Professional Documents
Culture Documents
RESORCE, Estudio de Regorafenib
Uploaded by
jesus llumpoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
RESORCE, Estudio de Regorafenib
Uploaded by
jesus llumpoCopyright:
Available Formats
Articles
Regorafenib for patients with hepatocellular carcinoma who
progressed on sorafenib treatment (RESORCE):
a randomised, double-blind, placebo-controlled, phase 3 trial
Jordi Bruix, Shukui Qin, Philippe Merle, Alessandro Granito, Yi-Hsiang Huang, György Bodoky, Marc Pracht, Osamu Yokosuka, Olivier Rosmorduc,
Valeriy Breder, René Gerolami, Gianluca Masi, Paul J Ross, Tianqiang Song, Jean-Pierre Bronowicki, Isabelle Ollivier-Hourmand, Masatoshi Kudo,
Ann-Lii Cheng, Josep M Llovet, Richard S Finn, Marie-Aude LeBerre, Annette Baumhauer, Gerold Meinhardt, Guohong Han, on behalf of the
RESORCE Investigators*
Summary
Lancet 2017; 389: 56–66 Background There are no systemic treatments for patients with hepatocellular carcinoma (HCC) whose disease
Published Online progresses during sorafenib treatment. We aimed to assess the efficacy and safety of regorafenib in patients with
December 5, 2016 HCC who have progressed during sorafenib treatment.
http://dx.doi.org/10.1016/
S0140-6736(16)32453-9
Methods In this randomised, double-blind, parallel-group, phase 3 trial done at 152 sites in 21 countries, adults with
This online publication has been
corrected. The corrected version HCC who tolerated sorafenib (≥400 mg/day for ≥20 of last 28 days of treatment), progressed on sorafenib, and had
first appeared at thelancet.com Child-Pugh A liver function were enrolled. Participants were randomly assigned (2:1) by a computer-generated
on January 5, 2017 randomisation list and interactive voice response system and stratified by geographical region, Eastern Cooperative
See Comment page 4 Oncology Group performance status, macrovascular invasion, extrahepatic disease, and α-fetoprotein level to best
*Full list of investigators can be supportive care plus oral regorafenib 160 mg or placebo once daily during weeks 1–3 of each 4-week cycle. Investigators,
found in the appendix patients, and the funder were masked to treatment assignment. The primary endpoint was overall survival (defined as
Barcelona Clinic Liver Cancer time from randomisation to death due to any cause) and analysed by intention to treat. This trial is registered with
(BCLC) Group, Liver Unit,
IDIBAPS-Hospital Clínic de
ClinicalTrials.gov, number NCT01774344.
Barcelona, CIBERehd,
Universitat de Barcelona, Findings Between May 14, 2013, and Dec 31, 2015, 843 patients were screened, of whom 573 were enrolled and
Catalonia, Spain (J Bruix MD, randomised (379 to regorafenib and 194 to placebo; population for efficacy analyses), and 567 initiated treatment
Prof J M Llovet MD); Chinese
People’s Liberation Army
(374 received regorafenib and 193 received placebo; population for safety analyses). Regorafenib improved overall
Cancer Center of Nanjing Bayi survival with a hazard ratio of 0·63 (95% CI 0·50–0·79; one-sided p<0·0001); median survival was 10·6 months
Hospital, Nanjing, China (95% CI 9·1–12·1) for regorafenib versus 7·8 months (6·3–8·8) for placebo. Adverse events were reported in all
(Prof S Qin MD); Groupement regorafenib recipients (374 [100%] of 374) and 179 (93%) of 193 placebo recipients. The most common clinically
Hospitalier Lyon Nord,
Hepatology Unit, Lyon, France
relevant grade 3 or 4 treatment-emergent events were hypertension (57 patients [15%] in the regorafenib group vs
(Prof P Merle MD); Department nine patients [5%] in the placebo group), hand–foot skin reaction (47 patients [13%] vs one [1%]), fatigue (34 patients
of Medical and Surgical [9%] vs nine patients [5%]), and diarrhoea (12 patients [3%] vs no patients). Of the 88 deaths (grade 5 adverse events)
Sciences, University of reported during the study (50 patients [13%] assigned to regorafenib and 38 [20%] assigned to placebo), seven (2%)
Bologna, S Orsola-Malpighi
Hospital, Bologna, Italy
were considered by the investigator to be related to study drug in the regorafenib group and two (1%) in the placebo
(A Granito MD); Division of group, including two patients (1%) with hepatic failure in the placebo group.
Gastroenterology and
Hepatology, Taipei Veterans Interpretation Regorafenib is the only systemic treatment shown to provide survival benefit in HCC patients
General Hospital, Institute of
Clinical Medicine, National
progressing on sorafenib treatment. Future trials should explore combinations of regorafenib with other systemic
Yang-Ming University, Taipei, agents and third-line treatments for patients who fail or who do not tolerate the sequence of sorafenib and
Taiwan (Prof Y-H Huang MD); regorafenib.
St Laszlo Teaching Hospital,
Budapest, Hungary
(G Bodoky MD); Service Funding Bayer.
d’Oncologie Médicale, Centre
Eugène Marquis, Rennes, Introduction provide a clinically significant improvement in overall
France (M Pracht MD);
The treatment of hepatocellular carcinoma (HCC) survival.4,5 Since the results with sorafenib were
Department of
Gastroenterology and follows well established guidelines.1–3 Surgical resection, published almost 10 years ago, all phase 3 trials
Nephrology, Chiba University, transplantation, and ablation are potential curative assessing novel systemic drugs have failed to improve
Chiba, Japan options for early-stage disease, whereas chemo- outcomes over sorafenib in the first-line setting6–10 or in
(Prof O Yokosuka MD);
embolisation is recommended for patients with the second-line setting following sorafenib.11–14 In
Department of Hepatology,
Hôpital de la Pitié-Salpétrière, preserved liver function and disease confined to the second-line trials in patients who have failed sorafenib,
Assistance Publique-Hôpitaux liver generally without vascular invasion. For patients overall survival in the placebo group is about
de Paris and Université Pierre who are not or who are no longer candidates for 8 months.11–14 Therefore, there is an unmet need for
et Marie Curie, Sorbonne
locoregional therapy, the oral multikinase inhibitor effective systemic therapies for HCC, particularly after
Universités, Paris, France
sorafenib is the only systemic treatment shown to treatment with sorafenib.
56 www.thelancet.com Vol 389 January 7, 2017
Articles
(Prof O Rosmorduc MD); Russian
Research in context Cancer Research Center
n.a.N.Blokhin, Moscow, Russia
Evidence before this study Similarly, none of the drugs assessed in the second-line setting (V Breder MD); CHU Timone,
We searched PubMed for articles published between Jan 1, 2008, in patients previously treated with sorafenib who stopped Université de la Méditerranée,
and Oct 26, 2016, with no language restrictions, reporting on because of disease progression or intolerance showed Marseille, France
(Prof R Gerolami MD); Azienda
the treatment of patients with advanced hepatocellular improvement over placebo. Therefore, new effective systemic
Ospedaliero-Universitaria
carcinoma (HCC) who failed sorafenib treatment using the therapies for patients with advanced HCC who fail sorafenib Pisana, Pisa, Italy (G Masi MD);
search terms (”advanced hepatocellular carcinoma” OR treatment are needed. King’s College Hospital NHS
“advanced hepatocellular cancer”) AND “sorafenib”, filtering for Foundation Trust, London, UK
Added value of this study (P J Ross FRCP); Tianjin Medical
articles describing phase 3 clinical trials. We also searched
Until now, no systemic agent has been shown to improve University Cancer Hospital,
abstracts of the annual meeting of the American Society of Tianjin, China (T Song PhD);
survival over placebo in patients with advanced HCC who fail
Clinical Oncology, using the search term “advanced INSERM 954, CHU de Nancy,
sorafenib treatment. The results of RESORCE show that Université de Lorraine, Nancy,
hepatocellular carcinoma’’, limiting the results to phase 3 trials
treatment with regorafenib resulted in a significant France (Prof J-P Bronowicki MD);
published or presented during the past 2 years. The search
improvement in overall survival compared with placebo in Service
resulted in 15 articles or abstracts, of which three were excluded d’Hépatogastroentérologie,
patients with disease progression on sorafenib. Significant
(two subanalyses and one report of maintenance sorafenib CHU, Caen, France
improvement over placebo was also shown for the secondary (I Ollivier-Hourmand MD);
therapy following the combination of transcatheter arterial
endpoints of progression-free survival, time to progression, Kindai University Faculty of
chemoembolisation and radiotherapy). Of the remaining Medicine, Osaka, Japan
disease control, and overall tumour response.
