You might also like
- Freebie Bundle-50 PagesDocument75 pagesFreebie Bundle-50 PagesKarla Seravalli83% (6)
- ACS/ASE Medical Student Core Curriculum Trauma II: Diagnosis and ManagementDocument35 pagesACS/ASE Medical Student Core Curriculum Trauma II: Diagnosis and ManagementJefriantoNo ratings yet
- Postpartum Complications 2015Document52 pagesPostpartum Complications 2015Janella Asis100% (1)
- IMCI BayaniDocument6 pagesIMCI BayaniclarNo ratings yet
- Management of The Sick Young Infant Age 1 Week Up To 2 MonthsDocument5 pagesManagement of The Sick Young Infant Age 1 Week Up To 2 Monthsapi-19824701No ratings yet
- IMCI Session 7 - Sick Young InfantDocument69 pagesIMCI Session 7 - Sick Young Infantsarguss14100% (2)
- IMCIDocument2 pagesIMCIJarzhieRhojeenNo ratings yet
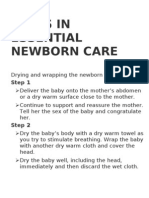
- Steps in Essential Newborn CareDocument12 pagesSteps in Essential Newborn CareCedy L. CieloNo ratings yet
- Nursing Care of Clients With General Disturbance in Reproduction and SexualityDocument23 pagesNursing Care of Clients With General Disturbance in Reproduction and Sexualityastraeax pandaNo ratings yet
- Mumps: Dr. Oky Rahma Prihandani, Msi - Med, Spa Fakultas Kedokteran Universitas Muhammadiyah SemarangDocument12 pagesMumps: Dr. Oky Rahma Prihandani, Msi - Med, Spa Fakultas Kedokteran Universitas Muhammadiyah Semarangnur chasanahNo ratings yet
- Case Report "Febrile Seizures": Betsheba E. S. 123307018Document37 pagesCase Report "Febrile Seizures": Betsheba E. S. 123307018AmandaRizkaNo ratings yet
- 4 - ToddlerDocument25 pages4 - ToddlerMichelle FactoNo ratings yet
- Nursing Care of at Risk/ High Risk/ Sick ClientDocument256 pagesNursing Care of at Risk/ High Risk/ Sick ClientAaron ConstantinoNo ratings yet
- Rationale For An Integrated Approach in The Management of Sick ChildrenDocument42 pagesRationale For An Integrated Approach in The Management of Sick ChildrenRIK HAROLD GATPANDANNo ratings yet
- Test Scribd 3Document42 pagesTest Scribd 3Kiran KumarNo ratings yet
- MMDSTDocument1 pageMMDSTJaic Ealston D. TampusNo ratings yet
- Cleansing Bed BathDocument16 pagesCleansing Bed BathRoger ViloNo ratings yet
- Neonatal Sepsis: CausesDocument3 pagesNeonatal Sepsis: CausesGeraldine BirowaNo ratings yet
- FINAL ENC ChecklistDocument8 pagesFINAL ENC ChecklistRaven Torres100% (1)
- Randomized Trial of Plastic Bags To Prevent TermDocument8 pagesRandomized Trial of Plastic Bags To Prevent TermkemalmiaNo ratings yet
- NCM 107: Care of The Mother and Child (WELL) : San Pablo Colleges College of Nursing San Pablo City, LagunaDocument20 pagesNCM 107: Care of The Mother and Child (WELL) : San Pablo Colleges College of Nursing San Pablo City, LagunaLorraine CayamandaNo ratings yet
- Mumps PresentationDocument15 pagesMumps PresentationMoney MotivationNo ratings yet
- Applying Pediatric Restrains Final Group 1bDocument6 pagesApplying Pediatric Restrains Final Group 1bJimnah Rhodrick Bontilao0% (1)
- The Newborn (Neonate) : The Unang Yakap Strategy: Essential Intrapartal Newborn Care (Einc)Document4 pagesThe Newborn (Neonate) : The Unang Yakap Strategy: Essential Intrapartal Newborn Care (Einc)ROSANNA BUCAGNo ratings yet
- Pedia Set B PRNDocument9 pagesPedia Set B PRNEdgar RebuyasNo ratings yet
- What Is The Apgar ScoreDocument4 pagesWhat Is The Apgar ScoreAira Jane MuñozNo ratings yet
- Notes On Baby Bath - Care of The Mother During The Postpartum PeriodDocument12 pagesNotes On Baby Bath - Care of The Mother During The Postpartum PeriodOink TopusNo ratings yet
- NUrsing Care PreschoolerDocument15 pagesNUrsing Care PreschoolerShamie ColozaNo ratings yet
- Signs and Symptoms of DiseaseDocument3 pagesSigns and Symptoms of DiseaseAdrian MangahasNo ratings yet
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaNo ratings yet
