You might also like
- Certificate of Physical FitnessDocument1 pageCertificate of Physical FitnessdeepusvvpNo ratings yet
- Form - 4 Certificate of FitnessDocument1 pageForm - 4 Certificate of FitnessAnandababuNo ratings yet
- Form No, 32 - Certificate of Fitness by Medical Practitioner - Hazardous and Dangerous Occupations - Punjab PDFDocument1 pageForm No, 32 - Certificate of Fitness by Medical Practitioner - Hazardous and Dangerous Occupations - Punjab PDFNiten Chopra0% (1)
- Sterilization Certificate FormatDocument1 pageSterilization Certificate Formatsciencewing rbi100% (1)
- FORM 27 - Certificate of Fitness For Employment in Hazardous ProcessesDocument2 pagesFORM 27 - Certificate of Fitness For Employment in Hazardous ProcesseszubairmbbsNo ratings yet
- William Carey University: Application Form For Issue of Migration CertificateDocument2 pagesWilliam Carey University: Application Form For Issue of Migration CertificateAnish Ag100% (1)
- Esic Form 7b WordDocument1 pageEsic Form 7b WordPatil Hemant67% (3)
- AFFIDAVIT Registered Pharmacist Karnataka PDFDocument4 pagesAFFIDAVIT Registered Pharmacist Karnataka PDFBalaji Pharmacy - GMNo ratings yet
- 09.medical Fitness Certificate Format 2013Document1 page09.medical Fitness Certificate Format 2013quantabosonNo ratings yet
- SDAT Sports Hostel Online Application For The Year2022-2023Document4 pagesSDAT Sports Hostel Online Application For The Year2022-2023VIBIN RONALDONo ratings yet
- Admit Card PDFDocument1 pageAdmit Card PDFatul012No ratings yet
- APSR-1.1Form of Physical FitnessDocument3 pagesAPSR-1.1Form of Physical Fitnessraghavbiduru1100% (1)
- A.P.Model School & JR College Yellanur Study & Conduct CertificateDocument1 pageA.P.Model School & JR College Yellanur Study & Conduct CertificaterajNo ratings yet
- Certificate of Medical Fitness AdmissionDocument1 pageCertificate of Medical Fitness AdmissionJagruti NaikNo ratings yet
- Med Unfit Form 3 PDFDocument1 pageMed Unfit Form 3 PDFamit_saxena_10No ratings yet
- Medical Certificate FormatDocument1 pageMedical Certificate FormatrashmarsvNo ratings yet
- Form 23Document1 pageForm 23hdpanchal86100% (2)
- Form - E: (See Rule 9 and 10)Document1 pageForm - E: (See Rule 9 and 10)vishalsolsheNo ratings yet
- TTL Safety PoliciesDocument60 pagesTTL Safety PoliciesCory WalkerNo ratings yet
- Form3 COPDocument2 pagesForm3 COPinaglepankaj2213No ratings yet
- Malaysia Fifth Schedule - Rev.1Document1 pageMalaysia Fifth Schedule - Rev.1Su Kil SungNo ratings yet
- 3 FORMAT OF MEDICAL FITNESS CERTIFICATE - OFF RoleDocument1 page3 FORMAT OF MEDICAL FITNESS CERTIFICATE - OFF RoleDipanjal Saikia100% (1)
- Annexures II IV South Central Railway Various PostsDocument5 pagesAnnexures II IV South Central Railway Various PostsRuthvik ReddyNo ratings yet
- Annex UreDocument12 pagesAnnex UreNewspaper boyNo ratings yet
- NEW Med ReportDocument1 pageNEW Med Reportmegan.hoover2722No ratings yet
- Indonesia - Measures Concerning The Importation of Chicken Meat and Chicken ProductsDocument160 pagesIndonesia - Measures Concerning The Importation of Chicken Meat and Chicken ProductsVicky Yuliana SaputriNo ratings yet
- Revised PF Withdrawal Form-19Document3 pagesRevised PF Withdrawal Form-19Sukhveer SinghNo ratings yet
- Application For HEALTH INSPECTOR (CIVILIAN)Document3 pagesApplication For HEALTH INSPECTOR (CIVILIAN)suchita_0607No ratings yet
- Format of Affidavit To Be Submitted by The Staff On Rs. 10/-Stamp PaperDocument1 pageFormat of Affidavit To Be Submitted by The Staff On Rs. 10/-Stamp PaperAmit SinghNo ratings yet
- CTX 510 Eco Rukovodstvo Po EkspluatatsiiDocument378 pagesCTX 510 Eco Rukovodstvo Po EkspluatatsiiAlekseyNo ratings yet
- Family Pension On The Death of PensionerDocument5 pagesFamily Pension On The Death of PensionerVipul RameshNo ratings yet
- Bond 2022 For Kerala Medical CollegeDocument9 pagesBond 2022 For Kerala Medical CollegeSinchan SharmaNo ratings yet
- PGS Da Gdi2010Document68 pagesPGS Da Gdi2010Daniel MorenoNo ratings yet
