You might also like
- COVID-19: Effects in Comorbidities and Special PopulationsFrom EverandCOVID-19: Effects in Comorbidities and Special PopulationsNo ratings yet
- Apb 13 233Document11 pagesApb 13 233pprs6cpbrhNo ratings yet
- COVID-19 and The Renin-Angiotensin SystemDocument6 pagesCOVID-19 and The Renin-Angiotensin SystemrichabertNo ratings yet
- 2021 12 BijpsreviewDocument9 pages2021 12 BijpsreviewNguyên NguyễnNo ratings yet
- Von Willebrand Factor and Endothelial Damage: A Possible Association With Covid-19Document4 pagesVon Willebrand Factor and Endothelial Damage: A Possible Association With Covid-19Rehabilitasi Narkoba Ar RahmanNo ratings yet
- Kinins and Cytokines in COVID-19: A Comprehensive Pathophysiological ApproachDocument18 pagesKinins and Cytokines in COVID-19: A Comprehensive Pathophysiological ApproachRara AuliaNo ratings yet
- Hyperglycemia, Hydroxychloroquine, and The COVID 19 PandemicDocument6 pagesHyperglycemia, Hydroxychloroquine, and The COVID 19 PandemicMarco Antonio Tarazona MoyaNo ratings yet
- Naguib - Potential Relationships Between COVID-19 and The Thyroid Gland An UpdateDocument16 pagesNaguib - Potential Relationships Between COVID-19 and The Thyroid Gland An UpdateerixNo ratings yet
- AKI Pada Covid19Document10 pagesAKI Pada Covid19ita maghfirah IlhamjayaNo ratings yet
- A Modeling Study of The Respiratory System For An Early Intervention of COVID-19 and Its TransmissionDocument7 pagesA Modeling Study of The Respiratory System For An Early Intervention of COVID-19 and Its TransmissionPriyam NayakNo ratings yet
- Targeting Acute Kidney Injury in COVID-19: John A. Kellum, J.W. Olivier Van Till and George MulliganDocument11 pagesTargeting Acute Kidney Injury in COVID-19: John A. Kellum, J.W. Olivier Van Till and George MulliganLeticia DimanNo ratings yet
- Angiotensin-Converting Enzyme 2 (Ace2), Sars-Cov-2 and The Pathophysiology of Coronavirus Disease 2019 (Covid-19)Document21 pagesAngiotensin-Converting Enzyme 2 (Ace2), Sars-Cov-2 and The Pathophysiology of Coronavirus Disease 2019 (Covid-19)Misbahul MirnaNo ratings yet
- Role of Angiotensin-Converting Enzyme 2 (ACE2) in COVID-19: Review Open AccessDocument10 pagesRole of Angiotensin-Converting Enzyme 2 (ACE2) in COVID-19: Review Open AccessjakpowerNo ratings yet
- Sag 2004 168COVIDarticle PDFDocument14 pagesSag 2004 168COVIDarticle PDFCarolle LaoNo ratings yet
- Journal Pre-Proof: Cytokine and Growth Factor ReviewsDocument27 pagesJournal Pre-Proof: Cytokine and Growth Factor ReviewsTufik NaderNo ratings yet
- Shukla Banerjee2021 - Article - Angiotensin Converting Enzyme2Document11 pagesShukla Banerjee2021 - Article - Angiotensin Converting Enzyme2madelineNo ratings yet
- 8 DBFDocument4 pages8 DBFFatimaNo ratings yet
- AntioxidantsandCOVID 19Document13 pagesAntioxidantsandCOVID 19Anthony ChristantoNo ratings yet
- Apb 12 641Document4 pagesApb 12 641Irin Susan VargheseNo ratings yet
- Journal Pre-Proof: Nutrition, Metabolism and Cardiovascular DiseasesDocument13 pagesJournal Pre-Proof: Nutrition, Metabolism and Cardiovascular Diseasessameer sahaanNo ratings yet
- 10 Current Research Articles Related To Our SystemDocument11 pages10 Current Research Articles Related To Our Systemhomework solutionNo ratings yet
- 12996-Article Text-39447-1-10-20210901Document13 pages12996-Article Text-39447-1-10-20210901rohamaNo ratings yet
