You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Motivations For Seeking Outdoor ExperiencesDocument13 pagesMotivations For Seeking Outdoor ExperiencesMatthew Pringle100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Jarvis Neurological Assessment SummaryDocument11 pagesJarvis Neurological Assessment Summaryaderonke bello100% (2)
- Dunn and Dunn Learning StylesDocument22 pagesDunn and Dunn Learning Stylesblaze monique100% (1)
- Visual Perception FlashcardsDocument12 pagesVisual Perception FlashcardsfewjkhvbjkhlckvsjdbNo ratings yet
- Cyp2c19, Ugt2b7, Ugt1a8Document8 pagesCyp2c19, Ugt2b7, Ugt1a8Nandit BanawalikarNo ratings yet
- Association of UGT2B7 and UGT1A4 Polymorphisms With Serum Concentration of Antiepileptic Drugs in Children Medscimonit-22-4107Document7 pagesAssociation of UGT2B7 and UGT1A4 Polymorphisms With Serum Concentration of Antiepileptic Drugs in Children Medscimonit-22-4107Nandit BanawalikarNo ratings yet
- Gastrointestinal Drugs: Dr. Nandit P BDocument34 pagesGastrointestinal Drugs: Dr. Nandit P BNandit BanawalikarNo ratings yet
- Pharmacotherapy of Epilepsy: Nandit P BDocument53 pagesPharmacotherapy of Epilepsy: Nandit P BNandit BanawalikarNo ratings yet
- Polymerase Chain Reaction & Types: Nandith P B Research ScholarDocument22 pagesPolymerase Chain Reaction & Types: Nandith P B Research ScholarNandit Banawalikar100% (1)
- High Performance Liquid Chromatography (HPLC) : Presenter: Nandit P BDocument39 pagesHigh Performance Liquid Chromatography (HPLC) : Presenter: Nandit P BNandit BanawalikarNo ratings yet
- NEUROTRANSMITTERDocument28 pagesNEUROTRANSMITTERiqiqiqiqiq100% (1)
- التفكير المنظومي 2012Document22 pagesالتفكير المنظومي 2012lizamarai454No ratings yet
- Internet AddictionDocument15 pagesInternet AddictionAmimie LingNo ratings yet
- Balance Exercise For ElderlyDocument46 pagesBalance Exercise For ElderlyReni ZubirNo ratings yet
- REACTION PAPER SubmittedDocument3 pagesREACTION PAPER SubmittedMaria Catalina PorcadillaNo ratings yet
- Maslow's Theory of Human Motivation PDFDocument2 pagesMaslow's Theory of Human Motivation PDFnagarajhebbarNo ratings yet
- A Study On Self Concept in Relation To Academic Achievement Among B.Ed TraineesDocument9 pagesA Study On Self Concept in Relation To Academic Achievement Among B.Ed TraineesEditor IJTSRDNo ratings yet
- Bagaimana Memilih Metode Dan Teknik PembelajaranDocument13 pagesBagaimana Memilih Metode Dan Teknik PembelajaranSyarif LuqmanNo ratings yet
- E Book AddictionandAttachmentDocument246 pagesE Book AddictionandAttachmentMarilyn Cercado FernandezNo ratings yet
- CouselingDocument5 pagesCouselingFhaij AbdrjNo ratings yet
- 11 Brain & LanguageDocument20 pages11 Brain & LanguageIvan Giovanni MiterNo ratings yet
- D4 Professıonal Educatıon Theft School Equipment Like TVDocument12 pagesD4 Professıonal Educatıon Theft School Equipment Like TVAshley RañesesNo ratings yet
- Reflective Practice G Bishop - 2Document47 pagesReflective Practice G Bishop - 2sCore IELTSNo ratings yet
- Sample Intake PaperDocument5 pagesSample Intake PaperSinthia RahmanNo ratings yet
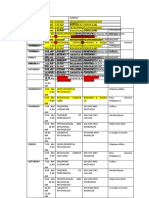
- BSP - 2ND Year, 2ND Sem TentativeDocument1 pageBSP - 2ND Year, 2ND Sem TentativeCyriz Matthew MontesNo ratings yet
- What Is Psychology - A DetailDocument23 pagesWhat Is Psychology - A DetailShraddha KarkiNo ratings yet
- SP2 Short Form and Caregiver Template Summary & Interpretation FormDocument4 pagesSP2 Short Form and Caregiver Template Summary & Interpretation FormjcNo ratings yet
- Assessing Sleep Qualityof SHSStudentsDocument10 pagesAssessing Sleep Qualityof SHSStudentskberrameNo ratings yet
- Principles of LearningDocument5 pagesPrinciples of LearningJonah Mendoza LatorreNo ratings yet
- Arredondo 2015Document15 pagesArredondo 2015argiaescuNo ratings yet
- Developing A Health Education PlanDocument5 pagesDeveloping A Health Education PlankimcheeseNo ratings yet
- Semester Essay - AlcoholDocument9 pagesSemester Essay - AlcoholEmma Kate LaubscherNo ratings yet
- Cell Signaling Write UpDocument4 pagesCell Signaling Write Upinfinity chronusNo ratings yet
- Good Will HuntingDocument1 pageGood Will HuntingnanananNo ratings yet
- TfEL South Australian Teaching FrameworkDocument88 pagesTfEL South Australian Teaching FrameworkShiftySteveNo ratings yet
- Prepared By: Harris Khaliq Tayyab Roll Number:11339 Subject: Self Management SkillsDocument9 pagesPrepared By: Harris Khaliq Tayyab Roll Number:11339 Subject: Self Management Skillssana_571No ratings yet