You might also like
- Anatomy of Respiratory SystemDocument75 pagesAnatomy of Respiratory SystemAnonymous aqeaNUn80% (5)
- Grade 10 Science NotesDocument43 pagesGrade 10 Science NotesIoana Burtea89% (27)
- EmfizemulDocument19 pagesEmfizemulMirela IoanaNo ratings yet
- Abdominal Ultrasound Anatomy.: DR/ Abd Allah Nazeer. MDDocument50 pagesAbdominal Ultrasound Anatomy.: DR/ Abd Allah Nazeer. MDAri Dwi PrasetyoNo ratings yet
- Ian M Symonds Sabaratnam Arulkumaran E M Symonds Essential Obstetrics and Gynaecology PDFDocument449 pagesIan M Symonds Sabaratnam Arulkumaran E M Symonds Essential Obstetrics and Gynaecology PDFVilde Lie100% (8)
- ZL 124 Lecture 7 - Gastrulation in Birds & MammalsDocument36 pagesZL 124 Lecture 7 - Gastrulation in Birds & MammalsNestory MartineNo ratings yet
- The Cardiovascular System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical CollegeDocument124 pagesThe Cardiovascular System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical Collegelourd nabNo ratings yet
- Accessory OrgansDocument43 pagesAccessory Organslouradel100% (1)
- Who Classification of Head & Neck Tumors - 2017Document343 pagesWho Classification of Head & Neck Tumors - 2017Pablo Enrique Mejia Paz78% (40)
- Kishimoto 2009Document8 pagesKishimoto 2009anitaabreu123No ratings yet
- Resorbable Collagen Membranes: Histopathologic Features: ResultsDocument5 pagesResorbable Collagen Membranes: Histopathologic Features: Resultsحسن عسيريNo ratings yet
- Bone Regeneration in Sinus Lifts: Comparing Tissue-Engineered Bone and Iliac BoneDocument6 pagesBone Regeneration in Sinus Lifts: Comparing Tissue-Engineered Bone and Iliac BoneArmando Renteria BravoNo ratings yet
- Lou Et Al (2018) - Wound-Healing Effects of 635-nm Low-Level Laser Therapy On Primary Human Vocal Fold Epithelial Cells An in Vitro StudyDocument8 pagesLou Et Al (2018) - Wound-Healing Effects of 635-nm Low-Level Laser Therapy On Primary Human Vocal Fold Epithelial Cells An in Vitro StudyRobson LemosNo ratings yet
- 1990 RozemaDocument5 pages1990 Rozemapiyush joshiNo ratings yet
- The New "Cubism" Graft Technique in Tympanoplasty - A Randomized Controlled TrialDocument9 pagesThe New "Cubism" Graft Technique in Tympanoplasty - A Randomized Controlled Trialian danarkoNo ratings yet
- PRP Treatment Accelerates Healing of Acute Vocal Fold InjuriesDocument5 pagesPRP Treatment Accelerates Healing of Acute Vocal Fold InjuriesConstantin StanNo ratings yet
- Flap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelDocument9 pagesFlap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelFlorina PopaNo ratings yet
- Yoshimoto 2004Document5 pagesYoshimoto 2004r1comfupchNo ratings yet
- Fat Augmentation Vocal FoldsDocument8 pagesFat Augmentation Vocal FoldsRoy HallakNo ratings yet
- The Z-Meatoplasty For Modified Radical Mastoidectomy in ChildrenDocument4 pagesThe Z-Meatoplasty For Modified Radical Mastoidectomy in ChildrenMita DaudNo ratings yet
- Auricular Prostheses and Osseointegrated Implants: Experience UclaDocument6 pagesAuricular Prostheses and Osseointegrated Implants: Experience UclanoranNo ratings yet
- Mastoid Obliteration 1916-0216-42-49 PDFDocument7 pagesMastoid Obliteration 1916-0216-42-49 PDFFurqan MirzaNo ratings yet
- Bimaxillary Dentoalveolar Protrusion Traits andDocument7 pagesBimaxillary Dentoalveolar Protrusion Traits andSAM PRASANTHNo ratings yet
- Lanigan 1993Document15 pagesLanigan 1993MarkNo ratings yet