12 publications, two were reports of the pivotal trials of (Prof M Kudo MD); Department
sorafenib for advanced HCC; five reported the first-line use of a Implications of all the available evidence of Medical Oncology, National
novel drug or the novel combination of a drug with sorafenib Taiwan University Hospital,
This phase 3 trial of regorafenib is the first to show an overall
Taipei, Taiwan
compared with a sorafenib control; and five reported the survival benefit compared with placebo in patients who failed (Prof A-L Cheng MD); Liver
second-line use of a novel agent in patients who had failed sorafenib treatment. Future trials should explore combinations Cancer Program, Division of
sorafenib. None of the trials assessing novel agents or novel of regorafenib with other systemic agents and third-line Liver Diseases, Tisch Cancer
Institute, Department of
combinations of agents in the first-line setting met the primary treatments for patients who fail or who do not tolerate the
Medicine, Icahn School of
endpoint to show improved overall survival over sorafenib. sequence of sorafenib and regorafenib. Medicine at Mount Sinai,
New York, NY, USA
(Prof J M Llovet MD); Institució
Regorafenib is an oral multikinase inhibitor that blocks stage B or C,23 could not benefit from resection, local Catalana de Recerca i Estudis
Avançats (ICREA), Barcelona,
the activity of protein kinases involved in angiogenesis, ablation, or chemoembolisation, and must have had
Spain (Prof J M Llovet);
oncogenesis, metastasis, and tumour immunity.15,16 It has documented radiological progression during sorafenib Department of Medicine,
a distinct molecular target profile and had more potent treatment as defined in a study-specific radiology charter. Division of Hematology/
pharmacological activity than sorafenib in preclinical They must have tolerated sorafenib (≥400 mg daily for at Oncology, David Geffen School
of Medicine at UCLA, Los
studies.15,17 Regorafenib is approved as monotherapy for least 20 of the 28 days before discontinuation) and
Angeles, CA, USA (R S Finn MD);
the treatment of treatment-refractory metastatic received their last sorafenib dose within 10 weeks of Bayer HealthCare SAS, Loos,
colorectal cancer and gastrointestinal stromal tumours at randomisation. They were required to have Child-Pugh A France (M-A LeBerre MSc);
a dose of 160 mg once daily for the first 3 weeks of each liver function. Patients were excluded if they had received Bayer Pharmaceuticals, Bayer
Vital GmbH, Leverkusen,
4-week cycle.18–20 Based on results of a single-arm phase 2 any other previous systemic treatment for HCC or if they Germany (A Baumhauer MD);
study showing antitumour activity and acceptable discontinued sorafenib for toxicity (see appendix pp 5–7 Bayer HealthCare
tolerability,21 we aimed to assess the efficacy and safety of for full inclusion and exclusion criteria). Pharmaceuticals, Whippany,
regorafenib in patients with HCC who progressed during All patients provided written informed consent. The NJ, USA (G Meinhardt MD); and
The First Affiliated Hospital
sorafenib treatment. trial was approved by each centre’s ethics committee or (Xijing Hospital) of the Fourth
institutional review board and complied with Good Military Medical University,
Methods Clinical Practice guidelines, the Declaration of Helsinki, Xi’an, China (Prof G Han MD)
Study design and participants and applicable local laws. Correspondence to:
This randomised, double-blind, placebo-controlled Dr Jordi Bruix, BCLC Group, Liver
Unit, Hospital Clinic, University of
international phase 3 trial was done at 152 centres in Randomisation and masking Barcelona, IDIBAPS, CIBEREHD,
21 countries in North America, South America, Europe, Patients were randomly assigned (2:1) to regorafenib or Villarroel 170, Barcelona 08036,
Asia, and Australia. placebo using a computer-generated randomisation list Spain
Eligible patients were adults with HCC confirmed by prepared by the funder. Randomisation was stratified by jbruix@clinic.ub.es
pathological assessment or non-invasive assessment geographical region (Asia vs rest of world), macrovascular
according to the American Association for the Study of invasion (yes vs no), extrahepatic disease (yes vs no), See Online for appendix
Liver Diseases criteria for patients with confirmed α-fetoprotein concentration (<400 ng/mL vs ≥400 ng/mL),
cirrhosis,1 and had to have at least one measurable lesion and Eastern Cooperative Oncology Group (ECOG)
by modified Response Evaluation Criteria in Solid performance status (0 vs 1). The proportion of patients
Tumors for HCC (mRECIST)22 and RECIST version 1.1. recruited from Asia was limited to 40%. Investigators,
Patients were Barcelona Clinic Liver Cancer (BCLC) patients, and the funder were masked to treatment
www.thelancet.com Vol 389 January 7, 2017 57
Articles
assignment. The randomisation number for each patient cycles and every 12 weeks thereafter during treatment.
was assigned based on information obtained from the Treatment could be continued beyond progression if the
interactive voice-response system. Tablets with identical investigator judged that the patient would benefit from
appearance were used for regorafenib and placebo. continued treatment. Patients assigned to placebo could
receive regorafenib after the primary analysis.
Procedures Treatment interruptions and dose reductions (to
Patients received 160 mg regorafenib (four 40 mg tablets) 120 mg, then 80 mg) were allowed to manage toxicity
orally or matching placebo once daily for the first 3 weeks (appendix pp 12–15). The regorafenib dose could be re-
of each 4-week cycle. All patients received best supportive escalated to a maximum of 160 mg at the investigator’s
care. Other investigational antitumour drugs, discretion once toxicities were resolved. If further dose
antineoplastic chemotherapy, hormonal therapy, or reduction was required, treatment was discontinued.
immunotherapy were not allowed. Treatment continued
until disease progression as defined by mRECIST, Outcomes
clinical progression (defined as an ECOG performance The primary endpoint was overall survival (time from
score ≥3 or symptomatic deterioration, including randomisation to death due to any cause), analysed by
increased liver function tests), death, unacceptable intention to treat (ITT). Secondary efficacy endpoints were
toxicity, withdrawal of consent by the patient, or decision progression-free survival (randomisation to radiological or
by the treating physician that discontinuation would be clinical disease progression or death; by ITT), time to
in the patient’s best interest. Patients were followed up progression (randomisation to radiological or clinical
for tumour assessments every 6 weeks for the first eight disease progression; by ITT), objective response rate
(patients with complete or partial response), and disease
843 patients assessed for eligibility
control rate (patients with complete response, partial
response, or stable disease maintained for ≥6 weeks),
assessed by investigators using mRECIST22 and RECIST 1.1
270 ineligible, primary reason (appendix p 7).
238 screen failure
22 withdrawal by patient Health-related quality of life (HRQoL) was a
7 adverse event teritiary outcome assessed using the Functional
2 death
Assessment of Cancer Therapy (FACT)–General
1 therapeutic procedure required
(FACT-G), FACT–Hepatobiliary (FACT-Hep), EQ-5D,
and EQ-VAS questionnaires.24,25 The following tertiary
573 randomised endpoints are not reported here: pharmacokinetics of
regorafenib, and biomarker evaluation. Safety was
assessed by adverse events, laboratory abnormalities,
vital signs, and electrocardiography. Safety was
379 assigned to regorafenib 194 assigned to placebo
374 received regorafenib 193 received placebo monitored continuously throughout the study, and
5 did not receive regorafenib 1 did not receive placebo patients underwent safety evaluations at every cycle.
Concentrations of alanine aminotransferase (ALT),
309 discontinued treatment, primary reason 183 discontinued treatment, primary reason aspartate aminotransferase (AST), and bilirubin were
149 progressive disease, radiological 119 progressive disease, radiological assessed weekly during the first two cycles. Adverse
progression progression
21 progressive disease, clinical 14 progressive disease, clinical
events were graded using National Cancer Institute
progression progression Common Terminology Criteria for Adverse Events
56 adverse event associated with 1 progressive disease* (NCI-CTCAE) version 4.03 (appendix p 7 for further
disease progression 28 adverse event associated with
47 adverse event not associated with disease progression assessments) and seriousness of adverse events was
disease progression 12 adverse event not associated with recorded. Investigators were blinded to study treatment
1 adverse event disease progression
5 death 3 protocol violation
for assessment of whether a death was considered
26 withdrawal by patient 5 withdrawal by patient related to study drug.