- EliabethDocument6 pagesEliabethmadelineNo ratings yet
- BMJ m1313 FullDocument2 pagesBMJ m1313 FullDzikrul Haq KarimullahNo ratings yet
- Fsoa 2021 0099Document8 pagesFsoa 2021 0099catp38647No ratings yet
- Potential Pathogenesis of Ageusia and Anosmia in COVID-19 PatientsDocument3 pagesPotential Pathogenesis of Ageusia and Anosmia in COVID-19 PatientsJonathan FergusonNo ratings yet
- Hypokalemia and Clinical Implications in Patients With Coronavirus Disease 2019 (COVID-19)Document22 pagesHypokalemia and Clinical Implications in Patients With Coronavirus Disease 2019 (COVID-19)M. Fakhrul AnamNo ratings yet
- Journal Pre-Proof: European Journal of Internal MedicineDocument30 pagesJournal Pre-Proof: European Journal of Internal MedicineNabil Sangga BuanaNo ratings yet
- The State of Changes in The Immune System in Patients Chronic Obstructive Lung Disease in Survivors of Covid-19Document5 pagesThe State of Changes in The Immune System in Patients Chronic Obstructive Lung Disease in Survivors of Covid-19Central Asian StudiesNo ratings yet
- Covid and Cardiovascular SystemDocument4 pagesCovid and Cardiovascular SystemChristine Jane Rodriguez100% (1)
- Risk of Sars-Cov-2 Infection and Covid-19 Prognosis With The Use of Renin - Angiotensin - Aldosterone System (Raas) Inhibitors: A Systematic ReviewDocument10 pagesRisk of Sars-Cov-2 Infection and Covid-19 Prognosis With The Use of Renin - Angiotensin - Aldosterone System (Raas) Inhibitors: A Systematic ReviewnembutalNo ratings yet
- Fmed 08 671215Document8 pagesFmed 08 671215Jimmy PrayogiNo ratings yet
- Covid 19 NsaidDocument5 pagesCovid 19 Nsaidsstefan888No ratings yet
- The Relationship Between Oxygen Delivery and ConsumptionDocument7 pagesThe Relationship Between Oxygen Delivery and Consumptionjcarl_20063003No ratings yet
- Molecular Hydrogen As An Adjuvant Therapy May Be ADocument6 pagesMolecular Hydrogen As An Adjuvant Therapy May Be AM FrederiksenNo ratings yet
- COVID Diabetes 2Document5 pagesCOVID Diabetes 2htapiamNo ratings yet
- TO Cells-11-00444-V3Document19 pagesTO Cells-11-00444-V3Neven ZarkovicNo ratings yet
- Hidroxicloroquina BeneficiosDocument7 pagesHidroxicloroquina BeneficiosMarco Antonio Tarazona MoyaNo ratings yet
- Extremely Highdose Insulin Requirement in A Diabetic Patient With COVID19 A Case report2020BMC Endocrine DisordersOpen AccessDocument4 pagesExtremely Highdose Insulin Requirement in A Diabetic Patient With COVID19 A Case report2020BMC Endocrine DisordersOpen AccessYOMIDES LEONCIO LOLOY CAPANo ratings yet
- Acute Kidney Injury in Hospitalized Patients With Coronavirus Disease 2019 (Covid-19) and Literature ReviewDocument5 pagesAcute Kidney Injury in Hospitalized Patients With Coronavirus Disease 2019 (Covid-19) and Literature ReviewIJAR JOURNALNo ratings yet
- 1156 ArticleText 7287 1 10 20210107Document7 pages1156 ArticleText 7287 1 10 20210107TisaNo ratings yet
- Impact of COVID 19 On Erectile Function: The Aging MaleDocument16 pagesImpact of COVID 19 On Erectile Function: The Aging MaleQuenton CompasNo ratings yet
- Tip of The Iceberg Erectile Dysfunction & 19Document6 pagesTip of The Iceberg Erectile Dysfunction & 19123123123abcdefghNo ratings yet
- E499 FullDocument6 pagesE499 FullAlizaPinkyNo ratings yet
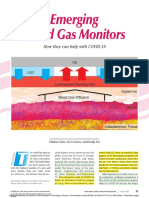