- Etiology and Treatment of Congenital Festoons PDFDocument11 pagesEtiology and Treatment of Congenital Festoons PDFprashanth kenchotiNo ratings yet
- The Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle DefectsDocument5 pagesThe Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle Defectslia indria watiNo ratings yet
- Granuloma PCLDocument5 pagesGranuloma PCLEmrys1987No ratings yet
- Bimaxillary Dentoalveolar Protrusion - Traits and Orthodontic CorrectionDocument7 pagesBimaxillary Dentoalveolar Protrusion - Traits and Orthodontic CorrectionAzra NadhiraNo ratings yet
- Fulco Et Al 2014Document10 pagesFulco Et Al 2014Alex PerryNo ratings yet
- IJGMP - Medicine - Clinical Study of DALK in Heterogeneous Corneal Diseases - Srinivas K.HDocument6 pagesIJGMP - Medicine - Clinical Study of DALK in Heterogeneous Corneal Diseases - Srinivas K.Hiaset123No ratings yet
- Okc PDFDocument6 pagesOkc PDFanggiNo ratings yet
- Auricular Prostheses and Osseointegrated Implants: Experience UclaDocument6 pagesAuricular Prostheses and Osseointegrated Implants: Experience UclaPablo Gutiérrez Da VeneziaNo ratings yet
- Endofistula Laser Ablation of Fistula-In-Ano - A New Minimally Invasive Technique For The Treatment of Fistula-In-AnoDocument6 pagesEndofistula Laser Ablation of Fistula-In-Ano - A New Minimally Invasive Technique For The Treatment of Fistula-In-AnoagusNo ratings yet
- Guided Tissue Regeneration in Jaw Reconstruction: Review and ApplicationsDocument2 pagesGuided Tissue Regeneration in Jaw Reconstruction: Review and ApplicationsNurhidayah hasanNo ratings yet
- Modeling of human extraction socketsDocument10 pagesModeling of human extraction socketsMahendra PrihandanaNo ratings yet
- Tube Exposure Repair: 10.5005/jp-Journals-10008-1121Document4 pagesTube Exposure Repair: 10.5005/jp-Journals-10008-1121alineochoaaNo ratings yet
- Mother Touch in Periodontal Therapy: Chorion MembraneDocument7 pagesMother Touch in Periodontal Therapy: Chorion MembraneInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1998-Ricucci-Apical - Limit-II-IEJ PDFDocument17 pages1998-Ricucci-Apical - Limit-II-IEJ PDFGhenciu AndreiNo ratings yet
- RTGD RaspunsuriDocument17 pagesRTGD RaspunsuriDan BrynzaNo ratings yet
- Cranioplasty FinalDocument13 pagesCranioplasty Finalinfobusiness2010No ratings yet
- Easy Graft: "Bioabsorbable Root Analogue For Closure of Oroantral Communications After Tooth Extraction: A Prospective Case-Cohort Study"Document7 pagesEasy Graft: "Bioabsorbable Root Analogue For Closure of Oroantral Communications After Tooth Extraction: A Prospective Case-Cohort Study"Dentapex ThailandNo ratings yet
- Pathological Examination of Experimentally Induced Periodontal Polyp in Mice Technical NoteDocument4 pagesPathological Examination of Experimentally Induced Periodontal Polyp in Mice Technical NotekarinaNo ratings yet
- Ghan em 2005Document5 pagesGhan em 2005asfwegereNo ratings yet
- Cleft Palate CaseDocument5 pagesCleft Palate CaseyomifNo ratings yet
- Free Flaps MaxillaDocument7 pagesFree Flaps MaxillaFahad QiamNo ratings yet
- Study of Jones Procedure For Senile Entropion: Medical ScienceDocument3 pagesStudy of Jones Procedure For Senile Entropion: Medical SciencedhitadwynNo ratings yet
- Management of Broken Instrument by File Bypass Technique: Sultana Parveen, Mozammal Hossain and Md. Farid UddinDocument3 pagesManagement of Broken Instrument by File Bypass Technique: Sultana Parveen, Mozammal Hossain and Md. Farid UddinsetiabektidwikiNo ratings yet