2 non-compliance with study drug 1 other
1 physician decision
1 protocol violation Statistical analysis
Using a per-protocol one-sided α of 0·025, a
2:1 randomisation between regorafenib and placebo, and
65 treatment ongoing 10 treatment ongoing
assuming a median overall survival of 8 months in the
placebo group, the study would have 90% power to detect
379 included in intention-to-treat analysis 194 included in intention-to-treat analysis a 43% increase in overall survival with regorafenib
(assumed median survival 11·4 months) compared with
Figure 1: Trial profile placebo at 370 deaths and requiring 560 patients. For the
*Patient had radiological progression but continued treatment, and terminated treatment when the investigator primary efficacy endpoint of overall survival, the groups
judged that the patient was no longer experiencing clinical benefit. were compared using a log-rank test, stratified by the
58 www.thelancet.com Vol 389 January 7, 2017
Articles
Regorafenib Placebo Regorafenib Placebo
(n=379) (n=194) (n=379) (n=194)
Sex (Continued from previous column)
Male 333 (88%) 171 (88%) Liver cirrhosis (investigator
285 (75%) 144 (74%)
assessed)
Female 46 (12%) 23 (12%)
Aetiology of HCC§
Age, years 64 (54–71) 62 (55–68)
Hepatitis B 143 (38%) 73 (38%)
Race
Alcohol use 90 (24%) 55 (28%)
White 138 (36%) 68 (35%)
Hepatitis C 78 (21%) 41 (21%)
Asian 156 (41%) 78 (40%)
Unknown 66 (17%) 32 (16%)
Black 6 (2%) 2 (1%)
Non-alcoholic
Other/not reported 79 (21%) 46 (24%) 25 (7%) 13 (7%)
steatohepatitis
Geographical region Other 28 (7%) 10 (5%)
Rest of world 236 (62%) 121 (62%) Number of target lesions (mRECIST)¶
Asia* 143 (38%) 73 (38%) 1 67 (18%) 31 (16%)
ECOG performance status 2 175 (46%) 88 (45%)
0 247 (65%) 130 (67%) 3 68 (18%) 37 (19%)
1 132 (35%) 64 (33%) 4 43 (11%) 26 (13%)
Macrovascular invasion 110 (29%) 54 (28%) 5 19 (5%) 12 (6%)
Extrahepatic disease 265 (70%) 147 (76%) Time from initial HCC
Macrovascular invasion and/or diagnosis to start of study
304 (80%) 162 (84%) treatment, months
extrahepatic disease
Lung, target lesion† 98 (26%) 48 (25%) Median (IQR) 21 (11–38) 20 (12–32)
Lymph node, target lesion† 58 (15%) 36 (19%) Mean (SD) 29 (28) 27 (22)
Lung, non-target lesion† 121 (32%) 57 (29%) Duration of sorafenib
7·8 (4·2–14·5) 7·8 (4·4–14·7)
treatment, months
Lymph node, non-target
61 (16%) 29 (15%) Time from progression on
lesion†
sorafenib to start of study 1·4 (0·9–2·3) 1·4 (0·9–2·2)
Pattern of progression on previous sorafenib treatment treatment, months
New extrahepatic lesion 153 (40%) 80 (41%) Time from discontinuation of
New intrahepatic lesion 168 (44%) 88 (45%) sorafenib to start of study 0·9 (0·7–1·3) 0·9 (0·7–1·3)
treatment, months
Growth of intrahepatic or
307 (81%) 156 (80%)
extrahepatic lesions, or both Data are n (%) or median (IQR), unless otherwise specified. BCLC=Barcelona Clinic
α-fetoprotein ≥400 ng/mL 162 (43%) 87 (45%) Liver Cancer. ECOG=Eastern Cooperative Oncology Group. HCC=hepatocellular
carcinoma. mRECIST=modified RECIST for HCC. *Includes patients from China, Japan,
Child-Pugh class‡
South Korea, Singapore, and Taiwan. †RECIST version 1.1. ‡The Child-Pugh system
A 373 (98%) 188 (97%) describes liver disease severity: patients are divided into classes from A to C, with class
C representing the worst prognosis. Child-Pugh class was missing in one patient in
B 5 (1%) 6 (3%)
the regorafenib group. Those patients who progressed to Child-Pugh B after
BCLC stage screening and before randomisation were included. §Patients could have more than
A (early) 1 (<1%) 0 one aetiology of HCC. ¶n=372 in the regorafenib group.
B (intermediate) 53 (14%) 22 (11%) Table 1: Baseline characteristics (efficacy population)
C (advanced) 325 (86%) 172 (89%)
(Table 1 continues in next column)
For HRQoL assessments, an analysis-of-covariance
model was used to compare the time-adjusted area under
aforementioned randomisation factors. The hazard ratio the curve (AUC) between groups with covariates for
(HR) for overall survival and its 95% CI were calculated baseline scores and stratification factors. The least-squares
using the stratified Cox model. An interim futility mean (LSM) with 95% CI was estimated for each
analysis was done after 30% of the events had occurred; treatment group and for the difference between groups.
futility boundaries were not crossed. For analyses of time Data were analysed with SAS, version 9.2 (SAS Institute
to progression and progression-free survival, groups Inc, Cary, NC, USA). The primary analysis was by
were compared using a log-rank test stratified by the intention to treat; safety analyses included all patients
factors used in the analyses of the primary endpoint. The who received at least one dose of study drug. The study
response rates and disease control rates in the two groups was overseen by a data safety monitoring committee.
were compared using the Cochran–Mantel–Haenszel This trial is registered with ClinicalTrials.gov, number
test, with adjustment for the stratification factors. NCT01774344.
www.thelancet.com Vol 389 January 7, 2017 59
Articles
Role of the funding source report and approved the submission for publication, had
The funder (Bayer) provided the study drug and worked full access to the data, and vouch for the completeness
with the principal investigator (JB) and the study steering and accuracy of the data and adherence of the study to
committee to design the study. Data collection and the protocol. The funder funded writing assistance.
interpretation, and preparation of this report, were done
by the investigators and the funder. Statistical analyses Results
were performed by the funder. All authors reviewed this Between May 14, 2013, and Dec 31, 2015, 843 patients were
screened, of whom 573 were enrolled and randomised
A (379 to regorafenib and 194 to placebo; population for
100 Regorafenib efficacy analyses; figure 1). 216 patients (38%) were from
Placebo Asia. Overall, 567 patients (99%) started treatment (374 in
90
80 the regorafenib group and 193 in the placebo group) and
Probability of survival (%)
70 comprise the safety analysis population. Treatment groups
60 were similar with respect to baseline demographics,
50 tumour burden, ECOG performance status, aetiology, and
40 severity of liver disease (table 1). We also assessed the
30 pattern of progression during sorafenib treatment because
20 this parameter has been shown to influence outcomes
10 and could distort the results of second-line studies.26 A
HR 0·63 (95% CI 0·50–0·79); one-sided p<0·0001
0 potential imbalance in the pattern of progression on
0 3 6 9 12 15 18 21 24 27 30 33 previous sorafenib was ruled out because the distribution
Number at risk
Regorafenib 379 316 224 170 122 78 54 34 21 10 4 0 of the different categories was similar across the treatment
Placebo 194 149 95 62 37 26 16 8 5 3 1 0 groups. Specifically, the development of new extrahepatic
sites during previous sorafenib, which was recently shown
B
100
to be associated with a worse prognosis,26 was present in
153 (40%) patients in the regorafenib group and 80 (41%)
Probability of progression-free survival (%)
90
80
in the placebo group. Similarly, growth of existing lesions
70
(intrahepatic or extrahepatic; 307 [81%] patients in the
60
regorafenib group and 156 [80%] patients in the placebo
50
group) or new intrahepatic sites (168 [44%] patients in the
regorafenib group and 88 [45%] patients in the placebo
40
group) were balanced between treatment groups.
