You might also like
- Consent Form (Sinovac)Document1 pageConsent Form (Sinovac)Kresta BenignoNo ratings yet
- (SINOVAC) Informed Consent Form - Eng March 5 2021Document1 page(SINOVAC) Informed Consent Form - Eng March 5 2021Mark Anthony RosasNo ratings yet
- Covid Vaccine Clover Form2948Document1 pageCovid Vaccine Clover Form2948marian2277No ratings yet
- Boosters Informed Consent Form ENGDocument1 pageBoosters Informed Consent Form ENGMoi ValdozNo ratings yet
- Pfizer COVID Vaccine Consent FormDocument1 pagePfizer COVID Vaccine Consent FormChristie ConalesNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.No ratings yet
- AstraZeneca COVID-19 vaccine informed consentDocument1 pageAstraZeneca COVID-19 vaccine informed consentJohn BNo ratings yet
- (ASTRAZENECA) Informed Consent Form - Eng March 5 2021Document1 page(ASTRAZENECA) Informed Consent Form - Eng March 5 2021Mara Ozoa VillaroyaNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineBelle Alaba - RabiaNo ratings yet
- Pfizer (Informed Consent Form) Eng - April 15 2021Document1 pagePfizer (Informed Consent Form) Eng - April 15 2021aleiah jean libatiqueNo ratings yet
- PEDIA Informed Consent Form PfizerDocument2 pagesPEDIA Informed Consent Form PfizerBalba ChrislynNo ratings yet
- Congvax Consent FormDocument3 pagesCongvax Consent FormRico MaligayaNo ratings yet
- Informed Consent Form Pfizer EnglishDocument2 pagesInformed Consent Form Pfizer EnglishIway SheenaNo ratings yet
- Parental Consent Form-EnGDocument2 pagesParental Consent Form-EnGMyrna ParasNo ratings yet
- Pfizer Consent Form - FillableDocument8 pagesPfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNo ratings yet
- (Informed Consent) Covid-19 Vaccine Forms EngDocument1 page(Informed Consent) Covid-19 Vaccine Forms EngYosh PamatmatNo ratings yet
- Consent 5 11 LandscapeDocument4 pagesConsent 5 11 LandscapeTin Pero-Rosal SaysonNo ratings yet
- Vaccine - Consent Form For Individuals 5-17 Years of Age - 01072022Document2 pagesVaccine - Consent Form For Individuals 5-17 Years of Age - 01072022Xenia Je SongcayaNo ratings yet
- Pfizer-Biontech Covid-19 Vaccine Consent Form For Individuals Under 18 Years of AgeDocument2 pagesPfizer-Biontech Covid-19 Vaccine Consent Form For Individuals Under 18 Years of AgeEric Canady ElNo ratings yet
- NMDOH Parental Consent Form for COVID-19 Administration 04162021Document1 pageNMDOH Parental Consent Form for COVID-19 Administration 04162021Kristina GarciaNo ratings yet
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Document4 pagesCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1bersabeh abayNo ratings yet
- Amdocs Waiver - Phillipines v.2Document1 pageAmdocs Waiver - Phillipines v.2A throw awayNo ratings yet
- COVID Vaccine Refusal FormDocument4 pagesCOVID Vaccine Refusal FormElizabeth AshtonNo ratings yet
- Covid-19 Vaccine Public FAQDocument7 pagesCovid-19 Vaccine Public FAQWXYZ-TV Channel 7 DetroitNo ratings yet
- COVD 19 Vaction Form 2020 Pfizerv2Document1 pageCOVD 19 Vaction Form 2020 Pfizerv2Neel YoyoNo ratings yet
- COVID19 Vaccination Guidefor Eligible BeneficiariesDocument16 pagesCOVID19 Vaccination Guidefor Eligible BeneficiariesKartik R. MorjariaNo ratings yet
- Pfizer Vaccine Consent FormDocument2 pagesPfizer Vaccine Consent FormPaulina HernandezNo ratings yet
