You might also like
- Marquez - Case Study 4Document4 pagesMarquez - Case Study 4Caren MarquezNo ratings yet
- Marquez - Case Study 3Document6 pagesMarquez - Case Study 3Caren MarquezNo ratings yet
- Marquez - Case Study 122Document5 pagesMarquez - Case Study 122Caren MarquezNo ratings yet
- Module 1 ExamDocument109 pagesModule 1 Examnursehelp12100% (2)
- Marquez - Case Study 120Document4 pagesMarquez - Case Study 120Caren Marquez100% (1)
- HD715 90003Document45 pagesHD715 90003onur tezmanNo ratings yet
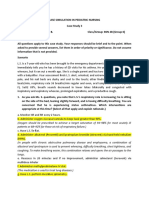
- Case Simulation 3 in Pediatric NursingDocument3 pagesCase Simulation 3 in Pediatric NursingCaren MarquezNo ratings yet
- Rufaida College of Nursing Jamia Hamdard (Hamdard University) Lesson Plan ONDocument16 pagesRufaida College of Nursing Jamia Hamdard (Hamdard University) Lesson Plan ONRaja100% (2)
- Mother's Class BFDocument55 pagesMother's Class BFriz04_fortitudessa5178100% (1)
- Case Simulation in Pediatric Nursing Case Study 1Document4 pagesCase Simulation in Pediatric Nursing Case Study 1Cheska PalomaNo ratings yet
- Case Study Baby HDocument6 pagesCase Study Baby HSharon Williams0% (1)
- Case Study 116Document4 pagesCase Study 116Jonah MaasinNo ratings yet
- PNC - Usaid 2-34 PDFDocument34 pagesPNC - Usaid 2-34 PDFRestiNo ratings yet
- NCM 107 Postpartum Care Guide QuestionDocument6 pagesNCM 107 Postpartum Care Guide QuestionMiguel LigasNo ratings yet
- Enbc RaniDocument24 pagesEnbc RaniRajaNo ratings yet
- Unciano Colleges Inc. Sta. Mesa ManilaDocument14 pagesUnciano Colleges Inc. Sta. Mesa Manilanaman24No ratings yet
- 3 - Aasisting With FeedingDocument23 pages3 - Aasisting With Feeding.No ratings yet
- Infant Feeding Breastfeeding The Healthy Term Baby - 110219 PDFDocument10 pagesInfant Feeding Breastfeeding The Healthy Term Baby - 110219 PDFFKIANo ratings yet
- BHW TRAINING Newborn HealthDocument24 pagesBHW TRAINING Newborn HealthWilma BeraldeNo ratings yet
- Kangaroo Mother Care Rooming in UpdatedDocument44 pagesKangaroo Mother Care Rooming in UpdatedStar DustNo ratings yet
- Case Study 107 2 Manalo Clio Anne P. 2BDocument4 pagesCase Study 107 2 Manalo Clio Anne P. 2BDudong SasakiNo ratings yet
- Case Study On Observation and Newborn CareDocument8 pagesCase Study On Observation and Newborn CarePiyush Dutta100% (1)
- Teaching Plan Fo Cord Car1Document15 pagesTeaching Plan Fo Cord Car1jaden1233No ratings yet
- Intervention 2: Essential Newborn Care Essential Newborn (Including Chlorhexidine For Umbilical Cord Care) Essential Newborn CareDocument5 pagesIntervention 2: Essential Newborn Care Essential Newborn (Including Chlorhexidine For Umbilical Cord Care) Essential Newborn CareSheima Ainie JuripaeNo ratings yet
- Delivery Room: (Institution/ Area)Document8 pagesDelivery Room: (Institution/ Area)Nickaela CalalangNo ratings yet
- Teaching Plan MNSG Breast FeedingDocument6 pagesTeaching Plan MNSG Breast FeedingKevin VinzNo ratings yet
- Case PresentationDocument24 pagesCase PresentationDarlen RabanoNo ratings yet
- Case Study On Observation and Newborn CareDocument38 pagesCase Study On Observation and Newborn CarePiyush Dutta100% (2)
- Neonatal NursingDocument53 pagesNeonatal Nursingkrishnasree100% (1)
- General Objecti-Wps OfficeDocument3 pagesGeneral Objecti-Wps OfficeSumit YadavNo ratings yet
- Breastfeeding Dissertation TopicsDocument8 pagesBreastfeeding Dissertation TopicsBuyACollegePaperOnlineMilwaukee100% (1)
- M NewbornDocument13 pagesM NewbornDonaJeanNo ratings yet
- Delivery Room,.Document3 pagesDelivery Room,.Yukki CuartoNo ratings yet