- Module 1 NCM 107 Pedia G & DDocument18 pagesModule 1 NCM 107 Pedia G & DAshley Nicole Bulawan BalladNo ratings yet
- PEDIA Lecture NCMA 219Document9 pagesPEDIA Lecture NCMA 219Yayin PestañoNo ratings yet
- PnemoniaDocument38 pagesPnemoniaArjumand AliNo ratings yet
- Newborn Assessment, Apgar & Ballard Scoring NotesDocument3 pagesNewborn Assessment, Apgar & Ballard Scoring NotesAshitakaNo ratings yet
- Child Health Nursing: MumpsDocument25 pagesChild Health Nursing: MumpsmanibharathiNo ratings yet
- Newborn Care Checklist EditedDocument3 pagesNewborn Care Checklist EditedMa. Danessa Lei AlavataNo ratings yet
- Role of Child Health NurseDocument40 pagesRole of Child Health NurseBinal Joshi100% (1)
- Midwifery Skills Clinical Laboratory: The Midwives ProcessDocument26 pagesMidwifery Skills Clinical Laboratory: The Midwives ProcessNano KaNo ratings yet
- Alteration in Inflammatory and Immunologic ResponseDocument1 pageAlteration in Inflammatory and Immunologic Responseleofrancis1984No ratings yet
- Immediate Newborn CareDocument21 pagesImmediate Newborn CareScarlet AmodiaNo ratings yet
- Ballard Gestational Age AssessmentDocument8 pagesBallard Gestational Age AssessmentgailNo ratings yet
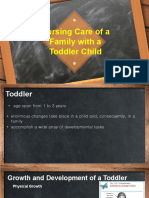
- Nursing Care of A Family With A ToddlerDocument37 pagesNursing Care of A Family With A ToddlerKarly Alissa TarubalNo ratings yet
- Nursing Care For NewbornDocument33 pagesNursing Care For NewbornDarla Quiballo100% (1)
- Health Problems Common in PRESCHOOLDocument15 pagesHealth Problems Common in PRESCHOOLJanelle Lois EscolanoNo ratings yet
- College of Allied Health Studies: NCM 102-Health Education Quiz 2Document1 pageCollege of Allied Health Studies: NCM 102-Health Education Quiz 2Mikel TuyayNo ratings yet
- 3 - High Risk InfantDocument30 pages3 - High Risk InfantMohammed AtaNo ratings yet
- Mcn. ReviewerDocument18 pagesMcn. ReviewerjeyNo ratings yet
- Growth and Development of Newborn To InfancyDocument54 pagesGrowth and Development of Newborn To Infancymerin sunilNo ratings yet
- BSN 2 Case Study On Family Nursing ProcessDocument13 pagesBSN 2 Case Study On Family Nursing ProcessRainier IbarretaNo ratings yet
- Intrapartum: Delivery Room Technique PurposeDocument8 pagesIntrapartum: Delivery Room Technique PurposeRoshin TejeroNo ratings yet
- MCN 4th QuizDocument27 pagesMCN 4th Quizastraeax pandaNo ratings yet
- Meal Planning For ChildrenDocument2 pagesMeal Planning For ChildrenSheryl Anne GonzagaNo ratings yet
- MCN SF Chapter 18 QuizDocument4 pagesMCN SF Chapter 18 QuizKathleen AngNo ratings yet
- 60 Steps Normal DeliveryDocument6 pages60 Steps Normal DeliveryDrBoen BunawanNo ratings yet
- Breastfeeding and HivDocument30 pagesBreastfeeding and HivbxrbxrNo ratings yet
- EENC (Early Essential Newborn Care)Document74 pagesEENC (Early Essential Newborn Care)Jennifer AlamonNo ratings yet
- Tirado-BSN 4D-Journal Reading Summary and ReflectionDocument4 pagesTirado-BSN 4D-Journal Reading Summary and ReflectionJeniper Marie Cute29No ratings yet
- Care of AdolescentDocument32 pagesCare of AdolescentNestor Cabacungan100% (2)
- Routine Newborn Care LectureDocument78 pagesRoutine Newborn Care LectureSheene Ainasthazia Diego AngNo ratings yet
- Ncam219 Lec PDFDocument102 pagesNcam219 Lec PDFDAVE BARIBENo ratings yet
- Module 7 - Breastfeeding and NBCDocument13 pagesModule 7 - Breastfeeding and NBCKat EstoniloNo ratings yet
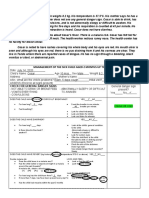
- Management of The Sick Child Aged 2 Months Up To 5 Years: Case#8: CesarDocument4 pagesManagement of The Sick Child Aged 2 Months Up To 5 Years: Case#8: CesarChloe MorningstarNo ratings yet
- What Does Your Face Says About Your Health.Document7 pagesWhat Does Your Face Says About Your Health.Harish JainNo ratings yet