- 00011Document10 pages00011M Joaquin Robles OrtizNo ratings yet
- Tunkel Comparacion Tecnicas2013Document9 pagesTunkel Comparacion Tecnicas2013SergioNo ratings yet
- Surgical Therapy of Peri-ImplantitisDocument17 pagesSurgical Therapy of Peri-Implantitiskaue francoNo ratings yet
- Histological Evaluation of Healing And: Revascularization of The Subepithelial Connective Tissue GraftDocument10 pagesHistological Evaluation of Healing And: Revascularization of The Subepithelial Connective Tissue GraftHector MurilloNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars.Document11 pagesA Long-Term Study of 370 Autotransplanted Premolars.jing.zhao222No ratings yet
- Kim2016 Pdo MultifilamenDocument5 pagesKim2016 Pdo Multifilamenyolanda tejaNo ratings yet
- Implant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoDocument6 pagesImplant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoMelina Nataly Robles AcuñaNo ratings yet
- A Hollow Delayed Surgical ObturatorDocument55 pagesA Hollow Delayed Surgical ObturatorvinnycoolbuddyNo ratings yet
- 99 IJPRD EMD TechDocument10 pages99 IJPRD EMD Techinamboy7No ratings yet
- Effect of Hyaluronic Acid On The Osseointegration of Dental ImplantsDocument5 pagesEffect of Hyaluronic Acid On The Osseointegration of Dental Implantsjaviers45No ratings yet
- Frontolateral Partial LaryngectomyDocument7 pagesFrontolateral Partial LaryngectomyJeremy HermantoNo ratings yet
- Congress Auricular Reconstruction AbstractsDocument92 pagesCongress Auricular Reconstruction AbstractsRocio RamirezNo ratings yet
- Conjunctival-Limbal Autograft Effective for Primary, Recurrent PterygiumDocument3 pagesConjunctival-Limbal Autograft Effective for Primary, Recurrent PterygiumMichael HumiantoNo ratings yet
- The Internolionol Joumal o (Periodontics & Restorolive DentishyDocument21 pagesThe Internolionol Joumal o (Periodontics & Restorolive DentishyJohanna Andrea CalderónNo ratings yet
- Carnoy's Solution in The Management of Odontogenic KeratocystDocument4 pagesCarnoy's Solution in The Management of Odontogenic KeratocystlydiaNo ratings yet
- Spiegel 2004Document5 pagesSpiegel 2004manuel abantoNo ratings yet
- Perichondrium Graft: Harvesting and Indications in Nasal SurgeryDocument5 pagesPerichondrium Graft: Harvesting and Indications in Nasal SurgerySyahnidel FitaNo ratings yet
- Horizontal Ridge Augmentation Using GBR With A Native Collagen Membrane and 1:1 Ratio of Particulate Xenograft and Autologous Bone: A 3 Year After Final Loading Prospective Clinical StudyDocument9 pagesHorizontal Ridge Augmentation Using GBR With A Native Collagen Membrane and 1:1 Ratio of Particulate Xenograft and Autologous Bone: A 3 Year After Final Loading Prospective Clinical StudyYodel SrnthNo ratings yet
- Intl J Gynecology Obste - 2023 - Clark - Dehydrated Human Amniotic Membrane and Amniotic Fluid Allograft For TheDocument3 pagesIntl J Gynecology Obste - 2023 - Clark - Dehydrated Human Amniotic Membrane and Amniotic Fluid Allograft For TheUrología GinecológicaNo ratings yet
- Dapus 11 Referat 2Document3 pagesDapus 11 Referat 2Akramanto RidwanNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Surgical Management of Childhood Glaucoma: Clinical Considerations and TechniquesFrom EverandSurgical Management of Childhood Glaucoma: Clinical Considerations and TechniquesAlana L. GrajewskiNo ratings yet
- TracheostomyDocument10 pagesTracheostomyanitaabreu123No ratings yet