30
Median time on sorafenib was 7·8 months
20
HR 0·46 (95% CI 0·37–0·56); one-sided p<0·0001 (IQR 4·2–14·5) in the regorafenib group and 7·8 months
10
(4·4–14·7) in the placebo group. Median time from
0
0 3 6 9 12 15 18 21 24 27 30 33 progression on sorafenib was similar in both groups
Number at risk (1·4 months [IQR 0·9–2·3] in the regorafenib group
Regorafenib 379 166 76 43 27 14 8 7 4 0 0 0
Placebo 194 37 15 6 3 2 1 1 0 0 0 0 vs 1·4 months [0·9–2·2] in the placebo group), as was the
median time from discontinuation of sorafenib to the
C start of study treatment (0·9 months [IQR 0·7–1·3] in
100
both groups).
90
Of patients who started treatment, 309 (83%) receiving
80
Probability of progression (%)
regorafenib and 183 (95%) receiving placebo discontinued
70
study treatment (figure 1). The most common reason for
60
discontinuation was disease progression (226 [60%] in
50
the regorafenib group and 162 [84%] in the placebo
40 group). Median treatment duration was 3·6 months
30 (IQR 1·6–7·6) with regorafenib and 1·9 months
20 (1·4–3·9) with placebo; mean durations were 5·9 months
10 (SD 6·0) and 3·3 months (3·9), respectively. Mean daily
HR 0·44 (95% CI 0·36–0·55); one-sided p<0·0001
0 dose of regorafenib was 144·1 mg (SD 21·3) and of
0 3 6 9 12 15 18 21 24 27 30 33
Months from randomisation placebo was 157·4 mg (10·3). Excluding treatment delays
Number at risk
Regorafenib 379 164 75 41 27 14 8 7 4 0 0 0 or interruptions, almost half of the regorafenib group
Placebo 194 36 15 6 3 2 1 1 0 0 0 0 (184 [49%] of 374]) received the full protocol dose
(160 mg/day) with no reductions.
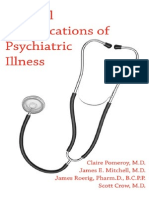
Figure 2: Kaplan-Meier analysis of overall survival (A), progression-free survival (mRECIST; B), and time to
progression (mRECIST; C) At the cutoff date for the final analysis (Feb 29, 2016) and
mRECIST=modified RECIST for hepatocellular carcinoma. a median follow-up of 7·0 months (IQR 3·7–12·6),
60 www.thelancet.com Vol 389 January 7, 2017
Articles
A n/events Hazard ratio
(95% CI)
Age group
<65 years 315/205 0·65 (0·49–0·87)
≥65 years 258/168 0·74 (0·54–1·02)
Sex
Male 504/327 0·65 (0·52–0·82)
Female 69/46 0·88 (0·48–1·62)
Geographical region
Asia 216/142 0·65 (0·46–0·92)
Rest of world 357/231 0·68 (0·52–0·90)
ECOG score
0 377/231 0·61 (0·47–0·80)
1 196/142 0·78 (0·55–1·11)
AFP
<400 ng/mL 324/194 0·67 (0·50–0·90)
≥400 ng/mL 249/179 0·68 (0·50–0·92)
Child-Pugh score
A5 362/222 0·60 (0·46–0·79)
A6 199/141 0·80 (0·57–1·13)
Extrahepatic disease
No 161/103 0·97 (0·63–1·48)
Yes 412/270 0·60 (0·47–0·77)
Macrovascular invasion
No 409/259 0·67 (0·52–0·86)
Yes 164/114 0·67 (0·46–0·98)
Extrahepatic disease, or macrovascular invasion, or both
No 107/68 0·98 (0·58–1·66)
Yes 466/305 0·63 (0·50–0·79)
Hepatitis B
No 357/238 0·73 (0·56–0·95)
Yes 216/135 0·58 (0·41–0·82)
Hepatitis C
No 454/295 0·65 (0·51–0·82)
Yes 119/78 0·79 (0·49–1·26)
Alcohol use
No 428/273 0·59 (0·46–0·76)
Yes 145/100 0·92 (0·61–1·38)
B
Age group
<65 years 315/267 0·46 (0·36–0·59)
≥65 years 258/207 0·51 (0·38–0·68)
Sex
Male 504/414 0·47 (0·39–0·58)
Female 69/60 0·55 (0·32–0·96)
Geographical region
Asia 216/180 0·34 (0·25–0·47)
Rest of world 357/294 0·54 (0·43–0·69)
ECOG score
0 377/310 0·43 (0·34–0·54)
1 196/164 0·62 (0·45–0·86)
AFP
<400 ng/mL 324/262 0·45 (0·35–0·58)
≥400 ng/mL 249/212 0·53 (0·40–0·70)
Child-Pugh score
A5 362/295 0·44 (0·34–0·56)
A6 199/170 0·56 (0·41–0·76)
Extrahepatic disease
No 161/127 0·52 (0·36–0·75)
Yes 412/347 0·47 (0·38–0·59)
Macrovascular invasion
No 409/341 0·45 (0·36–0·56)
Yes 164/133 0·55 (0·38–0·78)
Extrahepatic disease, or macrovascular invasion, or both
No 107/89 0·47 (0·30–0·73)
Yes 466/385 0·49 (0·39–0·60)
Hepatitis B
No 357/300 0·53 (0·41–0·67)
Yes 216/174 0·39 (0·29–0·54)
Hepatitis C
No 454/373 0·46 (0·37–0·57)
Yes 119/101 0·59 (0·39–0·90)
Alcohol use
No 428/354 0·46 (0·37–0·57)
Yes 145/120 0·53 (0·37–0·77)
0 0·5 1·0 1·5 2·0
Favours regorafenib Favours placebo
(Figure 3 continues on next page)
www.thelancet.com Vol 389 January 7, 2017 61
Articles
(Figure continued from previous page)
C n/events Hazard ratio
(95% CI)
Age group
<65 years 315/252 0·45 (0·35–0·58)
≥65 years 258/195 0·50 (0·37–0·68)
Sex
Male 504/390 0·47 (0·38–0·57)
Female 69/57 0·53 (0·30–0·93)
Geographical region
Asia 216/170 0·34 (0·24–0·47)
Rest of world 357/277 0·53 (0·41–0·67)
ECOG score
0 377/293 0·42 (0·33–0·54)
1 196/154 0·61 (0·44–0·84)
AFP
<400 ng/mL 324/248 0·43 (0·33–0·56)
≥400 ng/mL 249/199 0·53 (0·40–0·71)
Child-Pugh score
A5 362/282 0·43 (0·34–0·56)
A6 199/158 0·51 (0·37–0·71)
Extrahepatic disease
No 161/122 0·51 (0·35–0·74)
Yes 412/325 0·46 (0·37–0·58)
Macrovascular invasion
No 409/321 0·45 (0·35–0·56)
Yes 164/126 0·52 (0·36–0·75)
Extrahepatic disease, or macrovascular invasion, or both
No 107/84 0·46 (0·29–0·73)
Yes 466/363 0·48 (0·38–0·59)
Hepatitis B
No 357/284 0·51 (0·40–0·65)
Yes 216/163 0·38 (0·28–0·53)
Hepatitis C
No 454/351 0·45 (0·36–0·56)
Yes 119/96 0·57 (0·37–0·87)
Alcohol use
No 428/334 0·45 (0·36–0·56)
Yes 145/113 0·51 (0·35–0·75)
0 0·5 1·0 1·5 2·0
Favours regorafenib Favours placebo
Figure 3: Overall survival (A), progression-free survival (mRECIST; B), and time to progression (mRECIST; C) in selected subgroups
AFP=α-fetoprotein. ECOG=Eastern Cooperative Oncology Group. mRECIST=modified RECIST.