- Newborn Care Case PresDocument11 pagesNewborn Care Case PresCamille GalasNo ratings yet
- LP 1 I NCM 107 RLE I CARE OF PREGNANT WOMAN StudentsDocument28 pagesLP 1 I NCM 107 RLE I CARE OF PREGNANT WOMAN StudentsNaomi Anne AsuntoNo ratings yet
- NCPDocument4 pagesNCPMarielle SorianoNo ratings yet
- Wellness of A New Born: CHO Mentoring ProjectDocument57 pagesWellness of A New Born: CHO Mentoring ProjectAmelia ChristmasNo ratings yet
- Reproductive Nursing System: Neonatus (In 6 Hours, 6 Hour) Nursing Care Plan + WOC (Pathophysiology + Nursing Problem)Document11 pagesReproductive Nursing System: Neonatus (In 6 Hours, 6 Hour) Nursing Care Plan + WOC (Pathophysiology + Nursing Problem)Nofri YanTiNo ratings yet
- Assess The Knowledge Attitude and Practice Regarding Breastfeeding Among Primi MothersDocument43 pagesAssess The Knowledge Attitude and Practice Regarding Breastfeeding Among Primi Mothersjuli_naz94% (33)
- MODULE 4 1st Part INTRAPARTAL CARE - Docx 2Document13 pagesMODULE 4 1st Part INTRAPARTAL CARE - Docx 2jared abriolNo ratings yet
- Teaching Plan Breast Feeding 270Document8 pagesTeaching Plan Breast Feeding 270Franco ObedozaNo ratings yet
- Nicu Case StudyDocument4 pagesNicu Case Studyapi-508102663No ratings yet
- Brief Resume of The Intended Work: "The Nation Walks On The Feet of Little Children."Document11 pagesBrief Resume of The Intended Work: "The Nation Walks On The Feet of Little Children."sr.kumariNo ratings yet
- Maternal and Child Health Programmes AssignmentDocument11 pagesMaternal and Child Health Programmes Assignmentannu panchal80% (5)
- Baby Friendly Hospital InitiativeDocument6 pagesBaby Friendly Hospital InitiativeBinal JoshiNo ratings yet
- Care of NewornDocument4 pagesCare of NewornArchana SahuNo ratings yet
- UntitledDocument18 pagesUntitledstuffednurseNo ratings yet
- Mother's Class BFDocument55 pagesMother's Class BFriz04_fortitudessa5178No ratings yet
- Discharge For InfantDocument3 pagesDischarge For InfantIra Krystel ReyesNo ratings yet
- Foundations of NursingDocument14 pagesFoundations of NursingDeborah Chimeremeze JosephNo ratings yet
- My ThesisDocument46 pagesMy ThesisManish SharmaNo ratings yet
- Einc-Word 054847Document4 pagesEinc-Word 054847Jane OrsalNo ratings yet
- DR ChecklistDocument2 pagesDR ChecklistShinrin SukehiroNo ratings yet
- 05 N310 16324Document14 pages05 N310 16324Wanda WoodNo ratings yet
- Management of Breast FeedingDocument17 pagesManagement of Breast FeedingUday KumarNo ratings yet
- Iwas Paputok LectureDocument31 pagesIwas Paputok LectureShan Dave TupasNo ratings yet
- Essential Intrapartum and Newborn CareDocument5 pagesEssential Intrapartum and Newborn Careanjie kamidNo ratings yet
- Rle NCM 107 Case Simulation 116 No AnswerDocument19 pagesRle NCM 107 Case Simulation 116 No AnswerDudong SasakiNo ratings yet
- Post Partum PeriodDocument31 pagesPost Partum PeriodMay CaballeroNo ratings yet
- First-Time Mom Handbook: All the Steps from Being Pregnant, Getting Ready and Embracing Motherhood: Motherhood & ChildbirthFrom EverandFirst-Time Mom Handbook: All the Steps from Being Pregnant, Getting Ready and Embracing Motherhood: Motherhood & ChildbirthNo ratings yet
- "Nurturing Beginnings: A Comprehensive Guide to Breastfeeding Success"From Everand"Nurturing Beginnings: A Comprehensive Guide to Breastfeeding Success"No ratings yet
- Nursing Diagnosis Objectives Nursing Interventions Rationale Risk For InjuryDocument1 pageNursing Diagnosis Objectives Nursing Interventions Rationale Risk For InjuryCaren MarquezNo ratings yet