- parcf (1)Document8 pagesparcf (1)Googool YNo ratings yet
- COVID Vaccine FAQ January 20Document2 pagesCOVID Vaccine FAQ January 20Sara PoppinsNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- COVID Vaccine FAQs: Top Questions AnsweredDocument7 pagesCOVID Vaccine FAQs: Top Questions AnsweredIshu AgrawalNo ratings yet
- Waiver and Assumption of RiskDocument11 pagesWaiver and Assumption of RisklancedadorNo ratings yet
- Notice of Liability: Re: Vaccines Administered To Minors (18 and Under)Document2 pagesNotice of Liability: Re: Vaccines Administered To Minors (18 and Under)Cathy GabroninoNo ratings yet
- Hawaii Schools C&D NOL 51821Document11 pagesHawaii Schools C&D NOL 51821Jamie WhiteNo ratings yet
- Joint Waiver On Covid-19 VaccinationDocument3 pagesJoint Waiver On Covid-19 VaccinationAlexanderNo ratings yet
- COVID-19 Vaccine Declination FormDocument4 pagesCOVID-19 Vaccine Declination FormMark McLean100% (1)
- Frequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseDocument8 pagesFrequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseCNBCTV18 DigitalNo ratings yet
- Eligibility Declaration Form: COVID-19 Vaccine RolloutDocument4 pagesEligibility Declaration Form: COVID-19 Vaccine RolloutMoey AwadNo ratings yet
- 6076e3e727bb4e3ee4bd8b74 Vaccine Public LetterDocument4 pages6076e3e727bb4e3ee4bd8b74 Vaccine Public LetterAngelaNo ratings yet
- D - Vaccination Minor Consent FormDocument2 pagesD - Vaccination Minor Consent FormNoemi CamberosNo ratings yet
- Fact-Sheet-Recipients-Caregivers-Moderna Covid-19 Vaccine 1Document5 pagesFact-Sheet-Recipients-Caregivers-Moderna Covid-19 Vaccine 1api-537351752No ratings yet
- Risk of COVID-19 Disease Transmission During IVF Treatment WaiverDocument2 pagesRisk of COVID-19 Disease Transmission During IVF Treatment WaiveraleonalonsoNo ratings yet
- Information On COVID-19 Pfizer (Comirnaty) VaccineDocument4 pagesInformation On COVID-19 Pfizer (Comirnaty) VaccineLa LuneNo ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- COVID-19 Vaccine Screening and Agreement: Contact Information - Person Being VaccinatedDocument7 pagesCOVID-19 Vaccine Screening and Agreement: Contact Information - Person Being VaccinatedLuz VelezNo ratings yet
- Annex C - COVID Waiver For Junior InternshipDocument2 pagesAnnex C - COVID Waiver For Junior InternshipDrina PaglinawanNo ratings yet
- Consent Form and Information SheetDocument3 pagesConsent Form and Information SheetTravis FlowersNo ratings yet
- EUA 27034.167 - FS For Recipients and Caregivers - Final - 5.10.2021Document7 pagesEUA 27034.167 - FS For Recipients and Caregivers - Final - 5.10.2021Diona SmithNo ratings yet
- Medical Religious Exemption FormDocument4 pagesMedical Religious Exemption FormWilberellisNo ratings yet
- COVID 19 ConsentDocument2 pagesCOVID 19 Consentstephany steinbergNo ratings yet
- Covid-19 Vaccine Public FAQDocument10 pagesCovid-19 Vaccine Public FAQWXYZ-TV Channel 7 DetroitNo ratings yet
- COVID-19 Vaccine Frequently Asked Questions April 1, 2022 New/Updated Information Is Highlighted in YellowDocument14 pagesCOVID-19 Vaccine Frequently Asked Questions April 1, 2022 New/Updated Information Is Highlighted in YellowMadonna FletcherNo ratings yet
