You might also like
- The Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramFrom EverandThe Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramRating: 5 out of 5 stars5/5 (2)
- Formular Za Pristanak Na Cijepljenje Na FloridiDocument2 pagesFormular Za Pristanak Na Cijepljenje Na FloridiIndex.hrNo ratings yet
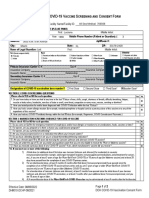
- DOH - Covid Vaccine Screening Consent FormDocument2 pagesDOH - Covid Vaccine Screening Consent FormCasey Feindt100% (1)
- Covid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 VaccineDocument2 pagesCovid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 Vaccinesiriamma wiliamsNo ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- Pfizer Screen Consent Form PrintDocument2 pagesPfizer Screen Consent Form Printp. wsmNo ratings yet
- FINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Document2 pagesFINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Natasa PrelevicNo ratings yet
- BivalentConsent MichaelBelen HAG322426Document2 pagesBivalentConsent MichaelBelen HAG322426michaeljohnbelen14No ratings yet
- CoehatiancreoleDocument1 pageCoehatiancreoleDonnaNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 pagesHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikNo ratings yet
- Informed Consent UniversalDocument1 pageInformed Consent Universalahasgahsg031No ratings yet
- Vaccination NoticeDocument2 pagesVaccination NoticeJulian Williams©™100% (2)
- Boosters Informed Consent Form ENGDocument1 pageBoosters Informed Consent Form ENGMoi ValdozNo ratings yet
- Vaccination Notice: Notice To Agent Is Notice To Principal Notice To Principal Is Notice To AgentDocument3 pagesVaccination Notice: Notice To Agent Is Notice To Principal Notice To Principal Is Notice To AgentOne HereNo ratings yet
- WA 2009 Certificate of ExemptionDocument1 pageWA 2009 Certificate of ExemptionDonnaNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- ParcfDocument8 pagesParcfGoogool YNo ratings yet
- REV - Outpatient Claim Form - AIADocument2 pagesREV - Outpatient Claim Form - AIAYen SylvaniNo ratings yet
- Pfizer Consent Form - FillableDocument8 pagesPfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.No ratings yet
- Hospitalization Reimbursment Claim FormDocument4 pagesHospitalization Reimbursment Claim FormFarhan aliNo ratings yet
- Pfizer Informed Consent Form Eng - April 15 2021Document1 pagePfizer Informed Consent Form Eng - April 15 2021Christie ConalesNo ratings yet
- Congvax Consent FormDocument3 pagesCongvax Consent FormRico MaligayaNo ratings yet
- REV - Inpatient Claim Form - AIADocument2 pagesREV - Inpatient Claim Form - AIAYen SylvaniNo ratings yet
- Consent Form (Sinovac)Document1 pageConsent Form (Sinovac)Kresta BenignoNo ratings yet
- Moderna Informed Consent Form Eng June 18 2021Document1 pageModerna Informed Consent Form Eng June 18 2021Bruce GonzalesNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineJohn BNo ratings yet
- (ASTRAZENECA) Informed Consent Form - Eng March 5 2021Document1 page(ASTRAZENECA) Informed Consent Form - Eng March 5 2021Mara Ozoa VillaroyaNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineBelle Alaba - RabiaNo ratings yet
- Parental Consent Form-EnGDocument2 pagesParental Consent Form-EnGMyrna ParasNo ratings yet
- Pfizer (Informed Consent Form) Eng - April 15 2021Document1 pagePfizer (Informed Consent Form) Eng - April 15 2021aleiah jean libatiqueNo ratings yet
- YL Camping Consent and Health FormDocument4 pagesYL Camping Consent and Health Formmcronin1970No ratings yet
- UKHSA COVID 19 Consent Form CYPDocument1 pageUKHSA COVID 19 Consent Form CYPPaula BurogNo ratings yet
- (SINOVAC) Informed Consent Form - Eng March 5 2021Document1 page(SINOVAC) Informed Consent Form - Eng March 5 2021Mark Anthony RosasNo ratings yet
- Covid Vaccine Clover Form2948Document1 pageCovid Vaccine Clover Form2948marian2277No ratings yet
- PEDIA Informed Consent Form PfizerDocument2 pagesPEDIA Informed Consent Form PfizerBalba ChrislynNo ratings yet
- Phil HealthDocument26 pagesPhil HealthliliposhianNo ratings yet
- Joint Waiver On Covid-19 VaccinationDocument3 pagesJoint Waiver On Covid-19 VaccinationAlexanderNo ratings yet
- Affidavit of Vaccine Adverse EffectDocument4 pagesAffidavit of Vaccine Adverse EffectRichard BalaisNo ratings yet
- Registration and Consent Form For Covid 19 Vaccination 05.03.21Document4 pagesRegistration and Consent Form For Covid 19 Vaccination 05.03.21Yash HardowarNo ratings yet
- Flu Consent FormDocument2 pagesFlu Consent FormTiger Palm TigerNo ratings yet
- COVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataDocument2 pagesCOVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataMaimoon AliNo ratings yet
- Vaccination Notice Affidavit: Mother and Father of - NAME - I/ or My ChildDocument2 pagesVaccination Notice Affidavit: Mother and Father of - NAME - I/ or My ChildMatthew McClusterNo ratings yet
