You might also like
- Ameloblastomatous Calcifying Odontogenic Cyst: A Case Report of A Rare Histologic VariantDocument4 pagesAmeloblastomatous Calcifying Odontogenic Cyst: A Case Report of A Rare Histologic VariantindhupriyakNo ratings yet
- Kishimoto 2009Document8 pagesKishimoto 2009anitaabreu123No ratings yet
- Kishimoto 2009Document8 pagesKishimoto 2009anitaabreu123No ratings yet
- 2013 - Holtzclaw - Amnion Chorion Allograft Barrier Used For Guided Tissue Regeneration TreatmentDocument7 pages2013 - Holtzclaw - Amnion Chorion Allograft Barrier Used For Guided Tissue Regeneration TreatmentJontavius GilbertNo ratings yet
- Ameloblastoma Arising in A Dentigerous Cyst: Report of Three CasesDocument6 pagesAmeloblastoma Arising in A Dentigerous Cyst: Report of Three Casessantos eddyNo ratings yet
- Horizontal Ridge Augmentation Using GBR With A Native Collagen Membrane and 1:1 Ratio of Particulate Xenograft and Autologous Bone: A 3 Year After Final Loading Prospective Clinical StudyDocument9 pagesHorizontal Ridge Augmentation Using GBR With A Native Collagen Membrane and 1:1 Ratio of Particulate Xenograft and Autologous Bone: A 3 Year After Final Loading Prospective Clinical StudyYodel SrnthNo ratings yet
- Hed 20192Document6 pagesHed 20192Tiago TavaresNo ratings yet
- Okc PDFDocument6 pagesOkc PDFanggiNo ratings yet
- Corneal Sensitivity and Ocular Surface Changes Following Preserved Amniotic Membrane Transplantation For Nonhealing Corneal UlcersDocument10 pagesCorneal Sensitivity and Ocular Surface Changes Following Preserved Amniotic Membrane Transplantation For Nonhealing Corneal UlcersDitha FadhilaNo ratings yet
- 2 YdcDocument8 pages2 YdcŞahin ŞahinNo ratings yet
- The Effect of Complete Dentures On Alveolar MucosaDocument8 pagesThe Effect of Complete Dentures On Alveolar MucosaZachary DuongNo ratings yet
- Fulltext - Jda v5 Id1107Document3 pagesFulltext - Jda v5 Id1107Sahana RangarajanNo ratings yet
- 1 s2.0 S2210261223007721 MainDocument5 pages1 s2.0 S2210261223007721 MainEduardo BarbosaNo ratings yet
- Keratopati BulosaDocument7 pagesKeratopati BulosaShafira LusianaNo ratings yet
- Parakeratinized Odontogenic Keratocyst: A Case Report With 8 Years Follow-UpDocument4 pagesParakeratinized Odontogenic Keratocyst: A Case Report With 8 Years Follow-UpIJAR JOURNALNo ratings yet
- Free Flaps MaxillaDocument7 pagesFree Flaps MaxillaFahad QiamNo ratings yet
- Tumores OdontogenicosDocument8 pagesTumores OdontogenicosMeditador OficialNo ratings yet
- Argument For The Conservative Management of Mandibular AmeloblastomasDocument5 pagesArgument For The Conservative Management of Mandibular AmeloblastomasVincentius Novian RomilioNo ratings yet
- Flap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelDocument9 pagesFlap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelFlorina PopaNo ratings yet
- Tabrizi2012marsupialization As A Treatment Option For The Odontogenic KeratocystDocument3 pagesTabrizi2012marsupialization As A Treatment Option For The Odontogenic KeratocystquetmauhamNo ratings yet
- Prosthodontic Rehabilitation of Residual Mandibular Defect With Fixed Removable Hybrid Prosthesis-A Case ReportDocument4 pagesProsthodontic Rehabilitation of Residual Mandibular Defect With Fixed Removable Hybrid Prosthesis-A Case ReportnastitiiNo ratings yet