373 (65%) of the 573 randomised patients had died regorafenib group versus eight patients (4% [2–8]) in the
(233 [61%] of 379 in the regorafenib group and 140 [72%] of placebo group had a partial response by mRECIST as
194 in the placebo group). Median overall survival was assessed by investigators (table 2). 40 (11%) of 379 patients
10·6 months (95% CI 9·1–12·1) with regorafenib and in the regorafenib group versus eight (4%) of 194 patients
7·8 months (6·3–8·8) with placebo (HR 0·63 [95% CI in the placebo group achieved an objective response
0·50–0·79]; one-sided p<0·0001; figure 2A). The (p=0·0047). 247 (65%) of 379 patients in the regorafenib
improvement in overall survival with regorafenib was group versus 70 (36%) of 194 patients in the placebo
maintained in all preplanned subgroup analyses group achieved disease control (p<0·0001). A significant
(figure 3A; appendix p 16). improvement in tumour response and disease control
Median progression-free survival by mRECIST was was also shown using RECIST 1.1 (appendix p 16).
3·1 months (95% CI 2·8–4·2) with regorafenib and Tumour shrinkage (any decrease in the sum of diameters
1·5 months (1·4–1·6) with placebo (figure 2B). Median of target lesions) was reported in 49% (184/379) of
time to progression by mRECIST was 3·2 months patients in the regorafenib group and 23% (44/194) of
(95% CI 2·9–4·2) with regorafenib and 1·5 months patients in the placebo group (appendix p 17). Duration
(1·4–1·6) with placebo (figure 2C). Predefined subgroup of response and duration of stable disease are reported in
analysis for progression-free survival and time to the appendix (p 17).
progression also showed a consistent benefit All (374/374) patients who received regorafenib and
(figures 3B,C). The HRs for progression-free survival and 179 (93%) of 193 patients who received placebo had at least
time to progression assessed by RECIST 1.1 were one treatment-emergent adverse event; these were deemed
comparable (appendix pp 8–11). possibly study-drug related in 346 (93%) patients who
Two patients (1% [95% CI <1–2]) in the regorafenib received regorafenib and 100 (52%) patients who received
group versus no patients in the placebo group had a placebo (table 3). The most common clinically relevant
complete response and 38 patients (10% [7–14]) in the grade 3 or 4 events were hypertension (57 patients [15%] in
62 www.thelancet.com Vol 389 January 7, 2017
Articles
193 patients in the placebo group), hand–foot skin reaction
Regorafenib Placebo (n=194)
(n=379) (seven [2%] vs none), and ALT increase (four [1%] vs none).
No clinically meaningful differences were noted
Best overall response*
between the regorafenib and placebo groups in HRQoL.
Complete response 2 (1%; <1–2) 0
Overall changes from baseline in EQ-5D and FACT-Hep
Partial response 38 (10%; 7–14) 8 (4%; 2–8)
were similar in the two groups. In the LSM time-adjusted
Stable disease 206 (54%; 49–59) 62 (32%; 26–39)
AUC analysis of the EQ-5D and FACT-Hep, the scores
Non-complete response/ 1 (<1%; 0–2) 0
non-progressive disease
were lower in the regorafenib group than in the placebo
Progressive disease 86 (23%; 19–27) 108 (56%; 48–63)
group, and specifically the scores of the FACT-Hep Total
and Trial Outcome Index (a subscale of the FACT-Hep)
Not evaluable 19 (5%; 3–8) 8 (4%; 2–8)]
were statistically lower in the regorafenib group than in
Not assessed 27 (7%; 5–10) 8 (4%; 2–8)
the placebo group (p=0·0006 and p<0·0001, respectively);
Clinical progression† 86 (23%; 19–27) 40 (21%; 15–27)
however, minimally important thresholds for the
Objective response 40 (11%)‡ 8 (4%)‡
(complete response + partial differences as established in the literature were not met
response)* (appendix p 19).24,25
Disease control* 247 (65%)§ 70 (36%)§
Discussion
Data are n (%; 95% CI). *Based on radiological review using modified Response
Evaluation Criteria in Solid Tumors for HCC (mRECIST).22 †Defined as worsening of
Our study shows that regorafenib provides a significant
ECOG performance status or symptomatic deterioration including increase in liver and clinically meaningful improvement in overall
function tests. ‡One-sided p=0·0047. §One-sided p<0·0001. survival in patients with HCC progressing during
Table 2: Tumour response (efficacy population)
sorafenib treatment. This finding was associated with an
increase in median survival from 7·8 months to
10·6 months. This survival benefit was maintained in the
the regorafenib group vs nine patients [5%] in the placebo prespecified subgroup analyses, including geographical
group), hand–foot skin reaction (47 patients [13%] vs region and aetiology, and was accompanied by significant
one [1%]), fatigue (34 patients [9%] vs nine patients [5%]), improvements in progression-free survival, time to
and diarrhoea (12 patients [3%] vs no patients). The progression, and objective response, and disease control
frequency of hepatobiliary disorders was higher with rate. Two patients treated with regorafenib had a
placebo (18% [34/193]) than with regorafenib (11% complete tumour response by mRECIST, which excludes
[40/374]). Serious adverse events occurred in 166 (44%) necrosis of the target lesion from the tumour
patients assigned to regorafenib and 90 (47%) patients measurement. These responses would also have been
assigned to placebo and were attributed to study drug in classified as complete using conventional European
39 (10%) patients assigned to regorafenib and five (3%) Association for the Study of the Liver criteria.27
patients assigned to placebo. Of the 88 deaths (grade 5 Interestingly, we noted similar outcomes using
adverse events) reported during the study (50 patients mRECIST and RECIST 1.1 for progression-free survival
[13%] assigned to regorafenib and 38 [20%] assigned to and time to progression.
placebo), seven (2%) were considered by the investigator to The survival of the placebo group in our study is
be related to study drug in the regorafenib arm and two consistent with previous second-line studies in HCC at
(1%) in the placebo arm, including two patients (1%) with about 8 months.11–14 Use of five stratification factors
hepatic failure in the placebo group (appendix p 18). ensured that the trial groups were fully balanced for
21 (6%) of 374 patients in the regorafenib group had commonly assessed patient and disease characteristics;
grade 3 or higher treatment-emergent bleeding events however, we also analysed the distribution of patients
versus 15 (8%) of 193 patients in the placebo group across treatment groups according to the pattern of
(appendix p 18). 255 (68%) of 374 patients in the regorafenib progression under sorafenib. Pattern of progression has
group had interruptions or dose reductions due to adverse recently been found to be a major factor affecting
events versus 60 (31%) of 193 patients in the placebo group. outcome and potentially confounding study results if not
Similarly, 93 (25%) of 374 patients in the regorafenib group balanced across study groups.26 Although new
discontinued due to adverse events versus 37 (19%) of intrahepatic sites or growth of known tumour lesions
193 patients in the placebo group. Drug-related adverse have been shown to have a moderate effect on post-
events led to interruptions or dose reductions in 202 (54%) progression survival, the development of new vascular
patients in the regorafenib group and 20 (10%) patients in invasion or extrahepatic spread is a significant predictor
the placebo group, and to discontinuations in 39 (10%) of a worse survival.26 Pattern of progression under
patients in the regorafenib group and seven (4%) patients previous sorafenib was balanced in this study.