- How To Obtain The Letter of Consent For Covid Vaccine For Children From 5 To 11 Years OldDocument2 pagesHow To Obtain The Letter of Consent For Covid Vaccine For Children From 5 To 11 Years OldScribdTranslationsNo ratings yet
- Public FAQDocument15 pagesPublic FAQIan WeberNo ratings yet
- Vaccine MemosDocument13 pagesVaccine MemosThe Daily OrangeNo ratings yet
- Frequently Asked Questions: COVID-19 VaccinesDocument16 pagesFrequently Asked Questions: COVID-19 VaccinesWXYZ-TV Channel 7 DetroitNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- How to Arm Yourself Against Vaccine Injuries And What to Do If Things Go WrongFrom EverandHow to Arm Yourself Against Vaccine Injuries And What to Do If Things Go WrongNo ratings yet
- Soft Blue Orange Harmonie Simple Minimalist Presentation TemplateDocument8 pagesSoft Blue Orange Harmonie Simple Minimalist Presentation TemplateBruce GonzalesNo ratings yet
- Batik DesignDocument4 pagesBatik DesignBruce GonzalesNo ratings yet
- Basketball BasicsDocument9 pagesBasketball BasicsBruce GonzalesNo ratings yet
- Activity in Music: Direction: Design and Describe Your Own Tabla and Bhaya InstrumentDocument1 pageActivity in Music: Direction: Design and Describe Your Own Tabla and Bhaya InstrumentBruce GonzalesNo ratings yet
- Soft Blue Orange Harmonie Simple Minimalist Presentation TemplateDocument8 pagesSoft Blue Orange Harmonie Simple Minimalist Presentation TemplateBruce GonzalesNo ratings yet
- Gonzales, Angelyn Kyle 12-PiusDocument1 pageGonzales, Angelyn Kyle 12-PiusBruce GonzalesNo ratings yet
- Profiling Form INDIGENTSDocument2 pagesProfiling Form INDIGENTSBruce GonzalesNo ratings yet
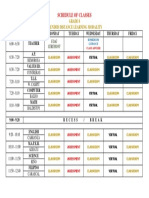
- Schedule of Classes: Grade 8 Blended Distance Learning ModalityDocument1 pageSchedule of Classes: Grade 8 Blended Distance Learning ModalityBruce GonzalesNo ratings yet
- Bruce Gonzales - Template FamilyDocument2 pagesBruce Gonzales - Template FamilyBruce GonzalesNo ratings yet
- Algeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaDocument1 pageAlgeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaBruce GonzalesNo ratings yet
- Bruce Gonzales - Template FamilyDocument2 pagesBruce Gonzales - Template FamilyBruce GonzalesNo ratings yet
- Kassandra Alexios Shared Epic GearDocument80 pagesKassandra Alexios Shared Epic GearJohn K Smith25% (4)
- Algeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaDocument1 pageAlgeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaBruce GonzalesNo ratings yet
- Algeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaDocument1 pageAlgeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaBruce GonzalesNo ratings yet
- Algeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaDocument1 pageAlgeria - Algiers (El Djazaïr) Egypt .Cairo Libya - Tripoli: TunisiaBruce GonzalesNo ratings yet
- Russia - Moscow: France .ParisDocument1 pageRussia - Moscow: France .ParisBruce GonzalesNo ratings yet
- Russia .Moscow: China - BeijingDocument1 pageRussia .Moscow: China - BeijingBruce GonzalesNo ratings yet
- Russia .Moscow: China - BeijingDocument1 pageRussia .Moscow: China - BeijingBruce GonzalesNo ratings yet
- Aplastic Anemia and HomoeopathyDocument3 pagesAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Atlas of Clinical HematologyDocument146 pagesAtlas of Clinical HematologyMaath Khalid100% (11)