- Case Series: Single-Flap Approach in Periodontal Regeneration For Intraosseous Defects: Case SeriesDocument6 pagesCase Series: Single-Flap Approach in Periodontal Regeneration For Intraosseous Defects: Case SeriesJoshua Diaz QuiquijanaNo ratings yet
- In Vitro Investigation of Gelatin/Polycaprolactone Nano Bers in Modulating Human Gingival Mesenchymal Stromal CellsDocument15 pagesIn Vitro Investigation of Gelatin/Polycaprolactone Nano Bers in Modulating Human Gingival Mesenchymal Stromal CellsZhongqi ZhaoNo ratings yet
- A Parulis-Like Soft Tissue Tumor in Relation With A Dental Implant: Case ReportDocument3 pagesA Parulis-Like Soft Tissue Tumor in Relation With A Dental Implant: Case ReportDr. AtheerNo ratings yet
- Preserving of A Tooth Related With Central Giant Cell Granuloma With Noninvasive Curettage Years Followedup Case ReportDocument4 pagesPreserving of A Tooth Related With Central Giant Cell Granuloma With Noninvasive Curettage Years Followedup Case ReportMaya GusmanNo ratings yet
- Periorbital Dermoid Cyst PDFDocument3 pagesPeriorbital Dermoid Cyst PDFRicarhdo Valentino HanafiNo ratings yet
- QueratoquisteDocument10 pagesQueratoquisteicmNo ratings yet
- Bios GraftDocument7 pagesBios GraftAndrei TuicaNo ratings yet
- Bozkurt Et Al-2014-Clinical Oral Implants ResearchDocument9 pagesBozkurt Et Al-2014-Clinical Oral Implants ResearchAlfred OrozcoNo ratings yet
- Oral Bilateral Collagenous Fibroma A Previously Unreported Case and Literature ReviewDocument4 pagesOral Bilateral Collagenous Fibroma A Previously Unreported Case and Literature ReviewRichard LimaNo ratings yet
- Aaid Joi D 12 00028Document9 pagesAaid Joi D 12 00028NancyLiaoNo ratings yet
- Diagnostic and Therapeutic Pieges Before Clinicoradiological Elements Eviding A Mandibular AmeloblastomaDocument4 pagesDiagnostic and Therapeutic Pieges Before Clinicoradiological Elements Eviding A Mandibular AmeloblastomaAnjay MabarNo ratings yet
- Queratoquiste OdontogénicoDocument4 pagesQueratoquiste OdontogénicoBetsaida Escandón MoronesNo ratings yet
- Young2008 (1) - 1Document13 pagesYoung2008 (1) - 1dehaaNo ratings yet
- Comparative Biocompatibility and Osteogenic Potential of Two Bioceramic SealersDocument6 pagesComparative Biocompatibility and Osteogenic Potential of Two Bioceramic SealerssarmientocornejoNo ratings yet
- Surgical and Endodontic Management of Large Cystic Lesion: AbstractDocument5 pagesSurgical and Endodontic Management of Large Cystic Lesion: AbstractanamaghfirohNo ratings yet
- Morphological Immunochemical: HypertrophicDocument9 pagesMorphological Immunochemical: HypertrophicRarasati SrimurniNo ratings yet
- Bimaxillary Dentoalveolar Protrusion - Traits and Orthodontic CorrectionDocument7 pagesBimaxillary Dentoalveolar Protrusion - Traits and Orthodontic CorrectionAzra NadhiraNo ratings yet
- Sialolithiasis - A Report of Two Cases and ReviewDocument4 pagesSialolithiasis - A Report of Two Cases and Reviewmaharani spNo ratings yet
- Jurnal 22 PDFDocument4 pagesJurnal 22 PDFsriwahyuutamiNo ratings yet
- Metaplastic Epithelium in An Odontogenic Keratocyte. A Case ReportDocument3 pagesMetaplastic Epithelium in An Odontogenic Keratocyte. A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Immediate or Early Placement of Implants Following Tooth Extraction: Review of Biologic Basis, Clinical Procedures, and OutcomesDocument15 pagesImmediate or Early Placement of Implants Following Tooth Extraction: Review of Biologic Basis, Clinical Procedures, and OutcomesFelipe CastroNo ratings yet