- (Informed Consent) Covid-19 Vaccine Forms EngDocument1 page(Informed Consent) Covid-19 Vaccine Forms EngYosh PamatmatNo ratings yet
- Bupa Medical Declaration FormDocument1 pageBupa Medical Declaration FormMhedz agaoNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- COVID Vaccination Packet SFODocument16 pagesCOVID Vaccination Packet SFOferNo ratings yet
- Eligibility Declaration Form: COVID-19 Vaccine RolloutDocument4 pagesEligibility Declaration Form: COVID-19 Vaccine RolloutMoey AwadNo ratings yet
- COVID Immunization Record Correction RequestDocument1 pageCOVID Immunization Record Correction RequestNBC 10 WJAR50% (2)
- D - Vaccination Minor Consent FormDocument2 pagesD - Vaccination Minor Consent FormNoemi CamberosNo ratings yet
- Medical Claims Authorisation Form (Single Institution) : A - Particulars of PatientDocument2 pagesMedical Claims Authorisation Form (Single Institution) : A - Particulars of PatientArthur YeungNo ratings yet
- Covid19 WaiverDocument1 pageCovid19 WaiverSamiNo ratings yet
- COVD 19 Vaction Form 2020 Pfizerv2Document1 pageCOVD 19 Vaction Form 2020 Pfizerv2Neel YoyoNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- Protecting Yourself During A Pandemic : Step By Step Self-Care Guide: Step By Step Self-Care GuideFrom EverandProtecting Yourself During A Pandemic : Step By Step Self-Care Guide: Step By Step Self-Care GuideNo ratings yet
- Handbook of Child and Adolescent Drug and Substance Abuse: Pharmacological, Developmental, and Clinical ConsiderationsFrom EverandHandbook of Child and Adolescent Drug and Substance Abuse: Pharmacological, Developmental, and Clinical ConsiderationsNo ratings yet
- Plague 2.0 - Surviving the 2020 Coronavirus Pandemic (SARS-CoV 2, COVID-19 Edition)From EverandPlague 2.0 - Surviving the 2020 Coronavirus Pandemic (SARS-CoV 2, COVID-19 Edition)Rating: 1.5 out of 5 stars1.5/5 (5)
- ??? NP 2 Set A ???Document17 pages??? NP 2 Set A ???Elizabella Henrietta TanaquilNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsAdarsh RajNo ratings yet
- Covid 3Document5 pagesCovid 3api-559328651No ratings yet
- Moderna COVID-19 Vaccine: BasicsDocument2 pagesModerna COVID-19 Vaccine: BasicsCanoa TrailNo ratings yet
- Kolathur Initial LatestDocument213 pagesKolathur Initial LatestMathivanan AnbazhaganNo ratings yet
- Lesson 4Document11 pagesLesson 4Cabdullahi maxamed xussenNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsK1K5KNo ratings yet
- Kalamuddin 620459Document1 pageKalamuddin 620459Vikas KumarNo ratings yet
- Vaccines 10 00472Document17 pagesVaccines 10 00472IdmNo ratings yet
- Vaccination CertificateDocument1 pageVaccination CertificateKishore RNo ratings yet
- CertificateDocument1 pageCertificatechinni kumarNo ratings yet
- Masterlist Learners Covid 19 Vaccination Status Four AgilaDocument3 pagesMasterlist Learners Covid 19 Vaccination Status Four Agilajaze chavezNo ratings yet
- Dignity HepB Declination FormDocument1 pageDignity HepB Declination FormClarissa ShenahNo ratings yet
- COVID VaccinationDocument1 pageCOVID Vaccinationsoma mondalNo ratings yet
- EUA Astrazeneca WebsiteDocument4 pagesEUA Astrazeneca WebsiteMahealani SaligumbaNo ratings yet
- September 2021 Monthly Reporting ToolDocument19 pagesSeptember 2021 Monthly Reporting ToolChuchai BaliliNo ratings yet
- Urn Uvci 01 Ro 319x0l246gozo5854mnpemvy78wkqr#8Document2 pagesUrn Uvci 01 Ro 319x0l246gozo5854mnpemvy78wkqr#8Diana IscolniiNo ratings yet
- Persuasive SpeechDocument2 pagesPersuasive SpeechRonn ArtajoNo ratings yet
- 10 Reporting Formats HP Oct2017Document65 pages10 Reporting Formats HP Oct2017Devendra Singh Tomar100% (1)
- Rabies GuidelinesDocument21 pagesRabies Guidelineslotski100% (2)
- NOVA Vaccines Calling The ShotsDocument7 pagesNOVA Vaccines Calling The Shotslu naeNo ratings yet
- D - Vaccination Minor Consent FormDocument2 pagesD - Vaccination Minor Consent FormNoemi CamberosNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsErid Wan RoseNo ratings yet
- Maine 130 - HP 635 Item 1Document2 pagesMaine 130 - HP 635 Item 1NEWS CENTER MaineNo ratings yet
- HII Coding Process GuideDocument3 pagesHII Coding Process GuidePrashanthPatroNo ratings yet
- Main - Vaccine Refrigerator Freezer Temperature Chart TemplateDocument1 pageMain - Vaccine Refrigerator Freezer Temperature Chart TemplateMaan SantiagoNo ratings yet
- Immunisation History Statement: This Individual Has Received All Required COVID-19 VaccinationsDocument2 pagesImmunisation History Statement: This Individual Has Received All Required COVID-19 VaccinationsRhonda McveighNo ratings yet
- Personal Estacion BosqueDocument22 pagesPersonal Estacion BosqueAdalberto CabreraNo ratings yet
- Vaccination CertificateDocument1 pageVaccination Certificatememoriesmm17No ratings yet
- Real-World Evidence Summary: Covid-19 Vaccine AstrazenecaDocument2 pagesReal-World Evidence Summary: Covid-19 Vaccine AstrazenecaDsmmNo ratings yet