You might also like
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineBelle Alaba - RabiaNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineJohn BNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.No ratings yet
- Boosters Informed Consent Form ENGDocument1 pageBoosters Informed Consent Form ENGMoi ValdozNo ratings yet
- Moderna Informed Consent Form Eng June 18 2021Document1 pageModerna Informed Consent Form Eng June 18 2021Bruce GonzalesNo ratings yet
- Consent Form (Sinovac)Document1 pageConsent Form (Sinovac)Kresta BenignoNo ratings yet
- Covid Vaccine Clover Form2948Document1 pageCovid Vaccine Clover Form2948marian2277No ratings yet
- (SINOVAC) Informed Consent Form - Eng March 5 2021Document1 page(SINOVAC) Informed Consent Form - Eng March 5 2021Mark Anthony RosasNo ratings yet
- Pfizer Informed Consent Form Eng - April 15 2021Document1 pagePfizer Informed Consent Form Eng - April 15 2021Christie ConalesNo ratings yet
- Pfizer (Informed Consent Form) Eng - April 15 2021Document1 pagePfizer (Informed Consent Form) Eng - April 15 2021aleiah jean libatiqueNo ratings yet
- Congvax Consent FormDocument3 pagesCongvax Consent FormRico MaligayaNo ratings yet
- PEDIA Informed Consent Form PfizerDocument2 pagesPEDIA Informed Consent Form PfizerBalba ChrislynNo ratings yet
- Parental Consent Form-EnGDocument2 pagesParental Consent Form-EnGMyrna ParasNo ratings yet
- Informed Consent Form Pfizer EnglishDocument2 pagesInformed Consent Form Pfizer EnglishIway SheenaNo ratings yet
- (Informed Consent) Covid-19 Vaccine Forms EngDocument1 page(Informed Consent) Covid-19 Vaccine Forms EngYosh PamatmatNo ratings yet
- Vaccine - Consent Form For Individuals 5-17 Years of Age - 01072022Document2 pagesVaccine - Consent Form For Individuals 5-17 Years of Age - 01072022Xenia Je SongcayaNo ratings yet
- Pfizer-Biontech Covid-19 Vaccine Consent Form For Individuals Under 18 Years of AgeDocument2 pagesPfizer-Biontech Covid-19 Vaccine Consent Form For Individuals Under 18 Years of AgeEric Canady ElNo ratings yet
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Document4 pagesCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1bersabeh abayNo ratings yet
- Pfizer Consent Form - FillableDocument8 pagesPfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNo ratings yet
- D - Vaccination Minor Consent FormDocument2 pagesD - Vaccination Minor Consent FormNoemi CamberosNo ratings yet
- NMDOH Parental Consent Form For COVID-19 Administration 04162021Document1 pageNMDOH Parental Consent Form For COVID-19 Administration 04162021Kristina GarciaNo ratings yet
- Pfizer Minor Consent Form Sample ADADocument2 pagesPfizer Minor Consent Form Sample ADAPaulina HernandezNo ratings yet
- ParcfDocument8 pagesParcfGoogool YNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- Registration and Consent Form For Covid 19 Vaccination 05.03.21Document4 pagesRegistration and Consent Form For Covid 19 Vaccination 05.03.21Yash HardowarNo ratings yet
- Amdocs Waiver - Phillipines v.2Document1 pageAmdocs Waiver - Phillipines v.2A throw awayNo ratings yet
- Consent For Minor Covid-19 Vaccination FormDocument3 pagesConsent For Minor Covid-19 Vaccination FormRechelle Ann TerrenalNo ratings yet
- Covid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 VaccineDocument2 pagesCovid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 Vaccinesiriamma wiliamsNo ratings yet
- COVD 19 Vaction Form 2020 Pfizerv2Document1 pageCOVD 19 Vaction Form 2020 Pfizerv2Neel YoyoNo ratings yet
- Joint Waiver On Covid-19 VaccinationDocument3 pagesJoint Waiver On Covid-19 VaccinationAlexanderNo ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- QC Protektodo Forms Sinopharm 1st Dose AranetaDocument3 pagesQC Protektodo Forms Sinopharm 1st Dose AranetaRalph Clinton PalomenoNo ratings yet