- Dental Amalgam Study 2008Document76 pagesDental Amalgam Study 2008NicolasDrazulNo ratings yet
- Exp CertDocument1 pageExp CertvintersmileNo ratings yet
- National Health and Nutrition Examination Survey: Physician Examination Procedures ManualDocument325 pagesNational Health and Nutrition Examination Survey: Physician Examination Procedures ManualSemadela SolichinNo ratings yet
- Show PDFDocument2 pagesShow PDFSandip MandalNo ratings yet
- Navy Manual of Naval Preventive MedicineDocument561 pagesNavy Manual of Naval Preventive MedicinePlainNormalGuy2No ratings yet
- Form 19Document3 pagesForm 1919CS224 Sarathy.RNo ratings yet
- Nomination PDFDocument1 pageNomination PDFymonafNo ratings yet
- Physical Fitness CertificateDocument1 pagePhysical Fitness Certificatedilip50% (8)
- Japan MilkDocument80 pagesJapan MilkPauline LamNo ratings yet
- Form of Nativity Certificate: Please Delete The Words Which Are Not ApplicableDocument1 pageForm of Nativity Certificate: Please Delete The Words Which Are Not ApplicablebalakalasNo ratings yet
- Form 19 EnglishDocument2 pagesForm 19 EnglishSachi SivamNo ratings yet
- State Bank of India ............................................................ Branch/OfficeDocument1 pageState Bank of India ............................................................ Branch/Officemani_588No ratings yet
- Rajasthan University of Health Sciences, Jaipur: Summary SheetDocument11 pagesRajasthan University of Health Sciences, Jaipur: Summary SheetJitendra ChoudharyNo ratings yet
- Form - A & Form-F: Application For Issuance of Certificate of PracticeDocument7 pagesForm - A & Form-F: Application For Issuance of Certificate of PracticeUmesh AraligidadNo ratings yet
- 3 - Frozen Fruits and Vegetables Processing Unit - IQFDocument70 pages3 - Frozen Fruits and Vegetables Processing Unit - IQFSaid Id100% (4)
- Member Registration Data Provisional Collection: A Better FutureDocument1 pageMember Registration Data Provisional Collection: A Better FutureMugenyiNo ratings yet
- If The Employee Is Allowed Increment After Crossing The EDocument1 pageIf The Employee Is Allowed Increment After Crossing The EINDIAN KNIGHTSNo ratings yet
- RZTDD 6 DDocument5 pagesRZTDD 6 DSABIR MNo ratings yet
- SA Medical Bi 811Document1 pageSA Medical Bi 811rajkmm36No ratings yet
- Rajasthan University of Health Sciences, Jaipur: Application Form For Post Basic B.Sc. Nursing (2 Years) 2011-12Document6 pagesRajasthan University of Health Sciences, Jaipur: Application Form For Post Basic B.Sc. Nursing (2 Years) 2011-12Jitendra ChoudharyNo ratings yet
- Dust HandbookDocument82 pagesDust HandbookuragunbagaNo ratings yet
- Consitutional Law I Digest CodexDocument39 pagesConsitutional Law I Digest CodexrjpogikaayoNo ratings yet
- Schedule ADocument82 pagesSchedule ATaskin SayyedNo ratings yet
- Ggggggggmmmfffmmnew PDFDocument49 pagesGgggggggmmmfffmmnew PDFBelayneh TadesseNo ratings yet
- MC FormDocument3 pagesMC FormSreeraj B PillaiNo ratings yet
- 20-054 - Airline Ground Service Equipment Mechanic Sep 19, 2020Document2 pages20-054 - Airline Ground Service Equipment Mechanic Sep 19, 2020dwi ari wibowoNo ratings yet
- Proformas of Service BookDocument25 pagesProformas of Service BookToshiba Tv100% (1)
- Hospital Annual Report (HAR) - Instructions: Financial, Utilization, and Services DataDocument48 pagesHospital Annual Report (HAR) - Instructions: Financial, Utilization, and Services DataKamalakar KaramchetiNo ratings yet
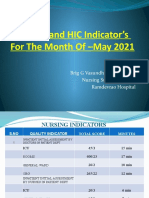
- Nursing and HIC Indicator's For The Month of - May 2021Document9 pagesNursing and HIC Indicator's For The Month of - May 2021Kamalakar KaramchetiNo ratings yet
- APIC FormsChecklists Volume01Document198 pagesAPIC FormsChecklists Volume01Kamalakar Karamcheti100% (1)
- 12 Software Validation LogDocument1 page12 Software Validation LogKamalakar KaramchetiNo ratings yet
- Implementation of 7 Core Principles of ISO 26000 (CSR) in Bangladesh: A Case Study On GrameenphoneDocument14 pagesImplementation of 7 Core Principles of ISO 26000 (CSR) in Bangladesh: A Case Study On GrameenphoneKamalakar KaramchetiNo ratings yet
