You might also like
- Phlebotomy Study GuideDocument18 pagesPhlebotomy Study GuideAnastasiaNo ratings yet
- Risk For BleedingDocument2 pagesRisk For Bleedingmikebry72% (25)
- Fetal Therapy JournalDocument9 pagesFetal Therapy JournalHasna Dian PramestiNo ratings yet
- Prenatal Diagnosis of ThalassemiaDocument4 pagesPrenatal Diagnosis of Thalassemiakamrankhan46143No ratings yet
- Pregnancy in Patients With B-Thalassemia Intermedia: Outcome of Mothers and NewbornsDocument4 pagesPregnancy in Patients With B-Thalassemia Intermedia: Outcome of Mothers and NewbornsIlham RamadhanisNo ratings yet
- FTP PDFDocument4 pagesFTP PDFIzat FuadiNo ratings yet
- Pneumonia and Pregnancy Outcomes: A Nationwide Population-Based StudyDocument7 pagesPneumonia and Pregnancy Outcomes: A Nationwide Population-Based StudyAdrin Mahmuddin HarahapNo ratings yet
- Current Update On Recurrent Pregnancy LossDocument6 pagesCurrent Update On Recurrent Pregnancy Losssutomo sutomo100% (1)
- Received: 2 June 2017 Accepted: 6 October 2017Document36 pagesReceived: 2 June 2017 Accepted: 6 October 2017Mohammad Pino HakimNo ratings yet
- Maternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewDocument23 pagesMaternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewasfwegereNo ratings yet
- PND IndiaDocument11 pagesPND IndiasuryasivNo ratings yet
- Taiwanese Journal of Obstetrics & GynecologyDocument4 pagesTaiwanese Journal of Obstetrics & GynecologykiranaNo ratings yet
- App Acog 2012Document10 pagesApp Acog 2012jimedureyNo ratings yet
- Aust NZ J Obst Gynaeco - 2022 - Silveira - Placenta Accreta Spectrum We Can Do BetterDocument7 pagesAust NZ J Obst Gynaeco - 2022 - Silveira - Placenta Accreta Spectrum We Can Do BetterDrFeelgood WolfslandNo ratings yet
- Factors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaDocument8 pagesFactors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaIllona SaharaNo ratings yet
- Zhang 2019Document9 pagesZhang 2019Maria José MendiolaNo ratings yet
- Ijrm 9 009 PDFDocument6 pagesIjrm 9 009 PDFWahyu PermataNo ratings yet
- AbruptionDocument13 pagesAbruptionMauricio Lopez MejiaNo ratings yet
- Anemia-1Document15 pagesAnemia-1Intan Wahyu CahyaniNo ratings yet
- Cell Free Dna Acog 2012Document3 pagesCell Free Dna Acog 2012gs2710No ratings yet
- Masas AnexialesDocument17 pagesMasas AnexialesEdwin CalleNo ratings yet
- Pregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninDocument5 pagesPregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninMentari SetiawatiNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- Sirichotiyakul 2016Document5 pagesSirichotiyakul 2016Atul GargNo ratings yet
- Jurding 1Document8 pagesJurding 1Danis SharitaNo ratings yet
- Khan, Et Al. (2016) - Frequency and Risk Factors of Low Birth Weight in Term Pregnancy. Pakistan Journal of Medical Science, 32 (1), Pp. 138-142.Document5 pagesKhan, Et Al. (2016) - Frequency and Risk Factors of Low Birth Weight in Term Pregnancy. Pakistan Journal of Medical Science, 32 (1), Pp. 138-142.Adib FraNo ratings yet
- AbruptionDocument13 pagesAbruptionAnghelo Aldair Velásquez CarrilloNo ratings yet
- Fonc 11 803994Document13 pagesFonc 11 803994zahra abdurrazakNo ratings yet
- Is Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyDocument6 pagesIs Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyYessie ErNo ratings yet
- 176S Tuesday Posters Obstetrics & GynecologyDocument1 page176S Tuesday Posters Obstetrics & GynecologyJoseph BennettNo ratings yet
- Pi Is 0002937812001317Document7 pagesPi Is 0002937812001317harold.atmajaNo ratings yet
- Herrera 2017Document9 pagesHerrera 2017Bianca Maria PricopNo ratings yet
- Antenatal and Early Infant Predictors of Postnatal Growth in Rural Vietnam: A Prospective Cohort StudyDocument10 pagesAntenatal and Early Infant Predictors of Postnatal Growth in Rural Vietnam: A Prospective Cohort StudyKomala SariNo ratings yet