- Consent 5 11 LandscapeDocument4 pagesConsent 5 11 LandscapeTin Pero-Rosal SaysonNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Document6 pagesCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Stephanie BewleyNo ratings yet
- The Vaccine Injury Compensation Program (VICP) : Who Can File A Claim?Document2 pagesThe Vaccine Injury Compensation Program (VICP) : Who Can File A Claim?Mommyx44No ratings yet
- Eligibility Declaration Form: COVID-19 Vaccine RolloutDocument4 pagesEligibility Declaration Form: COVID-19 Vaccine RolloutMoey AwadNo ratings yet
- Covid19vaccineconsentform UpdatedDocument2 pagesCovid19vaccineconsentform UpdatedGlenn ReinhardtNo ratings yet
- Final SPMCWaiverfortraineesandaffiliatesDocument3 pagesFinal SPMCWaiverfortraineesandaffiliatesSuzanne AndresNo ratings yet
- BivalentConsent MichaelBelen HAG322426Document2 pagesBivalentConsent MichaelBelen HAG322426michaeljohnbelen14No ratings yet
- Consent Form and Information SheetDocument3 pagesConsent Form and Information SheetTravis FlowersNo ratings yet
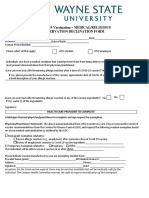
- WAYNE STATE U Covid Vaccine Declination FormDocument3 pagesWAYNE STATE U Covid Vaccine Declination FormWXYZ-TV Channel 7 DetroitNo ratings yet
- Medical QuestionnaireDocument2 pagesMedical QuestionnaireKunal GuptaNo ratings yet
- Vaccination Notice Affidavit: Mother and Father of - NAME - I/ or My ChildDocument2 pagesVaccination Notice Affidavit: Mother and Father of - NAME - I/ or My ChildMatthew McClusterNo ratings yet
- Risk of COVID-19 Disease Transmission During IVF Treatment WaiverDocument2 pagesRisk of COVID-19 Disease Transmission During IVF Treatment WaiveraleonalonsoNo ratings yet
- FINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Document2 pagesFINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Natasa PrelevicNo ratings yet
- Covid-19 Self-Certification Form June 2021-2Document1 pageCovid-19 Self-Certification Form June 2021-2zahid- techNo ratings yet
- REV - Inpatient Claim Form - AIADocument2 pagesREV - Inpatient Claim Form - AIAYen SylvaniNo ratings yet
- Vaccination Drive Confirmatin FormDocument2 pagesVaccination Drive Confirmatin Formpan.ben83No ratings yet
- PHE 11920 Covid-19 Consent Form Frontline SCSDocument1 pagePHE 11920 Covid-19 Consent Form Frontline SCSCormac QuinnNo ratings yet
- 08.10.2021-COVID Vaccine Declination FormDocument4 pages08.10.2021-COVID Vaccine Declination FormElizabeth AshtonNo ratings yet
- Influenza/Pneumococcal Immunization Consent FormDocument1 pageInfluenza/Pneumococcal Immunization Consent FormAna AsmaraNo ratings yet
- Claim Form-MD IndiaDocument5 pagesClaim Form-MD IndiaMusycal FynncNo ratings yet
- Annex C - COVID Waiver For Junior InternshipDocument2 pagesAnnex C - COVID Waiver For Junior InternshipDrina PaglinawanNo ratings yet
- 6076e3e727bb4e3ee4bd8b74 Vaccine Public LetterDocument4 pages6076e3e727bb4e3ee4bd8b74 Vaccine Public LetterAngelaNo ratings yet
- Hawaii Schools C&D NOL 51821Document11 pagesHawaii Schools C&D NOL 51821Jamie WhiteNo ratings yet
- MD India Insurance Claim FormDocument5 pagesMD India Insurance Claim FormYogesh ParchaniNo ratings yet
- Decision To Not Vaccinate My Child: Vaccine / DiseaseDocument2 pagesDecision To Not Vaccinate My Child: Vaccine / DiseaseNano InnaNo ratings yet
- Final SPMCWaiverfortraineesandaffiliates-1Document3 pagesFinal SPMCWaiverfortraineesandaffiliates-1Brandone Dave ParagosoNo ratings yet
- 2020 Review For Print PRE TEST IN BIOCHEMIStryDocument14 pages2020 Review For Print PRE TEST IN BIOCHEMIStryMara Ozoa VillaroyaNo ratings yet
- Board ReviewDocument17 pagesBoard ReviewMara Ozoa VillaroyaNo ratings yet
- Preventive MedicineDocument10 pagesPreventive MedicineHuji JalamiNo ratings yet
- PMRF 012020 PDFDocument2 pagesPMRF 012020 PDFJenilyn Gonzales Narrido100% (2)