- Clinical Study: A Liquid Membrane As A Barrier Membrane For Guided Bone RegenerationDocument6 pagesClinical Study: A Liquid Membrane As A Barrier Membrane For Guided Bone RegenerationStanislav ȘuiuNo ratings yet
- Ameloblastoma Arising From Gorlins Cyst: A Rare Case ReportDocument4 pagesAmeloblastoma Arising From Gorlins Cyst: A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Granular Cell Odontogenic Tumour: Case Report and Review of LiteratureDocument4 pagesGranular Cell Odontogenic Tumour: Case Report and Review of LiteratureBharath SreenivasNo ratings yet
- 1 s2.0 S0002939411008993 MainDocument1 page1 s2.0 S0002939411008993 MainCupris23No ratings yet
- International Journal of Health Sciences and ResearchDocument6 pagesInternational Journal of Health Sciences and ResearchDentist HereNo ratings yet
- Temporalis Muscle Flap For The Immediate Reconstruction of Oral Defects After Oncologic ResectionDocument7 pagesTemporalis Muscle Flap For The Immediate Reconstruction of Oral Defects After Oncologic ResectionSanjay RinaNo ratings yet
- A Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyDocument4 pagesA Novel Strategy To Achieve Stable and Lasting Double Eyelids in Upper BlepharoplastyRaul FonsecaNo ratings yet
- Holtzclaw2013 PDFDocument7 pagesHoltzclaw2013 PDFpallav GanataNo ratings yet
- Periosteal Pocket Flap For Horizontal Bone RegenerDocument10 pagesPeriosteal Pocket Flap For Horizontal Bone RegenerViorel Ion100% (1)
- Regenerationof Periodontaltissues: Guidedtissue RegenerationDocument20 pagesRegenerationof Periodontaltissues: Guidedtissue RegenerationPiyusha SharmaNo ratings yet
- Guided Tissue Regeneration in Jaw Reconstruction: Review and ApplicationsDocument2 pagesGuided Tissue Regeneration in Jaw Reconstruction: Review and ApplicationsNurhidayah hasanNo ratings yet
- Factors Influencing The Recurrence of KeratocystsDocument8 pagesFactors Influencing The Recurrence of KeratocystsRocio CacñahuarayNo ratings yet
- Alveolar Bone Preservation in Extraction Sockets Using Non-Resorbable dPTFE Membranes: A Retrospective Non-Randomized StudyDocument15 pagesAlveolar Bone Preservation in Extraction Sockets Using Non-Resorbable dPTFE Membranes: A Retrospective Non-Randomized StudyDiego SiqueiraNo ratings yet
- Easy Graft: "Bioabsorbable Root Analogue For Closure of Oroantral Communications After Tooth Extraction: A Prospective Case-Cohort Study"Document7 pagesEasy Graft: "Bioabsorbable Root Analogue For Closure of Oroantral Communications After Tooth Extraction: A Prospective Case-Cohort Study"Dentapex ThailandNo ratings yet
- Recurrent Peripheral Odontogenic Keratocyst: A Case ReportDocument3 pagesRecurrent Peripheral Odontogenic Keratocyst: A Case ReportthedocperuNo ratings yet
- Recurrence Odontogenic Keratocyst of The Mandible Treated by Surgical Hemimandibulectomy: Case ReportDocument10 pagesRecurrence Odontogenic Keratocyst of The Mandible Treated by Surgical Hemimandibulectomy: Case Reportarbi123No ratings yet
- Cholesterol Crystals in Periapical Lesions of Root Filled TeethDocument7 pagesCholesterol Crystals in Periapical Lesions of Root Filled TeethCarlos BelsuzarriNo ratings yet
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- A Semi-Detailed Lesson Plan in English Grade 8 Focus: Reading SkillDocument4 pagesA Semi-Detailed Lesson Plan in English Grade 8 Focus: Reading SkillKim KimNo ratings yet