- Can Placental Growth Factor in Maternal Circulation Identify Fetuses With Placental Intrauterine Growth RestrictionDocument7 pagesCan Placental Growth Factor in Maternal Circulation Identify Fetuses With Placental Intrauterine Growth RestrictionagusNo ratings yet
- Original Article The Association of Bacterial Vaginosis and Preterm LaborDocument3 pagesOriginal Article The Association of Bacterial Vaginosis and Preterm LaborHarry ManuhutuNo ratings yet
- Morfologi PlasentaDocument6 pagesMorfologi PlasentayueldiNo ratings yet
- Female Sterilization by Tubal Ligation During C-Se PDFDocument5 pagesFemale Sterilization by Tubal Ligation During C-Se PDFYø KåiNo ratings yet
- PIIS2210778916303701Document2 pagesPIIS2210778916303701Fatimah AssagafNo ratings yet
- Wolf Et Al MultivitaminsDocument30 pagesWolf Et Al MultivitaminsAnonymous 2GBzrE3XNo ratings yet
- A Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthDocument5 pagesA Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthSarahí SosaNo ratings yet
- 8699 36053 1 PBDocument7 pages8699 36053 1 PBPatrick RamosNo ratings yet
- 33873-Article Text-121761-1-10-20170831Document6 pages33873-Article Text-121761-1-10-20170831AnggaNo ratings yet
- Jourdain (2018)Document13 pagesJourdain (2018)nam dinhNo ratings yet
- Intensive Dialysis and Pregnancy: Home HemodialysisDocument10 pagesIntensive Dialysis and Pregnancy: Home HemodialysisOctaria SaputraNo ratings yet
- Grinshpun Cohen Et Al 2015 Health ExpectationsDocument12 pagesGrinshpun Cohen Et Al 2015 Health ExpectationsmaneshaputraNo ratings yet
- Paper Cervical LenghtDocument30 pagesPaper Cervical LenghtDanTe D' WinchesterNo ratings yet
- Jurnal Abrupsio PlasentaDocument13 pagesJurnal Abrupsio Plasentaperussi pranadiptaNo ratings yet
- Vitamins and Perinatal Outcomes Among HIV-Negative Women in TanzaniaDocument9 pagesVitamins and Perinatal Outcomes Among HIV-Negative Women in TanzaniaEmma KomalasariNo ratings yet
- Comparative Analysis of Obstetrical Complications in Nepalese at Advanced Maternal AgeDocument4 pagesComparative Analysis of Obstetrical Complications in Nepalese at Advanced Maternal AgeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Low Primary Cesarean Rate and High VBAC Rate With Good Outcomes in An Amish Birthing CenterDocument8 pagesLow Primary Cesarean Rate and High VBAC Rate With Good Outcomes in An Amish Birthing CenterStefanichalisnia 96No ratings yet
- Placenta Accreta Is Associated With IVF Pregnancies: A Retrospective Chart ReviewDocument6 pagesPlacenta Accreta Is Associated With IVF Pregnancies: A Retrospective Chart ReviewGladstone AsadNo ratings yet
- Clinical Case 4-PGI MendezDocument5 pagesClinical Case 4-PGI MendezJoher MendezNo ratings yet
- Anaemia in Pregnancy Malaysia, APJCN2006 PDFDocument10 pagesAnaemia in Pregnancy Malaysia, APJCN2006 PDFAkhmal SidekNo ratings yet
- Sleep Position, Fetal Growth Restriction, And.10Document9 pagesSleep Position, Fetal Growth Restriction, And.10harold.atmajaNo ratings yet
- Jurnal ObsgynDocument11 pagesJurnal ObsgynVivie Tirany SoediroNo ratings yet
- Post Partum Maternal Morbidities and TheDocument102 pagesPost Partum Maternal Morbidities and TheBagusHibridaNo ratings yet
- Mothers With Hypertensive Disorders of Pregnancy Increased Risk of Periventricular Leukomalacia in Extremely Preterm or Extremely Low Birth Weight Infants A Propensity Score AnalysisDocument9 pagesMothers With Hypertensive Disorders of Pregnancy Increased Risk of Periventricular Leukomalacia in Extremely Preterm or Extremely Low Birth Weight Infants A Propensity Score Analysisnurt.wongNo ratings yet
- Journal of The National Cancer Center: A R T I C L e I N F o A B S T R A C TDocument8 pagesJournal of The National Cancer Center: A R T I C L e I N F o A B S T R A C TCirugia SolcaNo ratings yet