- Ceramic Fiber 23Document28 pagesCeramic Fiber 23Kowsik RajendranNo ratings yet
- Design of Marina Structures and FacilitiesDocument23 pagesDesign of Marina Structures and FacilitiesAhmed Balah0% (1)
- Plumbing Specifications: Catch Basin PlanDocument1 pagePlumbing Specifications: Catch Basin PlanMark Allan RojoNo ratings yet
- Pneumatic Oscillator Valve - Pneumatic Controls - Impulse Automation LTDDocument3 pagesPneumatic Oscillator Valve - Pneumatic Controls - Impulse Automation LTDDindin NajmudinNo ratings yet
- Black and Decker Vaporera Electrica RecetarioDocument17 pagesBlack and Decker Vaporera Electrica RecetarioFabio AtenógenesNo ratings yet
- FPC Manual PreviewDocument5 pagesFPC Manual PreviewIbrahim Levent AkkoyunluNo ratings yet
- Carti Libraria Victor Papilian Ian 2015Document8 pagesCarti Libraria Victor Papilian Ian 2015Petru AcozmeiNo ratings yet
- 4 Strength and Durability of Concrete With LC3Document41 pages4 Strength and Durability of Concrete With LC3Mirza BasitNo ratings yet
- Enzyme Review Mcqs (From The Official Biochemistry Study Guide)Document5 pagesEnzyme Review Mcqs (From The Official Biochemistry Study Guide)Mrs Rehan100% (1)
- MahuaDocument12 pagesMahuaVinay ChhalotreNo ratings yet
- ISO 9001: 2015 Certified Semen Freezing LaboratoryDocument43 pagesISO 9001: 2015 Certified Semen Freezing LaboratoryShubhamNo ratings yet
- Program Thành TrungDocument3 pagesProgram Thành TrungQuốc HuyNo ratings yet
- Introduction To Mine SurveyingDocument7 pagesIntroduction To Mine SurveyingJoshua Miguel MejiasNo ratings yet
- Work Immersion Rubric & Assessment ReportDocument2 pagesWork Immersion Rubric & Assessment ReportJEE AR CANTERENo ratings yet
- Made in His ImageThe Amazing Design of The Human BodyDocument4 pagesMade in His ImageThe Amazing Design of The Human BodyAriam MariaNo ratings yet
- Valerie Tillard Murder: Probable CauseDocument11 pagesValerie Tillard Murder: Probable CauseLeigh EganNo ratings yet
- DGMS Final ReportDocument15 pagesDGMS Final ReportMaverickNo ratings yet
- P2 Nursing InfoDocument14 pagesP2 Nursing InfoMargarita Limon BalunesNo ratings yet
- 2 Day ALS Programme 24 Candidates IO ARS (March 2016) PDFDocument2 pages2 Day ALS Programme 24 Candidates IO ARS (March 2016) PDFCojocariu Emanuel50% (2)
- TympanometerDocument12 pagesTympanometerAli ImranNo ratings yet
- Acute GastroenteritisDocument7 pagesAcute GastroenteritisCherr NollNo ratings yet
- SECTION 02892 Traffic Signals Rev 0Document65 pagesSECTION 02892 Traffic Signals Rev 0Abdul HannanNo ratings yet
- HC SB 61 227Document22 pagesHC SB 61 227Hamed BarjestehNo ratings yet
- Comparitive Study of Pile Foundations With Foundations On Stone Column Treated Ground 170704090313Document23 pagesComparitive Study of Pile Foundations With Foundations On Stone Column Treated Ground 170704090313anurag hazarikaNo ratings yet
- Uas Semt Genap Fix BING XIDocument12 pagesUas Semt Genap Fix BING XISaepulloh KurniaNo ratings yet
- Boroscope Inspection Procedure 7th Stage StatorDocument15 pagesBoroscope Inspection Procedure 7th Stage StatorAPU SHOP BTH MS100% (2)
- Tolerance Chart: (Maximum Permissible Error)Document3 pagesTolerance Chart: (Maximum Permissible Error)arif_setyaw4nNo ratings yet
- ITCC in Riyadh Residential Complex J10-13300 16715-1 Voice & Data Communication CablingDocument16 pagesITCC in Riyadh Residential Complex J10-13300 16715-1 Voice & Data Communication CablinguddinnadeemNo ratings yet
- Potential Use of Probiotics: Ekachai ChukeatiroteDocument8 pagesPotential Use of Probiotics: Ekachai ChukeatiroteDanu EffendiNo ratings yet
- 1402AHS Prac Manual - 2023 - FINALDocument200 pages1402AHS Prac Manual - 2023 - FINALRuan BritsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsFrom EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsRating: 4.5 out of 5 stars4.5/5 (6)