- Allergic Rhinitis Clinical GuidelineDocument43 pagesAllergic Rhinitis Clinical Guidelineanitaabreu123No ratings yet
- Sulcus Mucosal Slicing TecniqueDocument9 pagesSulcus Mucosal Slicing Tecniqueanitaabreu123No ratings yet
- Clinical Practice Guideline: Tympanostomy Tubes in Children (Update)Document56 pagesClinical Practice Guideline: Tympanostomy Tubes in Children (Update)anitaabreu123No ratings yet
- Brandt Daroff Excercises Quick GuideDocument9 pagesBrandt Daroff Excercises Quick GuideEldar SulejmanovicNo ratings yet
- (Revisi) NANDA CSS - ParotitisDocument40 pages(Revisi) NANDA CSS - Parotitisbunga juliaNo ratings yet
- Preauricular SinusDocument2 pagesPreauricular Sinusanitaabreu123No ratings yet
- Correcting Caudal Septal Deviation With A Modified Horizontal Mattress SutureDocument3 pagesCorrecting Caudal Septal Deviation With A Modified Horizontal Mattress Sutureanitaabreu123No ratings yet
- Vocal Fold Scars - A Common Classifcation Proposal by The AmericanDocument4 pagesVocal Fold Scars - A Common Classifcation Proposal by The Americananitaabreu123No ratings yet
- Vocal Fold Scars Current Concepts and Future Directions. Consensus Report of The Phonosurgery Committee of The European Laryngological SocietyDocument17 pagesVocal Fold Scars Current Concepts and Future Directions. Consensus Report of The Phonosurgery Committee of The European Laryngological Societyanitaabreu123No ratings yet
- Sulcus Mucosal Slicing TecniqueDocument9 pagesSulcus Mucosal Slicing Tecniqueanitaabreu123No ratings yet
- Vocal Fold Scars - A Common Classifcation Proposal by The AmericanDocument4 pagesVocal Fold Scars - A Common Classifcation Proposal by The Americananitaabreu123No ratings yet
- Prevalence of Minor Larynx StructuralDocument7 pagesPrevalence of Minor Larynx Structuralanitaabreu123No ratings yet
- Pre-Auricular Abscess Due To Mycobacterium TuberculosisDocument3 pagesPre-Auricular Abscess Due To Mycobacterium Tuberculosisanitaabreu123No ratings yet
- Recurrent Epistaxis in ChildrenDocument3 pagesRecurrent Epistaxis in Childrenanitaabreu123No ratings yet
- Excision of Preauricular Sinus With Abscess Drainage in ChildrenDocument10 pagesExcision of Preauricular Sinus With Abscess Drainage in Childrenanitaabreu123No ratings yet
- Preauricular SinusDocument2 pagesPreauricular Sinusanitaabreu123No ratings yet
- Analysis of Incidence and Genetic Predisposition of Preauricular SinusDocument3 pagesAnalysis of Incidence and Genetic Predisposition of Preauricular Sinusanitaabreu123No ratings yet
- Sulcus Mucosal Slicing TecniqueDocument9 pagesSulcus Mucosal Slicing Tecniqueanitaabreu123No ratings yet
- Extrapulmonary TuberculosisDocument19 pagesExtrapulmonary Tuberculosisanitaabreu123No ratings yet
- Anosmia and Olfactory Tract Neuropathy in A Case of COVID-19Document4 pagesAnosmia and Olfactory Tract Neuropathy in A Case of COVID-19anitaabreu123No ratings yet
- Educational Value of A Preoperative CT Sinus Checklist A Resident's PerspectiveDocument3 pagesEducational Value of A Preoperative CT Sinus Checklist A Resident's Perspectiveanitaabreu123No ratings yet
- He International Frontal Sinus Anatomy Classification (IFAC) and Classification of The Extent of Endoscopic Frontal Sinus Surgery (EFSSDocument20 pagesHe International Frontal Sinus Anatomy Classification (IFAC) and Classification of The Extent of Endoscopic Frontal Sinus Surgery (EFSSanitaabreu123No ratings yet