- Marquez - Case Study 114Document6 pagesMarquez - Case Study 114Caren MarquezNo ratings yet
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- Case Study 2Document12 pagesCase Study 2Caren MarquezNo ratings yet
- Filling Station GuidelinesDocument8 pagesFilling Station GuidelinesOladipupo Mayowa PaulNo ratings yet
- Ky Nang Tong Hop 1Document2 pagesKy Nang Tong Hop 1Hong Ho100% (1)
- Separate Thin Amplifier Type: AP-V40AW SeriesDocument12 pagesSeparate Thin Amplifier Type: AP-V40AW SeriesRafael MirandaNo ratings yet
- The 0-1 Knapsack Problem: An Introductory SurveyDocument13 pagesThe 0-1 Knapsack Problem: An Introductory SurveyRahma JabriNo ratings yet
- Low Noise Operational Amplifiers: DatasheetDocument43 pagesLow Noise Operational Amplifiers: DatasheetMisael GonzalezNo ratings yet
- Chemistry 1Document19 pagesChemistry 1SAHIL SINGHNo ratings yet
- Exercise Weight Reps Completed Reps Sets: Week 1 Day 1 171.5lbsDocument35 pagesExercise Weight Reps Completed Reps Sets: Week 1 Day 1 171.5lbshuhah303No ratings yet
- Density Worksheet Physics Class 9Document3 pagesDensity Worksheet Physics Class 9vectors academyNo ratings yet
- The Limits of Thermal Comfort: Avoiding Overheating in European BuildingsDocument3 pagesThe Limits of Thermal Comfort: Avoiding Overheating in European BuildingsElissaNo ratings yet
- European Commission: 2slqlrqriwkh 6Flhqwlilf&Rpplwwhhrq9Hwhulqdu/0Hdvxuhvuhodwlqjwr3Xeolf+Hdowk RQDocument64 pagesEuropean Commission: 2slqlrqriwkh 6Flhqwlilf&Rpplwwhhrq9Hwhulqdu/0Hdvxuhvuhodwlqjwr3Xeolf+Hdowk RQkhoi moleNo ratings yet
- Microstrip AntennaDocument56 pagesMicrostrip AntennaPrajakta MoreNo ratings yet
- Circles Ad Infinitum - Nrich - MathsDocument1 pageCircles Ad Infinitum - Nrich - MathsgonsalvisNo ratings yet
- Dispassion (Vairagya)Document3 pagesDispassion (Vairagya)1stSargezNo ratings yet
- Basics - OpenEnergyMonitor 0.0.1 DocumentationDocument5 pagesBasics - OpenEnergyMonitor 0.0.1 Documentationh2oo2hNo ratings yet
- (6 Files Merged)Document6 pages(6 Files Merged)Jug SinghNo ratings yet
- GPS Map Camera Lite For Photo Location and TimestampDocument4 pagesGPS Map Camera Lite For Photo Location and Timestampgpslite cameraNo ratings yet
- Corona PDFDocument51 pagesCorona PDFAri CaushiNo ratings yet
- Slip FormsDocument31 pagesSlip Formssabareesan09No ratings yet
- PowerRelays Selection GuideDocument24 pagesPowerRelays Selection GuidearturobatallasNo ratings yet
- Recommended Price List (RPL) RPL RS.: RheinlandDocument16 pagesRecommended Price List (RPL) RPL RS.: RheinlandHemant Panpaliya100% (2)
- Nature of Educational PsychologyDocument44 pagesNature of Educational Psychologypintupal2008100% (8)
- Criteria For Patient Transfer From Recovery AreaDocument2 pagesCriteria For Patient Transfer From Recovery AreaDr Jisha TuNo ratings yet
- Air To Water Catalog Standard 20220419Document34 pagesAir To Water Catalog Standard 20220419coin pvhNo ratings yet
- Pergole SUNTECH PRIVEEDocument125 pagesPergole SUNTECH PRIVEEAlejandro MorelNo ratings yet
- Economic Botany PresentationDocument16 pagesEconomic Botany Presentationjames allenNo ratings yet
- 4.2 Environmental Policy: EMS Implementation ChecklistDocument8 pages4.2 Environmental Policy: EMS Implementation Checklistrnp2007123No ratings yet
- 2012 03 Particle Sizing Comminution PDFDocument6 pages2012 03 Particle Sizing Comminution PDFYashwanth KumarNo ratings yet
- Voice RecognitionDocument18 pagesVoice Recognitionr100% (1)
- Guideline For Prevention and Safe Handling of HydratesDocument11 pagesGuideline For Prevention and Safe Handling of Hydrateshitm357No ratings yet