- 2020 Emerging Blood Gas MonitorsDocument15 pages2020 Emerging Blood Gas MonitorsSHANU KUMARNo ratings yet
- Potential Risk of Liver Injury in Epileptic Patients During COVID-19 2022Document11 pagesPotential Risk of Liver Injury in Epileptic Patients During COVID-19 2022Pablo Sebastián SaezNo ratings yet
- Covid y Sistema EndocrinoDocument22 pagesCovid y Sistema EndocrinocristinaNo ratings yet
- Nonsteroidal Anti-Inflammatory Drugs (Nsaids) in Covid-19 PatientDocument2 pagesNonsteroidal Anti-Inflammatory Drugs (Nsaids) in Covid-19 PatientDaniel ChávezNo ratings yet
- Aspectos Autonómicos Post CovidDocument7 pagesAspectos Autonómicos Post Covidtavo570No ratings yet
- Koc 2022Document14 pagesKoc 2022John GoranitisNo ratings yet
- Comparative Review Analysis Between Metabolic Syndrome and COVID-19Document7 pagesComparative Review Analysis Between Metabolic Syndrome and COVID-19SAPTARSHI BHATTACHARYYANo ratings yet
- COVID-19 in Elderly Adults - Clinical Features, Molecular Mechanisms, and Proposed StrategiesDocument15 pagesCOVID-19 in Elderly Adults - Clinical Features, Molecular Mechanisms, and Proposed StrategiesDanisa EpaNo ratings yet
- Silent HypoxiaDocument6 pagesSilent HypoxiaMagda CabralesNo ratings yet
- SARS-CoV-2 and Coagulation Disorders in Different OrgansDocument11 pagesSARS-CoV-2 and Coagulation Disorders in Different OrgansMaarteeh' Listing Laambeert'No ratings yet
- Male Sexual and Covid 19Document9 pagesMale Sexual and Covid 19Rima EffendiNo ratings yet
- 1479 6813 Jme 22 0036Document26 pages1479 6813 Jme 22 0036Hitesh VermaNo ratings yet
- Epid Pubmed 1 (Bab2) .En - IdDocument11 pagesEpid Pubmed 1 (Bab2) .En - IdSHAFIYA ADELINANo ratings yet
- COVID-19 Immune System Response Hyperinflammation and RepurposiDocument14 pagesCOVID-19 Immune System Response Hyperinflammation and RepurposiLizbethNo ratings yet
- COVID-19 Hypertension and Diabetes - Hunt For TheDocument5 pagesCOVID-19 Hypertension and Diabetes - Hunt For TheAditya SutarNo ratings yet
- Supplementation With Vitamin D in The COVID-19 Pandemic?: Nutrition in Clinical CareDocument9 pagesSupplementation With Vitamin D in The COVID-19 Pandemic?: Nutrition in Clinical Caresuci argithaNo ratings yet
- Curroncol 29 00642Document13 pagesCurroncol 29 00642madelineNo ratings yet
- Biomedicines 10 00804Document21 pagesBiomedicines 10 00804madelineNo ratings yet
- SuspensionDocument51 pagesSuspensionmadelineNo ratings yet
- Yue MaDocument10 pagesYue MamadelineNo ratings yet
- 5 Guideline On Establishment of Test Item in Preparation of Standards and Analytical Methods of QuasiDrugsDocument21 pages5 Guideline On Establishment of Test Item in Preparation of Standards and Analytical Methods of QuasiDrugsmadelineNo ratings yet
- Ssentogo Et Al.,2020Document7 pagesSsentogo Et Al.,2020madelineNo ratings yet
- JMV 9999 NaDocument2 pagesJMV 9999 NamadelineNo ratings yet
- Shukla Banerjee2021 - Article - Angiotensin Converting Enzyme2Document11 pagesShukla Banerjee2021 - Article - Angiotensin Converting Enzyme2madelineNo ratings yet
- Park Et Al., 2021Document11 pagesPark Et Al., 2021madelineNo ratings yet
- Potential Harmful Effects of Discontinuing Ace-Inhibitors and Arbs in Covid-19 PatientsDocument8 pagesPotential Harmful Effects of Discontinuing Ace-Inhibitors and Arbs in Covid-19 PatientsmadelineNo ratings yet