- Psycho DiagnosisDocument212 pagesPsycho DiagnosisHadiqa KhanNo ratings yet
- Gastroenterology: Case Discussion: Pharmacological PerspectiveDocument21 pagesGastroenterology: Case Discussion: Pharmacological PerspectivePanini PatankarNo ratings yet
- Ebook Pediatrics Morning Report Beyond The Pearls PDF Full Chapter PDFDocument67 pagesEbook Pediatrics Morning Report Beyond The Pearls PDF Full Chapter PDFsarah.pogue790100% (26)
- Nursing Care Plan: Gen. Malvar ST., Davao CityDocument2 pagesNursing Care Plan: Gen. Malvar ST., Davao Cityscribd acctNo ratings yet
- OVERVIEW of CHN Report Sir JOSEDocument7 pagesOVERVIEW of CHN Report Sir JOSEVanessa Andrei Peralta CamelloNo ratings yet
- Complications of IV TherapyDocument2 pagesComplications of IV TherapyMarinill SolimanNo ratings yet
- Snomed CT: Coping With Concept InactivationDocument38 pagesSnomed CT: Coping With Concept InactivationMeera FarmsNo ratings yet
- NUTRITIONDocument13 pagesNUTRITIONFemale calmNo ratings yet
- Gut Dysbiosis, Leaky Gut, and Intestinal Epithelial Proliferation in Neurological Disorders Towards The Development of A New Therapeutic Using Amino Acids, Prebiotics, Probiotics, and PostbioticsDocument23 pagesGut Dysbiosis, Leaky Gut, and Intestinal Epithelial Proliferation in Neurological Disorders Towards The Development of A New Therapeutic Using Amino Acids, Prebiotics, Probiotics, and PostbioticsLevente BalázsNo ratings yet
- Social Legislation Report On SSSDocument14 pagesSocial Legislation Report On SSSBrian CbtngnNo ratings yet
- Australian and New Zealand College of Veterinary Scientists: Fellowship ExaminationDocument11 pagesAustralian and New Zealand College of Veterinary Scientists: Fellowship Examinationabazanhasan6705No ratings yet
- ChlorideDocument3 pagesChlorideMarjoNo ratings yet
- Police Annual Medical Report 2022Document98 pagesPolice Annual Medical Report 2022KAIGWA AKRAMNo ratings yet
- AutismDocument4 pagesAutismMary WanjiruNo ratings yet
- FRAILTY - Someone Who Is Skinny, Weak and Vulnerable (Cannot Be Diagnosed Based On Appearance)Document14 pagesFRAILTY - Someone Who Is Skinny, Weak and Vulnerable (Cannot Be Diagnosed Based On Appearance)Jhon Mark Miranda Santos100% (1)
- MCQ Old-Textbook-Qs-SearchableDocument45 pagesMCQ Old-Textbook-Qs-Searchableareej alblowiNo ratings yet
- Pathology of Hepatic Iron Overload: Nathan Subramaniam, PHDDocument6 pagesPathology of Hepatic Iron Overload: Nathan Subramaniam, PHDUmerNo ratings yet
- Common Heart DiseasesDocument5 pagesCommon Heart DiseasesShams MosaadNo ratings yet
- Pinworms (E.vermicularis) Mimicking Acute AppendicitisDocument2 pagesPinworms (E.vermicularis) Mimicking Acute AppendicitisMedtext PublicationsNo ratings yet
- New Horizons in Adjuvants For Vaccine Development: Steven G. Reed, Sylvie Bertholet, Rhea N. Coler and Martin FriedeDocument10 pagesNew Horizons in Adjuvants For Vaccine Development: Steven G. Reed, Sylvie Bertholet, Rhea N. Coler and Martin FriedehafsaNo ratings yet
- Foot and Ankle Surgery: Francesco Di Caprio, MD, Renato Meringolo, MD, Marwan Shehab Eddine, MD, Lorenzo Ponziani, MDDocument7 pagesFoot and Ankle Surgery: Francesco Di Caprio, MD, Renato Meringolo, MD, Marwan Shehab Eddine, MD, Lorenzo Ponziani, MDNishanthini AnnamalaiNo ratings yet
- Escaran - Drug Study - Set ADocument4 pagesEscaran - Drug Study - Set AFrancis Alfred EscaranNo ratings yet
- AbortionDocument67 pagesAbortionaneley cherinetNo ratings yet
- Activity Intolerance NCPDocument7 pagesActivity Intolerance NCPamitNo ratings yet
- Wikipedia - Peptic Ulcer (CHECKED)Document13 pagesWikipedia - Peptic Ulcer (CHECKED)pixoguiasNo ratings yet
- Benign Gestational Trophoblastic DiseaseDocument31 pagesBenign Gestational Trophoblastic Diseaseبسيل أبوهلالNo ratings yet