- CELLULAR INJURY AND INFLAMMATIONDocument10 pagesCELLULAR INJURY AND INFLAMMATIONBravya NiharikaNo ratings yet
- Rash Non Blanching Nhs GuidesDocument3 pagesRash Non Blanching Nhs Guidesapi-238551404No ratings yet
- Hematologic System and DisordersDocument68 pagesHematologic System and DisordersRellie Castro100% (1)
- Oncologic NursingDocument132 pagesOncologic Nursingɹǝʍdןnos100% (10)
- Bleeding Disorders: LCDR Art GeorgeDocument54 pagesBleeding Disorders: LCDR Art GeorgepallavberiNo ratings yet
- Thrombocytopenia Pocket GuideDocument8 pagesThrombocytopenia Pocket GuideAnnisaValentKhanNo ratings yet
- MY Hematology MasterclassDocument32 pagesMY Hematology Masterclassabdul qayyumNo ratings yet
- Thrombocytopenia in PregnancyDocument31 pagesThrombocytopenia in Pregnancyari naNo ratings yet
- Botryoid Nuclei in The Peripheral Blood of A Dog With HeatstrokeDocument5 pagesBotryoid Nuclei in The Peripheral Blood of A Dog With HeatstrokeLaboratorio de BioquimicaNo ratings yet
- MOST IMPORATANT ONE LINERS Compiled by Medicinosis Magnus 2Document18 pagesMOST IMPORATANT ONE LINERS Compiled by Medicinosis Magnus 2VAIBHAV SHARMA- 122No ratings yet
- Approach To A Bleeding NeonateDocument51 pagesApproach To A Bleeding NeonateJosmy JosephNo ratings yet
- Vas 004Document16 pagesVas 004Stephen CandinegaraNo ratings yet
- 1.amal S. Elhassade Et Al.Document3 pages1.amal S. Elhassade Et Al.International Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Bleeding Disorders 1Document152 pagesBleeding Disorders 1Shameena KnNo ratings yet
- How I Use Platelet TransfusionsDocument12 pagesHow I Use Platelet TransfusionsJovanna OrtuñoNo ratings yet
- Management of Patients With Nonmalignant Hematologic DisordersDocument97 pagesManagement of Patients With Nonmalignant Hematologic DisordersJulia Rae Delos SantosNo ratings yet
- Case Report on a 23-Month-Old Boy with Grade I Dengue Hemorrhagic FeverDocument49 pagesCase Report on a 23-Month-Old Boy with Grade I Dengue Hemorrhagic FeverPashëm IndonesiaNo ratings yet
- Haematology Physical AssessmentDocument26 pagesHaematology Physical AssessmentMarium Mohamed Ali100% (1)
- 62 Coagulation Failure in ObstetricsDocument28 pages62 Coagulation Failure in ObstetricscollinsmagNo ratings yet
- Hematologic DiseasesDocument13 pagesHematologic DiseaseshithNo ratings yet
- Thrombopoietin Receptor AgonistsDocument4 pagesThrombopoietin Receptor Agonistskhangsiean89No ratings yet
- Hematology MCCQE ReviewDocument46 pagesHematology MCCQE ReviewMustafa Khandgawi100% (1)
- Anemia Aplasica - BMJDocument21 pagesAnemia Aplasica - BMJPaola Alexandra Chavez FNo ratings yet
- Hematologic Diseases OverviewDocument11 pagesHematologic Diseases OverviewPerrilyn Perey100% (2)
- PBL Haematology (Bleeding) - B5Document49 pagesPBL Haematology (Bleeding) - B5nishibuchiNo ratings yet
- Hematologic Complications in Patients Hospitalized With COVID 19 InfectionDocument7 pagesHematologic Complications in Patients Hospitalized With COVID 19 Infectionedson floresNo ratings yet
- How Do We Approach Thrombocytopenia in Critically IllDocument16 pagesHow Do We Approach Thrombocytopenia in Critically IllRendyNo ratings yet
- Massive Transfusion. CHEST. 2009.Document14 pagesMassive Transfusion. CHEST. 2009.Jose Fernando Díez ConchaNo ratings yet