in the placebo group. The most common adverse events All primary and secondary efficacy outcomes in this
leading to discontinuation more frequently with sorafenib pretreated population seem numerically better
regorafenib were increase in AST concentration (eight [2%] than those with sorafenib in the first-line setting.4,5 This
of 374 patients in the regorafenib group vs three [2%] of might be because regorafenib is more pharmacologically
www.thelancet.com Vol 389 January 7, 2017 63
Articles
Treatment-emergent Treatment-emergent drug-related
Regorafenib (n=374) Placebo (n=193) Regorafenib (n=374) Placebo (n=193)
Any grade Grade 3 Grade 4 Any grade Grade 3 Grade 4 Any grade Grade 3 Grade 4 Any grade Grade 3 Grade 4
Any adverse event 374 (100%) 208 (56%) 40 (11%) 179 (93%) 61 (32%) 14 (7%) 346 (93%) 173 (46%) 14 (4%) 100 (52%) 31 (16%) 1 (1%)
Hand–foot skin reaction 198 (53%) 47 (13%) NA 15 (8%) 1 (1%) NA 196 (52%) 47 (13%) NA 13 (7%) 1 (1%) NA
Diarrhoea 155 (41%) 12 (3%) 0 29 (15%) 0 0 125 (33%) 9 (2%) 0 18 (9%) 0 0
Fatigue 151 (40%) 34 (9%) NA 61 (32%) 9 (5%) NA 110 (29%) 24 (6%) NA 37 (19%) 3 (2%) NA
Hypertension 116 (31%) 56 (15%) 1 (<1%) 12 (6%) 9 (5%) 0 87 (23%) 48 (13%) 1 (<1%) 9 (5%) 6 (3%) 0
Anorexia 116 (31%) 10 (3%) 0 28 (15%) 4 (2%) 0 88 (24%) 10 (3%) 0 12 (6%) 0 0
Increased blood bilirubin 108 (29%) 37 (10%) 2 (1%) 34 (18%) 15 (8%) 6 (3%) 70 (19%) 24 (6%) 1 (<1%) 7 (4%) 4 (2%) 0
Abdominal pain 105 (28%) 13 (3%) NA 43 (22%) 8 (4%) NA 34 (9%) 5 (1%) NA 5 (3%) 0 NA
Increased AST 92 (25%) 37 (10%) 4 (1%) 38 (20%) 19 (10%) 3 (2%) 48 (13%) 16 (4%) 3 (1%) 15 (8%) 9 (5%) 1 (1%)
Fever 72 (19%) 0 0 14 (7%) 0 0 14 (4%) 0 0 4 (2%) 0 0
Nausea 64 (17%) 2 (1%) NA 26 (13%) 0 NA 40 (11%) 1 (<1%) NA 13 (7%) 0 NA
Constipation 65 (17%) 1 (<1%) 0 22 (11%) 1 (1%) 0 24 (6%) 0 0 3 (2%) 0 0
Ascites 58 (16%) 16 (4%) 0 31 (16%) 11 (6%) 0 8 (2%) 3 (1%) 0 1 (1%) 1 (1%) 0
Anaemia 58 (16%) 16 (4%) 2 (1%) 22 (11%) 10 (5%) 1 (1%) 23 (6%) 5 (1%) 1 (<1%) 2 (1%) 1 (1%) 0
Limb oedema 60 (16%) 2 (1%) NA 24 (12%) 0 NA 12 (3%) 1 (<1%) NA 1 (1%) 0 NA
Increased ALT 55 (15%) 10 (3%) 2 (1%) 22 (11%) 5 (3%) 0 29 (8%) 6 (2%) 2 (1%) 8 (4%) 2 (1%) 0
Hypoalbuminaemia 57 (15%) 6 (2%) 0 16 (8%) 1 (1%) 0 9 (2%) 2 (1%) 0 0 0 0
General disorders and 53 (14%) 16 (4%) 2 (1%) 29 (15%) 6 (3%) 3 (2%) 8 (2%) 5 (1%) 0 2 (1%) 1 (1%) 0
administration site
conditions, other
Weight loss 51 (14%) 7 (2%) NA 9 (5%) 0 NA 27 (7%) 4 (1%) NA 3 (2%) 0 NA
Oral mucositis 47 (13%) 4 (1%) 0 6 (3%) 1 (1%) 0 42 (11%) 4 (1%) 0 5 (3%) 1 (1%) 0
Vomiting 47 (13%) 3 (1%) 0 13 (7%) 1 (1%) 0 27 (7%) 1 (<1%) 0 5 (3%) 0 0
Investigations, other 40 (11%) 4 (1%) 0 11 (6%) 1 (1%) 0 18 (5%) 1 (<1%) 0 0 0 0
Back pain 42 (11%) 6 (2%) 1 (<1%) 17 (9%) 2 (1%) 0 2 (1%) 1 (<1%) 0 2 (1%) 0 0
Thrombocytopenia 39 (10%) 13 (3%) 1 (<1%) 5 (3%) 0 0 19 (5%) 7 (2%) 1 (<1%) 2 (1%) 0 0
Cough 40 (11%) 1 (<1%) NA 14 (7%) 0 NA 4 (1%) 0 NA 2 (1%) 0 NA
Hypophosphataemia 37 (10%) 30 (8%) 2 (1%) 4 (2%) 3 (2%) 0 22 (6%) 16 (4%) 2 (1%) 2 (1%) 1 (1%) 0
Hoarseness 39 (10%) 0 NA 1 (1%) 0 NA 34 (9%) 0 NA 0 0 NA
Data are n (%). Adverse events were graded using NCI-CTCAE version 4.03. ALT=alanine aminotransferase. AST=aspartate aminotransferase. NA=not applicable. NCI-CTCAE=National Cancer Institute Common
Terminology Criteria for Adverse Events. *Events listed are treatment-emergent adverse events occurring in at least 10% of patients in either treatment group.
Table 3: Treatment-emergent adverse events and treatment-emergent drug-related adverse events* (safety population)
active than is sorafenib,15 and could also be because This study was designed to assess a new systemic
tolerability to regorafenib was improved for patients treatment for patients with HCC progressing on first-
tolerant to sorafenib due to the somewhat overlapping line therapy and incorporated lessons from previous
adverse-event profiles of the two drugs. As multikinase phase 3 trials that failed to meet their primary endpoint.6–14
inhibitors, the antitumour activity of regorafenib and Only patients with Child-Pugh A liver function were
sorafenib could extend beyond their antiangiogenic included to avoid the potential confounding effect of
properties to a direct effect on tumour and stromal cells impaired liver function on survival. To ensure that
that modulate inflammatory and immune processes.28 treatment groups were balanced with respect to relevant
Recent phase 3 trials in HCC assessing multikinase prognostic factors, randomisation was stratified by
inhibitors having profiles that partly overlap with α-fetoprotein concentrations and ECOG performance
regorafenib have failed to improve outcomes over status. However, unlike in previous studies,4,11
sorafenib or versus placebo after sorafenib.6–8,11 The macrovascular invasion and extrahepatic disease were
results of this study suggest that the sequential use of separate stratification factors. We also stratified for
two multikinase inhibitors with partly overlapping target geographical region because of differences in access to
profiles provides a survival benefit in HCC. Regorafenib cancer care and the use of locoregional therapies.
has been shown to improve survival in patients with Although the trial was not stratified for aetiology,
gastrointestinal stromal tumours after failure of geographical region accounts partly for the aetiology of
two multikinase inhibitors (imatinib and sunitinib).19 HCC because hepatitis B virus infection is the
64 www.thelancet.com Vol 389 January 7, 2017
Articles
predominant underlying cause of HCC in most Asian A-LC, JML, RSF, M-AL, AB, GMe, and GH collected the data. JB, M-AL,
countries. AB, and GMe analysed and interpreted the data. All authors participated
in the drafting, review, and approval of the report and in the decision to
The safety of regorafenib in HCC in this study is submit for publication.