- The Effects of Solvent Polarity On Analgesic and Aanti Inflammatory Activities of Portulaca Oleracea ExtractsDocument16 pagesThe Effects of Solvent Polarity On Analgesic and Aanti Inflammatory Activities of Portulaca Oleracea ExtractsmadelineNo ratings yet
- Evaluation of Anti-Inflammatory Activity: Portulaca SpeciesDocument1 pageEvaluation of Anti-Inflammatory Activity: Portulaca SpeciesmadelineNo ratings yet
- In Vitro Effects of Thai Medicinal Plants On Human Lymphocyte Activity PDFDocument8 pagesIn Vitro Effects of Thai Medicinal Plants On Human Lymphocyte Activity PDFmadelineNo ratings yet
- Module 1 - Animal Handling Basic Information of Pharmacology PracticumDocument14 pagesModule 1 - Animal Handling Basic Information of Pharmacology PracticummadelineNo ratings yet
- Chapter 14: Coliforms, Fecal Coliforms and Escherichia Coli: UpdatedDocument23 pagesChapter 14: Coliforms, Fecal Coliforms and Escherichia Coli: UpdatedBening setara bulanNo ratings yet
- Funda 6Document4 pagesFunda 6Nur SetsuNo ratings yet
- Literature Review On Hepatitis B VirusDocument5 pagesLiterature Review On Hepatitis B Virusafmzeracmdvbfe100% (1)
- Grade 8 Health Q1Document21 pagesGrade 8 Health Q1Jayhia Malaga JarlegaNo ratings yet
- The Silva Method - Mental Power PDFDocument5 pagesThe Silva Method - Mental Power PDFubuntulad88% (24)
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- Pharma Sub Part Unit 2Document6 pagesPharma Sub Part Unit 2Beverly DatuNo ratings yet
- Nursing Care PlanDocument11 pagesNursing Care PlanJan DamesNo ratings yet
- Safety Pilot Study On DoctorsDocument4 pagesSafety Pilot Study On DoctorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Positive and Negative Syndrome Scale (Panss) Rating Criteria General Rating Instructions Panss Rating FormDocument2 pagesPositive and Negative Syndrome Scale (Panss) Rating Criteria General Rating Instructions Panss Rating FormInshrah MukhtarNo ratings yet
- PHARMACOLOGY (POST TEST With Rationale)Document30 pagesPHARMACOLOGY (POST TEST With Rationale)Xyrelle Denise ReyesNo ratings yet
- Handout E4N Unit 1Document4 pagesHandout E4N Unit 1Ratu Aldi NingrumNo ratings yet
- Test 10 Bank in Abnormal Psychology Chapter 10Document41 pagesTest 10 Bank in Abnormal Psychology Chapter 10sirfrankvincentmendozaNo ratings yet
- The Misuse of Mobile PhoneDocument3 pagesThe Misuse of Mobile Phoneyisethe melisa erira menesesNo ratings yet
- Operative Vaginal Delivery: Ralphe Robert C. CajucomDocument41 pagesOperative Vaginal Delivery: Ralphe Robert C. CajucomThea ConcepcionNo ratings yet
- Kit Insert - LDL-CDocument2 pagesKit Insert - LDL-CtamacahyaNo ratings yet
- Single Stranded DNADocument6 pagesSingle Stranded DNAHannah Alvarado Bandola100% (1)
- Laporan Pendahuluan Sindrom Koroner Akut (Ska) I. Laporan PendahuluanDocument14 pagesLaporan Pendahuluan Sindrom Koroner Akut (Ska) I. Laporan PendahuluanBahiya Az ZahraNo ratings yet
- June 2018 (IAL) MS - Unit 1 Edexcel Biology A-Level PDFDocument23 pagesJune 2018 (IAL) MS - Unit 1 Edexcel Biology A-Level PDFMoataz NassefNo ratings yet
- Stressors Factors Experienced by Hospitalized Elderly From The Perspective of The Neuman Systems ModelDocument9 pagesStressors Factors Experienced by Hospitalized Elderly From The Perspective of The Neuman Systems ModelXian Cristy ParchasoNo ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument5 pagesCollege of Health Sciences: Urdaneta City UniversityDan Dan ManaoisNo ratings yet
