ratings yet
- Arens Aas17 PPT 01 PDFDocument38 pagesArens Aas17 PPT 01 PDFSin TungNo ratings yet
- Cryptography and Network Security Principles and Practice. First EditionDocument64 pagesCryptography and Network Security Principles and Practice. First EditionMd asmat Ali55No ratings yet
- Aiesec - International Sos Sign Up GuideDocument28 pagesAiesec - International Sos Sign Up Guideapi-268699635No ratings yet
- BRC Global Standard For Agents and Brokers: Order FormDocument6 pagesBRC Global Standard For Agents and Brokers: Order Formavinashn1984No ratings yet
- Free Online Invitations, Premium Cards and Party Ideas EviteDocument1 pageFree Online Invitations, Premium Cards and Party Ideas EviteMaria Luisa CalderonNo ratings yet
- For The Bank Accounts of Private IndividualsDocument19 pagesFor The Bank Accounts of Private IndividualsMun MunNo ratings yet
- Annual Report 2022 en Final WebsiteDocument76 pagesAnnual Report 2022 en Final WebsiteSin SeutNo ratings yet
- Flow Chart of Import CycleDocument6 pagesFlow Chart of Import CycleAyyanar100% (1)
- Hartbeeps Northwood + Chorleywood New TermDocument2 pagesHartbeeps Northwood + Chorleywood New TermRuth ColinNo ratings yet
- Literature Review On Wireless LanDocument4 pagesLiterature Review On Wireless Lanea8r2tyk100% (1)
- Credit Reports and Scores Note Taking Guide 2 6 1 l1Document4 pagesCredit Reports and Scores Note Taking Guide 2 6 1 l1api-26781587250% (2)
- Chap 12Document23 pagesChap 12MichelleLeeNo ratings yet
- Financial Accounting: 16Th EditionDocument31 pagesFinancial Accounting: 16Th EditionZooni FatimaNo ratings yet
- CIPS L2M5 exam questions on inventory, logistics and expeditingDocument5 pagesCIPS L2M5 exam questions on inventory, logistics and expeditingEng. Abdulaziz A. Al-Massabi100% (1)
- Marketing & Distribution Strategy of HCL Info SystemDocument78 pagesMarketing & Distribution Strategy of HCL Info SystemUmesh TyagiNo ratings yet
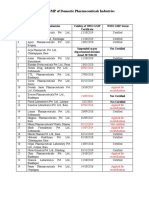
- Status of Nepali Pharma GMP CertificationDocument2 pagesStatus of Nepali Pharma GMP CertificationDapper Yourself100% (1)
- Haryana-Gurugram-Sec 50 #BA/AFSG/513: Invoice Number Billed ForDocument1 pageHaryana-Gurugram-Sec 50 #BA/AFSG/513: Invoice Number Billed ForSatender KumarNo ratings yet