consistent with the safety profile of regorafenib in other
Declaration of interests
gastrointestinal malignancies, and with no new safety JB has received grants and personal fees from Bayer; consultancy and
concerns.18,19 The most common grade 3 or 4 adverse advisory fees from Bayer and Novartis; and consultancy fees from
events included hypertension, hand–foot skin reaction, Gilead, AbbVie, Kowa, BTG, ArQule, Terumo, Bristol-Myers Squibb,
fatigue, and diarrhoea. Exclusion of patients who were Boehringer Ingelheim, OSI, Roche, Eisai, Sirtex, and Onxeo. PM has
received consultancy fees from Bayer. OY has received grants from
unable to tolerate sorafenib could have reduced the Gilead Sciences, MSD, Bayer, Mitsubishi Tanabe Pharma, and Bristol-
occurrence of severe adverse events; 10% of patients Myers Squibb. OR has received personal fees from Transgene and
discontinued treatment due to a regorafenib-related Bristol-Myers Squibb. VB has received personal fees from Bayer,
adverse event. Although underlying liver dysfunction is Boehringer Ingelheim, Pfizer, MSD, and Roche; and non-financial
support from Boehringer Ingelheim, Pfizer, and MSD. RG has received
expected to be more common in patients with HCC, the advisory fees from Bayer France. PJR has received personal fees from
rates of liver-related adverse events and liver failure in the Bayer, Celgene, Roche, Merck, and Sirtex; advisory fees from Bayer,
regorafenib group were not higher in this study compared Baxalta, Amgen, and Sanofi; speaker fees from Celgene; and support for
with in other regorafenib trials.18,19 In this study, the only attending meetings from Bayer, Celgene, and Merck. J-PB has received
grants from Bayer during the conduct of the study and lecturing and
two cases of drug-related death due to liver failure consultancy fees from Bayer. IO-H has received grants and personal
occurred in the placebo group. Although adverse events fees from Bayer; personal fees from Gilead, Intercept, Daiichi Sankyo,
in the regorafenib group led to higher rates of treatment AbbVie, and Boehringer Ingelheim; grants from Lilly; and non-financial
interruptions and dose reductions than did those in the support from Gilead, MSD, and AbbVie. MK has received grants from
Chugai, Otsuka, Takeda, Taiho, Sumitomo Dainippon, Daiichi Sankyo,
placebo group, the median treatment duration was longer MSD, Eisai, Bayer, and AbbVie; lecturing fees from Bayer, Eisai, MSD,
with regorafenib than with placebo. Assessments using and Ajinomoto; and advisory and consultancy fees from Bayer, Eisai,
standard, validated measures of quality of life in patients Kowa, MSD, Bristol-Myers Squibb, Chugai, and Taiho. A-LC has
received consultancy fees from Novartis, Eisai, MSD, Bayer, Ono
with hepatobiliary cancer showed no clinically meaningful
Pharmaceuticals, Bristol-Myers Squibb, and Merck Serono. JML has
differences between the groups. received grants from Bayer, Bristol-Myers Squibb, Blueprint Medicines,
Although biomarker-based treatment decisions have and Boehringer Ingelheim; and consultancy fees from Bayer,
become standard of care in certain tumour types, no Bristol-Myers Squibb, Blueprint Medicines, Boehringer Ingelheim, Lilly
Pharmaceuticals, Celsion, Biocompatibles, and Novartis. RSF has
baseline markers predictive of treatment benefit have been
received grants, consultancy fees, and travel support from Bayer, Pfizer,
identified for patients with HCC.29,30 Exploratory studies Novartis, and Bristol-Myers Squibb. M-AL is an employee of Bayer. AB
have suggested that there is an association between certain is an employee of Bayer. GMe is an employee of Bayer and owns stock
adverse events, most notably hand–foot skin reaction, and in Bayer. GH has received a grant and advisory board and speaker fees
from Bayer. SQ, AG, Y-HH, GB, MP, GMa, and TS declare no
overall survival and time to progression.31 However,
competing interests.
because this approach is based on post-randomisation
Acknowledgments
events, it does not inform the selection of patients who This study was funded by Bayer. Editorial assistance in the preparation
could derive a greater treatment benefit. of this manuscript was provided by Ann Contijoch (Bayer) and
A potential limitation of the study is that it was Jennifer Tobin (Choice Healthcare Solutions, with financial support
undertaken in patients who progressed during previous from Bayer). We thank the patients who participated in the RESORCE
trial, their families, the RESORCE investigators, and the members of the
sorafenib treatment, and therefore firm conclusions Data Safety Monitoring Committee: Morris Sherman, Bruno Daniele,
about the efficacy of regorafenib in patients who do not Gregory J Gores, and KyungMann Kim.
tolerate sorafenib cannot be drawn. In addition, special References
populations, such as patients co-infected with HIV, are 1 Bruix J, Sherman M. Management of hepatocellular carcinoma:
not included here. an update. Hepatology 2011; 53: 1020–22.
2 Llovet JM, Ducreux M, Lencioni R, et al. EASL-EORTC clinical
The results of this study represent a significant advance practice guidelines: management of hepatocellular
in addressing an unmet need in the treatment of HCC. All carcinoma. J Hepatol 2012; 56: 908–43.
previous second-line trials of novel agents have failed;11–14 3 Kudo M, Matsui O, Izumi N, et al. JSH Consensus-based clinical
thus no effective systemic therapies after progression on practice guidelines for the management of hepatocellular
carcinoma: 2014 update by the Liver Cancer Study Group of Japan.
sorafenib are currently available. These data underscore Liver Cancer 2014; 3: 458–68.
that prolonging exposure to multikinase inhibitors such as 4 Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced
the sequence of sorafenib and regorafenib in conjunction hepatocellular carcinoma. N Engl J Med 2008; 359: 378–90.
5 Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib
with proper management of adverse events can lead to an in patients in the Asia-Pacific region with advanced hepatocellular
extension in survival. In conclusion, this study met its carcinoma: a phase III randomised, double-blind,
primary endpoint showing that regorafenib improves placebo-controlled trial. Lancet Oncol 2009; 10: 25–34.
6 Cheng AL, Kang YK, Lin DY, et al. Sunitinib versus sorafenib in
overall survival in patients with HCC who had disease advanced hepatocellular cancer: results of a randomized phase III
progression during first-line treatment with sorafenib. trial. J Clin Oncol 2013; 31: 4067–75.
Contributors 7 Johnson PJ, Qin S, Park JW, et al. Brivanib versus sorafenib as
JB, M-AL, RSF, and GMe conceived and designed the study. JB, SQ, PM, first-line therapy in patients with unresectable, advanced
hepatocellular carcinoma: results from the randomized phase III
AG, Y-HH, GB, MP, OY, OR, VB, RG, GMa, PJR, TS, J-PB, IO-H, MK,
BRISK-FL study. J Clin Oncol 2013; 31: 3517–24.
www.thelancet.com Vol 389 January 7, 2017 65
Articles
8 Cainap C, Qin S, Huang WT, et al. Linifanib versus sorafenib in 19 Demetri GD, Reichardt P, Kang YK, et al. Efficacy and safety of
patients with advanced hepatocellular carcinoma: results of a regorafenib for advanced gastrointestinal stromal tumours after
randomized phase III trial. J Clin Oncol 2015; 33: 172–79. failure of imatinib and sunitinib (GRID): an international,
9 Zhu AX, Rosmorduc O, Evans TR, et al. SEARCH: a phase III, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet
randomized, double-blind, placebo-controlled trial of sorafenib plus 2013; 381: 295–302.
erlotinib in patients with advanced hepatocellular carcinoma. 20 Stivarga Prescribing Information. Whippany, NJ: Bayer HealthCare
J Clin Oncol 2015; 33: 559–66. Pharmaceuticals; 2016.
10 Abou-Alfa GK, Niedzwieski D, Knox JJ, et al. Phase III randomized 21 Bruix J, Tak WY, Gasbarrini A, et al. Regorafenib as second-line
study of sorafenib plus doxorubicin versus sorafenib in patients therapy for intermediate or advanced hepatocellular carcinoma:
with advanced hepatocellular carcinoma (HCC): CALGB 80802 multicentre, open-label, phase II safety study. Eur J Cancer 2013;
(Alliance). Proc Am Soc Clin Oncol 2016; 34: abstr 4003. 49: 3412–19.
11 Llovet JM, Decaens T, Raoul JL, et al. Brivanib in patients with 22 Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment
advanced hepatocellular carcinoma who were intolerant to sorafenib for hepatocellular carcinoma. Semin Liver Dis 2010; 30: 52–60.
or for whom sorafenib failed: results from the randomized 23 Bruix J, Reig M, Sherman M. Evidence-based diagnosis, staging,
phase III BRISK-PS study. J Clin Oncol 2013; 31: 3509–16. and treatment of patients with hepatocellular carcinoma.
12 Zhu AX, Kudo M, Assenat E, et al. Effect of everolimus on survival Gastroenterology 2016; 150: 835–53.
in advanced hepatocellular carcinoma after failure of sorafenib: 24 Steel JL, Eton DT, Cella D, Olek MC, Carr BI. Clinically meaningful
the EVOLVE-1 randomized clinical trial. JAMA 2014; 312: 57–67. changes in health-related quality of life in patients diagnosed with
13 Zhu AX, Park JO, Ryoo BY, et al. Ramucirumab versus placebo as hepatobiliary carcinoma. Ann Oncol 2006; 17: 304–12.
second-line treatment in patients with advanced hepatocellular 25 Pickard AS, Neary MP, Cella D. Estimation of minimally important
carcinoma following first-line therapy with sorafenib (REACH): differences in EQ-5D utility and VAS scores in cancer.
a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol Health Qual Life Outcomes 2007; 5: 70.