- Hyun Et Al. 2017 - Efficacy and Safety of TDF To Prevent MTCT of HBVDocument13 pagesHyun Et Al. 2017 - Efficacy and Safety of TDF To Prevent MTCT of HBVizvery.badNo ratings yet
- Shiozaki A JReprodImmunol 2011-89-133Document8 pagesShiozaki A JReprodImmunol 2011-89-133Anonymous Vw1G0CvafeNo ratings yet
- 2018 Early IUGR GUPTA JMFNM 1Document6 pages2018 Early IUGR GUPTA JMFNM 1Sidonia CatalinaNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Blood ComponentsDocument24 pagesBlood ComponentsNukematsu MawiNo ratings yet
- Blood Collection VialsDocument26 pagesBlood Collection VialsMunizah MunirNo ratings yet
- Patient Blood Management Guidelines Critical Care Quick Reference GuideDocument24 pagesPatient Blood Management Guidelines Critical Care Quick Reference GuideSyed Shahrul Naz SyedNo ratings yet
- BOX 17.4 NCP Postpartum HemorrhageDocument4 pagesBOX 17.4 NCP Postpartum HemorrhageJam AliNo ratings yet
- Kelompok 4 - Laporan Hasil Tugas IVDocument8 pagesKelompok 4 - Laporan Hasil Tugas IVYoshua Mayo AdiNo ratings yet
- تجميع اسئله الاخصائين 1Document36 pagesتجميع اسئله الاخصائين 1Osama BakheetNo ratings yet
- Intro. To Medtech AssignmentDocument8 pagesIntro. To Medtech AssignmentStephanie OlleroNo ratings yet
- Blood Component PreparationDocument24 pagesBlood Component PreparationLaiba ArshadNo ratings yet
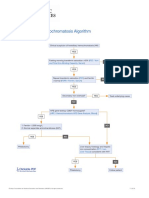
- Hereditary Hemochromatosis AlgorithmDocument1 pageHereditary Hemochromatosis AlgorithmS6b2No ratings yet
- Hematology 1 LeukemiaDocument140 pagesHematology 1 LeukemiamaryantoinetteriveraNo ratings yet
- S6 General Paper Mock Examinations 2019Document4 pagesS6 General Paper Mock Examinations 2019Kitooke Moses MutebiNo ratings yet
- Blood Bank and Blood TransfusionDocument11 pagesBlood Bank and Blood TransfusionMostafa Adel Ahmd100% (1)
- Practice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnDocument13 pagesPractice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnMadalina TalpauNo ratings yet
- 1-4 Hemostasis, Surgical Bleeding and TransfusionDocument17 pages1-4 Hemostasis, Surgical Bleeding and TransfusionRobin Tolentino100% (3)
- ReportDocument21 pagesReportmahhdyNo ratings yet
- HELLP SyndromeDocument8 pagesHELLP SyndromeFred OseiNo ratings yet
- Seeley's Ess9e.chapt11 - Lecture.aDocument43 pagesSeeley's Ess9e.chapt11 - Lecture.aJhara100% (2)
- Management of HemorrhageDocument11 pagesManagement of Hemorrhagemerin sunilNo ratings yet
- Isbb GuideDocument2 pagesIsbb GuidePaul Romil SumobayNo ratings yet
- Experiment Blood Composition and Blood Groups of Human by Iman Alisya 2K5Document5 pagesExperiment Blood Composition and Blood Groups of Human by Iman Alisya 2K5Iman AlisyaNo ratings yet
- Microcytic Hypochromic Anemia: - M QariDocument33 pagesMicrocytic Hypochromic Anemia: - M QarirohitNo ratings yet
- CASE REPORT COMPETITION With Identifying FeaturesDocument12 pagesCASE REPORT COMPETITION With Identifying FeaturesJoel Cesar AtinadoNo ratings yet
- Childrens FBC Reference Ranges PDFDocument1 pageChildrens FBC Reference Ranges PDFmfaddhilNo ratings yet
- 3 Hema 2 Laboratory Manual-Bleeding Time and Clotting TimeDocument5 pages3 Hema 2 Laboratory Manual-Bleeding Time and Clotting TimeJanielle FajardoNo ratings yet
- PBCC PDFDocument1 pagePBCC PDFMaureen Dela ResmaNo ratings yet
- Chapter 44: Nursing Care of The Client With An Hematologic DisordersDocument18 pagesChapter 44: Nursing Care of The Client With An Hematologic DisordersfLOR_ZIANE_MAENo ratings yet
- Non-Secretory Multiple Myeloma: Diagnosis and Management: Grzegorz Charliński, Artur JurczyszynDocument6 pagesNon-Secretory Multiple Myeloma: Diagnosis and Management: Grzegorz Charliński, Artur JurczyszynYosua Herling KumambongNo ratings yet
- Membrane Versus Centrifuge-Based Therapeutic Plasma Exchange, A Randomized Prospective Crossover StudyDocument6 pagesMembrane Versus Centrifuge-Based Therapeutic Plasma Exchange, A Randomized Prospective Crossover Studyalida romeroNo ratings yet