- 3996 11820 1 SMDocument8 pages3996 11820 1 SMindah rahmaNo ratings yet
- USPIE CSE Position StatementDocument2 pagesUSPIE CSE Position StatementCoralC21No ratings yet
- Seed HealthTestingDocument9 pagesSeed HealthTestingMd. Sajjad HossenNo ratings yet
- Bio Mattress and Bio Mat: A Company Committed To Product ExcellenceDocument15 pagesBio Mattress and Bio Mat: A Company Committed To Product Excellencethe secretplace2No ratings yet
- Further Distancing Between The Rich and The PoorDocument2 pagesFurther Distancing Between The Rich and The Poorjc de velaNo ratings yet
- Research PaperDocument75 pagesResearch PaperMa. Victoria RamosNo ratings yet
- Waiters Salmeterol PDFDocument1 pageWaiters Salmeterol PDFmp1757No ratings yet
- MEDTRONIC Placa Cervical VentureDocument19 pagesMEDTRONIC Placa Cervical Ventureruiduart100% (1)
- Orthopaedics & Trauma: SamsonDocument17 pagesOrthopaedics & Trauma: Samsonزكريا عمرNo ratings yet
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeFrom EverandChemistry for Breakfast: The Amazing Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (14)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactRating: 5 out of 5 stars5/5 (5)
- Dust Explosion and Fire Prevention Handbook: A Guide to Good Industry PracticesFrom EverandDust Explosion and Fire Prevention Handbook: A Guide to Good Industry PracticesNo ratings yet
- Chemistry: a QuickStudy Laminated Reference GuideFrom EverandChemistry: a QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- Applied Geochemistry: Advances in Mineral Exploration TechniquesFrom EverandApplied Geochemistry: Advances in Mineral Exploration TechniquesNo ratings yet
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeFrom EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeRating: 5 out of 5 stars5/5 (4)
- Practical Approaches to Method Validation and Essential Instrument QualificationFrom EverandPractical Approaches to Method Validation and Essential Instrument QualificationNo ratings yet
- The Unfortunate Truth About Vaccines: Exposing the Vaccine OrthodoxyFrom EverandThe Unfortunate Truth About Vaccines: Exposing the Vaccine OrthodoxyRating: 5 out of 5 stars5/5 (1)
- Formulating, Packaging, and Marketing of Natural Cosmetic ProductsFrom EverandFormulating, Packaging, and Marketing of Natural Cosmetic ProductsNo ratings yet
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideFrom EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNo ratings yet
- Guidelines for Asset Integrity ManagementFrom EverandGuidelines for Asset Integrity ManagementRating: 5 out of 5 stars5/5 (1)
- Long Hard Road: The Lithium-Ion Battery and the Electric CarFrom EverandLong Hard Road: The Lithium-Ion Battery and the Electric CarRating: 4.5 out of 5 stars4.5/5 (2)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactRating: 5 out of 5 stars5/5 (1)
- Essential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilFrom EverandEssential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilRating: 5 out of 5 stars5/5 (1)
- It's Elemental: The Hidden Chemistry in EverythingFrom EverandIt's Elemental: The Hidden Chemistry in EverythingRating: 4 out of 5 stars4/5 (10)
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolFrom EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolNo ratings yet