2015; 16: 859–70. 26 Reig M, Rimola J, Torres F, et al. Postprogression survival of
14 Abou-Alfa GK, Qin S, Ryoo BY, et al. Phase III randomized study of patients with advanced hepatocellular carcinoma: rationale for
second-line ADI-peg 20 (A) plus best supportive care versus second-line trial design. Hepatology 2013; 58: 2023–31.
placebo (P) plus best supportive care in patients (pts) with advanced 27 Bruix J, Sherman M, Llovet JM, et al. Clinical management of
hepatocellular carcinoma (HCC). Proc Am Soc Clin Oncol 2016; hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL
34: abstr 4017. conference. European Association for the Study of the Liver.
15 Wilhelm SM, Dumas J, Adnane L, et al. Regorafenib (BAY 73-4506): J Hepatol 2001; 35: 421–30.
a new oral multikinase inhibitor of angiogenic, stromal and 28 Mazzoccoli G, Miele L, Oben J, Grieco A, Vinciguerra M.
oncogenic receptor tyrosine kinases with potent preclinical Biology, epidemiology, clinical aspects of hepatocellular carcinoma
antitumor activity. Int J Cancer 2011; 129: 245–55. and the role of sorafenib. Curr Drug Targets 2016; 17: 783–99.
16 Abou-Elkacem L, Arns S, Brix G, et al. Regorafenib inhibits growth, 29 Llovet JM, Peña CE, Lathia CD, et al. Plasma biomarkers as
angiogenesis, and metastasis in a highly aggressive, orthotopic predictors of outcome in patients with advanced hepatocellular
colon cancer model. Mol Cancer Ther 2013; 12: 1322–31. carcinoma. Clin Cancer Res 2012; 8: 2290–300.
17 Wilhelm SM, Carter C, Tang L, et al. BAY 43-9006 exhibits broad 30 Zhu AX, Kang YK, Rosmorduc O, et al. Biomarker analyses of
spectrum oral antitumor activity and targets the RAF/MEK/ERK clinical outcomes in patients with advanced hepatocellular
pathway and receptor tyrosine kinases involved in tumor carcinoma treated with sorafenib with or without erlotinib in the
progression and angiogenesis. Cancer Res 2004; 64: 7099–109. SEARCH trial. Clin Cancer Res 2016; 22: 4870–79.
18 Grothey A, Van Cutsem E, Sobrero A, et al. 31 Reig M, Torres F, Rodriguez-Lope C, et al. Early dermatologic
Regorafenib monotherapy for previously treated metastatic colorectal adverse events predict better outcome in HCC patients treated with
cancer (CORRECT): an international, multicentre, randomised, sorafenib. J Hepatol 2014; 61: 318–24.
placebo-controlled, phase 3 trial. Lancet 2013; 381: 303–12.
66 www.thelancet.com Vol 389 January 7, 2017
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 1.4 Useful Utils and ToolsDocument15 pages1.4 Useful Utils and Toolsjesus llumpoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Healing Spices How To Use 50 Everyday and Exotic Spices To Boost Health and Beat Disease by Bharat B Aggarwal PHD Debora Yost PDFDocument7 pagesHealing Spices How To Use 50 Everyday and Exotic Spices To Boost Health and Beat Disease by Bharat B Aggarwal PHD Debora Yost PDFkcmkcm0% (1)
- Medical Complications of Psychiatric IllnessDocument226 pagesMedical Complications of Psychiatric IllnessMesias Patricio100% (2)
- UWorld Notes - Peds 2Document38 pagesUWorld Notes - Peds 2Dylan GerlachNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Periodontal DiseaseDocument2 pagesPeriodontal Diseasekiki119100% (1)
- ENZYMOLOGYDocument2 pagesENZYMOLOGYCarla Lagar FloresNo ratings yet
- PNLE Sample QuestionsDocument18 pagesPNLE Sample QuestionsDanielle KayeNo ratings yet
- Stevia - A Tale of Greed Profit and Deceit - DR MercolaDocument15 pagesStevia - A Tale of Greed Profit and Deceit - DR Mercolakcopenhagen100% (1)
- Adult Reference Dose/volume Limits: Structure Volume (CC) Total Dose (Gy) Max Dose (Gy) Endpoint Notes ReferenceDocument6 pagesAdult Reference Dose/volume Limits: Structure Volume (CC) Total Dose (Gy) Max Dose (Gy) Endpoint Notes ReferenceEdis Đedović100% (1)
- WJG RegoDocument32 pagesWJG Regojesus llumpoNo ratings yet
- Sensors For Wearable Electronics & Mobile Healthcare: June © 2015Document43 pagesSensors For Wearable Electronics & Mobile Healthcare: June © 2015jesus llumpoNo ratings yet
- 1.5 Developer ToolsDocument7 pages1.5 Developer Toolsjesus llumpoNo ratings yet
- 1.3 Single Page ApplicationsDocument8 pages1.3 Single Page Applicationsjesus llumpoNo ratings yet
- 1.1 Client Server ArchitectureDocument15 pages1.1 Client Server Architecturejesus llumpoNo ratings yet
- 1.2 Model View Controller PatternDocument11 pages1.2 Model View Controller Patternjesus llumpoNo ratings yet
- Oral Cancer Awareness Among Non-Medical Professionals - A Cross Sectional Study in LadakhDocument8 pagesOral Cancer Awareness Among Non-Medical Professionals - A Cross Sectional Study in LadakhIJAR JOURNALNo ratings yet
- ABAcard p30 - Semen - Miami Dade Police - Adriana Kristaly - David SmithDocument9 pagesABAcard p30 - Semen - Miami Dade Police - Adriana Kristaly - David SmithmarthacoolNo ratings yet
- p41100 VEM Assignment-1Document6 pagesp41100 VEM Assignment-1Parag PardhiNo ratings yet
- Annexure VI: Proposal Form For Lic'S Cancer CoverDocument5 pagesAnnexure VI: Proposal Form For Lic'S Cancer Coversarbjeet kumarNo ratings yet
- Miniexcavadora xn16Document137 pagesMiniexcavadora xn16martin100% (1)
- ĐỀ 26Document6 pagesĐỀ 26Uyên Lê PhươngNo ratings yet
- Indications, Contraindications, Side Effects and General Notes Regarding Total Hip Replacement (THR) OperationDocument3 pagesIndications, Contraindications, Side Effects and General Notes Regarding Total Hip Replacement (THR) OperationAstrid Nasna LarasatiNo ratings yet
- How To Remove Asbestos: Asbestos - Sa.gov - AuDocument2 pagesHow To Remove Asbestos: Asbestos - Sa.gov - AuthisulaNo ratings yet
- Cho Session DesignDocument8 pagesCho Session DesignConsolacion Binarao DoloresNo ratings yet
- Brochure Transplant 2019 v2Document6 pagesBrochure Transplant 2019 v2anastNo ratings yet
- Front Matter 2021Document18 pagesFront Matter 2021Евгений ПанковецNo ratings yet
- ReferensiDocument126 pagesReferensiFatchul ChoiriNo ratings yet
- Dental Consideration in Respiratory DiseaseDocument6 pagesDental Consideration in Respiratory Diseasejagjit singhNo ratings yet
- Abstract PollutionDocument4 pagesAbstract Pollutionlogeshboy007No ratings yet
- Bio Graphic DataDocument3 pagesBio Graphic DatahellokittygirlNo ratings yet
- Chapter 14 Diseases of The PericardiumDocument12 pagesChapter 14 Diseases of The PericardiumfathirNo ratings yet
- (18414036 - ARS Medica Tomitana) Purely Cutaneous Rosai-Dorfman Disease: A True Clinical Diagnosis ChallengeDocument6 pages(18414036 - ARS Medica Tomitana) Purely Cutaneous Rosai-Dorfman Disease: A True Clinical Diagnosis Challengeadriana PeraltaNo ratings yet
- BMRC EPTB Proposal 18-10-13 2Document32 pagesBMRC EPTB Proposal 18-10-13 2Rizwan ShameemNo ratings yet
- ShipDocument6 pagesShipKota varunNo ratings yet
- Short-Term and Long-Term Physical Effects of Exposure To CS SprayDocument3 pagesShort-Term and Long-Term Physical Effects of Exposure To CS SprayRoman MamunNo ratings yet
- Dysphagia Handicap Index, Development and ValidationDocument7 pagesDysphagia Handicap Index, Development and ValidationWlf OoNo ratings yet
- Herbal CigarettesDocument5 pagesHerbal CigarettesAnushka GuptaNo ratings yet