- Numl Lahore Campus Break Up of Fee (From 1St To 8Th Semester) Spring-Fall 2016Document1 pageNuml Lahore Campus Break Up of Fee (From 1St To 8Th Semester) Spring-Fall 2016sajeeNo ratings yet
- Information TechnologyDocument7 pagesInformation TechnologyRosenildo Palheta Coutinho0% (1)
- Omkar's ResumeDocument1 pageOmkar's ResumeOmkar RaneNo ratings yet
- Weebly ResumeDocument1 pageWeebly Resumeapi-272737031No ratings yet
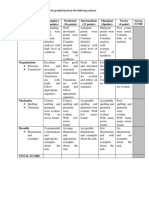
- 20 Points RubricsDocument1 page20 Points RubricsJerome Formalejo,No ratings yet
- Assignment Set No. 3 - Nieva O. MairinaDocument6 pagesAssignment Set No. 3 - Nieva O. MairinaNieva MairinaNo ratings yet
- 05b6-1714:documents (1) /gender Development (Reflection)Document3 pages05b6-1714:documents (1) /gender Development (Reflection)Queenie Carale0% (1)
- The Writing Block: Cheryl M. SigmonDocument4 pagesThe Writing Block: Cheryl M. Sigmoneva.bensonNo ratings yet
- TheoriesDocument14 pagesTheoriesChristine Joy DelaCruz CorpuzNo ratings yet
- Notes For Teaching ProfessionDocument4 pagesNotes For Teaching ProfessionJames JaramilloNo ratings yet
- Educ 121 My Virtual ChildDocument5 pagesEduc 121 My Virtual Childapi-378042907No ratings yet
- Rubric Shom Art Exploration Shoe DrawingDocument1 pageRubric Shom Art Exploration Shoe Drawingapi-201056542100% (1)
- Key Point Slides - Ch5Document21 pagesKey Point Slides - Ch5Nuzul DwiNo ratings yet
- Conducting A Nurse Consultation: ClinicalDocument6 pagesConducting A Nurse Consultation: ClinicalAlif Akbar HasyimiNo ratings yet
- Human Anatomy and Physiology Course OutlineDocument16 pagesHuman Anatomy and Physiology Course OutlineDEVORAH CARUZNo ratings yet
- Empowerment TechnologiesDocument72 pagesEmpowerment TechnologiesMark Jake RodriguezNo ratings yet
- Linguistic FunctionsDocument42 pagesLinguistic FunctionsRussel John CalloNo ratings yet
- Automated School Form 2 Kasapa Grade 3Document75 pagesAutomated School Form 2 Kasapa Grade 3JUN CARLO MINDAJAONo ratings yet
- Elder Sharmaine 15166272 Ede101 Assessment2Document10 pagesElder Sharmaine 15166272 Ede101 Assessment2api-240004103No ratings yet
- Tugas Bahasa InggrisDocument10 pagesTugas Bahasa InggrisFirdanNo ratings yet
- Poptropica English AmE TB Level 3Document227 pagesPoptropica English AmE TB Level 3Anita Magaly Anita100% (1)
- Essay On RamayanaDocument3 pagesEssay On Ramayanalmfbcmaeg100% (1)
- Cumberland Youth Football Registration 2021Document3 pagesCumberland Youth Football Registration 2021api-293704297No ratings yet
- Automated ML Approaches To Discriminate The Autism-Categorical Spectrum DisorderDocument5 pagesAutomated ML Approaches To Discriminate The Autism-Categorical Spectrum Disorderibmlenovo2021No ratings yet
- Action Plan in MathDocument4 pagesAction Plan in MathRoselyn Catubig Vidad Jumadla100% (4)
- Classroom Assessments Checklists, Rating Scales, and RubricsDocument24 pagesClassroom Assessments Checklists, Rating Scales, and RubricsJoseph Ajayi FAYOMINo ratings yet
- Ya Literature Past and PresentDocument10 pagesYa Literature Past and Presentapi-296864651No ratings yet
- Contoh DAFTAR PUSTAKADocument6 pagesContoh DAFTAR PUSTAKATegar PrakarsaNo ratings yet
- GE 1 (Activities) Understanding SelfDocument28 pagesGE 1 (Activities) Understanding Selfbethojim0% (1)