- GDP Govt ReleaseDocument27 pagesGDP Govt ReleaseKamalakar KaramchetiNo ratings yet
- DNV-DS-HC102 Hospital Standard Guidelines and Guidance V3 0Document151 pagesDNV-DS-HC102 Hospital Standard Guidelines and Guidance V3 0Kamalakar KaramchetiNo ratings yet
- Institutionalise Quality: LT Col (DR) K KamalakarDocument24 pagesInstitutionalise Quality: LT Col (DR) K KamalakarKamalakar KaramchetiNo ratings yet
- 04 Control of Calibrated Equipment SOPDocument8 pages04 Control of Calibrated Equipment SOPKamalakar KaramchetiNo ratings yet
- SOP - Informed ConsentDocument16 pagesSOP - Informed ConsentKamalakar KaramchetiNo ratings yet
- Patient Safety Assessment Manual 2016 PDFDocument236 pagesPatient Safety Assessment Manual 2016 PDFKamalakar KaramchetiNo ratings yet
- Guidance Document - Medical Devices 2018 PDFDocument241 pagesGuidance Document - Medical Devices 2018 PDFKamalakar KaramchetiNo ratings yet
- OT Manual - EyeDocument202 pagesOT Manual - EyeKamalakar Karamcheti100% (1)
- ISMP AssessmentDocument56 pagesISMP AssessmentKamalakar KaramchetiNo ratings yet
- A-Level Chemistry Revision: Cheeky Revision ShortcutsFrom EverandA-Level Chemistry Revision: Cheeky Revision ShortcutsRating: 4 out of 5 stars4/5 (5)
- How to Teach Nature Journaling: Curiosity, Wonder, AttentionFrom EverandHow to Teach Nature Journaling: Curiosity, Wonder, AttentionRating: 4.5 out of 5 stars4.5/5 (3)
- Lower Secondary Science Workbook: Stage 8From EverandLower Secondary Science Workbook: Stage 8Rating: 5 out of 5 stars5/5 (1)
- Airplane Flying Handbook: FAA-H-8083-3C (2024)From EverandAirplane Flying Handbook: FAA-H-8083-3C (2024)Rating: 4 out of 5 stars4/5 (12)
- AI and the Future of Education: Teaching in the Age of Artificial IntelligenceFrom EverandAI and the Future of Education: Teaching in the Age of Artificial IntelligenceRating: 5 out of 5 stars5/5 (1)
- Interactive Science Notebook: The Human Body WorkbookFrom EverandInteractive Science Notebook: The Human Body WorkbookRating: 4 out of 5 stars4/5 (2)
- Common Core Science 4 Today, Grade 3: Daily Skill PracticeFrom EverandCommon Core Science 4 Today, Grade 3: Daily Skill PracticeRating: 3.5 out of 5 stars3.5/5 (2)
- The School Garden Curriculum: An Integrated K-8 Guide for Discovering Science, Ecology, and Whole-Systems ThinkingFrom EverandThe School Garden Curriculum: An Integrated K-8 Guide for Discovering Science, Ecology, and Whole-Systems ThinkingNo ratings yet
- A-level Biology Revision: Cheeky Revision ShortcutsFrom EverandA-level Biology Revision: Cheeky Revision ShortcutsRating: 5 out of 5 stars5/5 (5)
- Chemistry All-in-One For Dummies (+ Chapter Quizzes Online)From EverandChemistry All-in-One For Dummies (+ Chapter Quizzes Online)No ratings yet
- How to Think Like a Lawyer--and Why: A Common-Sense Guide to Everyday DilemmasFrom EverandHow to Think Like a Lawyer--and Why: A Common-Sense Guide to Everyday DilemmasRating: 3 out of 5 stars3/5 (1)
- What is the Scientific Method? Science Book for Kids | Children's Science BooksFrom EverandWhat is the Scientific Method? Science Book for Kids | Children's Science BooksRating: 5 out of 5 stars5/5 (1)
- Quantum Physics for Beginners: Simple Illustrated Guide to Discover with Practical Explanations the Paradoxes of the Life and Universe Reconsidering RealityFrom EverandQuantum Physics for Beginners: Simple Illustrated Guide to Discover with Practical Explanations the Paradoxes of the Life and Universe Reconsidering RealityRating: 2 out of 5 stars2/5 (1)
- How Do Cell Phones Work? Technology Book for Kids | Children's How Things Work BooksFrom EverandHow Do Cell Phones Work? Technology Book for Kids | Children's How Things Work BooksNo ratings yet
- Nature-Based Learning for Young Children: Anytime, Anywhere, on Any BudgetFrom EverandNature-Based Learning for Young Children: Anytime, Anywhere, on Any BudgetRating: 5 out of 5 stars5/5 (1)