- Single-Blinded Prospective Implementation of A Preoperative Imaging Checklist For Endoscopic Sinus Surgery.Document4 pagesSingle-Blinded Prospective Implementation of A Preoperative Imaging Checklist For Endoscopic Sinus Surgery.anitaabreu123No ratings yet
- A Useful Tool-Systematic Checklist For Evaluating Sinus Scans.Document3 pagesA Useful Tool-Systematic Checklist For Evaluating Sinus Scans.anitaabreu123No ratings yet
- Vitamin A BeneficialDocument7 pagesVitamin A Beneficialanitaabreu123No ratings yet
- Single-Blinded Prospective Implementation of A Preoperative Imaging Checklist For Endoscopic Sinus Surgery.Document4 pagesSingle-Blinded Prospective Implementation of A Preoperative Imaging Checklist For Endoscopic Sinus Surgery.anitaabreu123No ratings yet
- Educational Value of A Preoperative CT Sinus Checklist A Resident's PerspectiveDocument3 pagesEducational Value of A Preoperative CT Sinus Checklist A Resident's Perspectiveanitaabreu123No ratings yet
- The Anatomy and Function of the Pleural CavityDocument8 pagesThe Anatomy and Function of the Pleural CavityKina KinaNo ratings yet
- EASL Hepatitis C Treatment Guidelines and Risk Factors for Alcoholic Liver DiseaseDocument13 pagesEASL Hepatitis C Treatment Guidelines and Risk Factors for Alcoholic Liver DiseaseJolaine ValloNo ratings yet
- Cell Organelle Functions and City AnalogsDocument13 pagesCell Organelle Functions and City AnalogsSean GonzalezNo ratings yet
- Nephrolithiasis AnatomyDocument3 pagesNephrolithiasis AnatomyKevin Ker Campaner MerillesNo ratings yet
- Goldfinger Human Anatomy For Artists PDFDocument4 pagesGoldfinger Human Anatomy For Artists PDFSamuelNo ratings yet
- Anatomy of the PelvisDocument10 pagesAnatomy of the PelvisJISHNU TKNo ratings yet
- Small Animal Abdominal Ultrasonography - The SpleenDocument9 pagesSmall Animal Abdominal Ultrasonography - The Spleenludiegues752No ratings yet
- +1 Zoology Focus Area NotesDocument85 pages+1 Zoology Focus Area NotesKhatarnakNo ratings yet
- Staining MethodsDocument8 pagesStaining MethodsMd Arshad100% (1)
- Maternal and Child Nursing - Antepartum Practice Test With AnswersDocument6 pagesMaternal and Child Nursing - Antepartum Practice Test With Answersgelean payodNo ratings yet
- Morphology Internationaljournalplantsciences2011Document14 pagesMorphology Internationaljournalplantsciences2011wenagoNo ratings yet
- Vernix Caseosa Formation and FunctionsDocument5 pagesVernix Caseosa Formation and FunctionsPriscila FloresNo ratings yet
- PhysioPsych Assignment1Document9 pagesPhysioPsych Assignment1Tiffany ZenhoihsangNo ratings yet
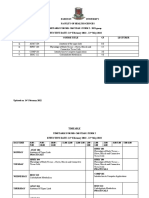
- MBCHB YEAR 1 TERM 2. 2022 (2021 Class)Document2 pagesMBCHB YEAR 1 TERM 2. 2022 (2021 Class)BedanNo ratings yet
- Micro McqsDocument1 pageMicro Mcqsmurtaza hashmiNo ratings yet
- Coordination and Control in the Human BodyDocument37 pagesCoordination and Control in the Human Bodywardah nooriNo ratings yet
- Hematology Topics Objectives References: Our Lady of Fatima University Department of Internal MedicineDocument7 pagesHematology Topics Objectives References: Our Lady of Fatima University Department of Internal MedicineAlmar NuñezNo ratings yet
- RBC MORPH UlkaDocument53 pagesRBC MORPH UlkaRushi WalgudeNo ratings yet
- Respiratory System AssignmentDocument3 pagesRespiratory System AssignmentzainaNo ratings yet
- Pelvic Pain - Sundhed - DKDocument11 pagesPelvic Pain - Sundhed - DKPavel BerlinschiNo ratings yet
- Chapter 3 Animal Tissues SolutionDocument6 pagesChapter 3 Animal Tissues SolutionLucky ErrojuNo ratings yet