You might also like
- Role of IV Meropenem in Current EraDocument38 pagesRole of IV Meropenem in Current EraImtiyaz Alam SahilNo ratings yet
- Clinical Pharmaco Kinetics (TDM) (Clinical Pharmacy Fall-22 Sem-9)Document27 pagesClinical Pharmaco Kinetics (TDM) (Clinical Pharmacy Fall-22 Sem-9)Mehran RiazNo ratings yet
- PK-PD of Antimicrobial Therapy-Lecture12 Oct11Document37 pagesPK-PD of Antimicrobial Therapy-Lecture12 Oct11Idrissou FmsbNo ratings yet
- Pain Pocket GuideDocument2 pagesPain Pocket Guidebtalera100% (2)
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliDocument45 pagesTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsNo ratings yet
- Phenytoin Administration GuideDocument2 pagesPhenytoin Administration GuideNoorHaziqZ1926No ratings yet
- Case Study RVD TB With AnswersDocument5 pagesCase Study RVD TB With Answersadilah fazliNo ratings yet
- 107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2Document4 pages107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2ft84nzzc92No ratings yet
- AST and Dosing Info Card - FINALDocument2 pagesAST and Dosing Info Card - FINALGAYATHIRINo ratings yet
- Cardiology Doses: WhiteknightloveDocument3 pagesCardiology Doses: WhiteknightloveSelim TarekNo ratings yet
- Answers To Practice Problem Set #10Document3 pagesAnswers To Practice Problem Set #10Raju NiraulaNo ratings yet
- Calculation of DosesDocument27 pagesCalculation of DosesAhmad Radhya Dionanda100% (1)
- Pharmacokinetic Training Packet For PharmacistsDocument24 pagesPharmacokinetic Training Packet For PharmacistsGlory Claudia KarundengNo ratings yet
- General Principles of Antibiotic TherapyDocument44 pagesGeneral Principles of Antibiotic TherapyFadhly SharimanNo ratings yet
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocument8 pagesGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelNo ratings yet
- 1.13 Hyper-CVAD-MA Version 2.1Document5 pages1.13 Hyper-CVAD-MA Version 2.1Alina CrissNo ratings yet
- Bacterial Uti GuidelinesDocument2 pagesBacterial Uti Guidelinesnurul muamanah amalNo ratings yet
- Pharmacokinetic Exercises ListDocument5 pagesPharmacokinetic Exercises ListVijendra R100% (1)
- TDM Practical Guide Part1Document7 pagesTDM Practical Guide Part1Ahmedshaker21100% (1)
- Appendix 1: Chemotherapy ProtocolsDocument3 pagesAppendix 1: Chemotherapy ProtocolsImam Hakim SuryonoNo ratings yet
- 311 Topotecan Monotherapy 5 DayDocument4 pages311 Topotecan Monotherapy 5 DayRuxandra BănicăNo ratings yet
- Use of Aeds in 2011 and Beyond: Optimizing Clinical ManagementDocument32 pagesUse of Aeds in 2011 and Beyond: Optimizing Clinical ManagementchandanNo ratings yet
- Case 1Document8 pagesCase 1radhakishan.22phpp09No ratings yet
- Ozempic Dispensing Quick Reference Guide 2023-06-07Document2 pagesOzempic Dispensing Quick Reference Guide 2023-06-07Graham Thomas GipsonNo ratings yet
- Monte Carlo Simulation of Temocillin 6 G Daily Administered by Continuous Infusion or Intermittent DosageDocument2 pagesMonte Carlo Simulation of Temocillin 6 G Daily Administered by Continuous Infusion or Intermittent DosageAris DokoumetzidisNo ratings yet
- Us Bactroban OintmentDocument4 pagesUs Bactroban OintmentJayCee AriasNo ratings yet
- PGX - Others 2021 - 240118 - 070911Document54 pagesPGX - Others 2021 - 240118 - 070911Maryam HaniniNo ratings yet
- Aminogycoside AntibioticsDocument31 pagesAminogycoside AntibioticsNurul Febrina100% (2)
- Meperidin: Toxicity SummaryDocument11 pagesMeperidin: Toxicity SummaryrosaNo ratings yet
- DIS IPD Ceftriaxone KonsulDocument28 pagesDIS IPD Ceftriaxone KonsulTriana MaulidyahNo ratings yet
- SCI 8008SEF Medical Microbiology & Virology II Lecture 5 - OLEDocument52 pagesSCI 8008SEF Medical Microbiology & Virology II Lecture 5 - OLEYY CheungNo ratings yet
- Laboratory Diagnosis: 1. Cytological Examination (Tzanck Smear)Document11 pagesLaboratory Diagnosis: 1. Cytological Examination (Tzanck Smear)Rahma P T RambeyNo ratings yet
- Therapeutic Drug Monitoring: T H e R A P e U T I C T o X I CDocument22 pagesTherapeutic Drug Monitoring: T H e R A P e U T I C T o X I Ckavya nainitaNo ratings yet
- Clinical Calculations 1Document8 pagesClinical Calculations 1evacawleyNo ratings yet
- Data Sheet Mabthera: Pharmaceutical FormDocument42 pagesData Sheet Mabthera: Pharmaceutical FormHeba_Al_KhozaeNo ratings yet
- Tuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, VaccinationDocument44 pagesTuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, Vaccinationskeisham11No ratings yet
- Purixan (Mercaptopurine) - Drug: Nova Laboratories, LTDDocument7 pagesPurixan (Mercaptopurine) - Drug: Nova Laboratories, LTDsupandiNo ratings yet
- Purixan (Mercaptopurine) - Drug: Nova Laboratories, LTDDocument7 pagesPurixan (Mercaptopurine) - Drug: Nova Laboratories, LTDsupandiNo ratings yet
- Pediatric Dosage CalculationsDocument5 pagesPediatric Dosage CalculationsLovely Anjenell MacalingaNo ratings yet
- Antibiotic Pharmacokinetic MonitoringDocument5 pagesAntibiotic Pharmacokinetic MonitoringlucialNo ratings yet
- Clinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringDocument11 pagesClinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringFate ChanNo ratings yet
- Management of Status Epilepticus 2022Document8 pagesManagement of Status Epilepticus 2022albert siraitNo ratings yet
- Prof Henny Lucida PHD Apt Calculation of DosespptDocument27 pagesProf Henny Lucida PHD Apt Calculation of DosespptWella CitraersyaNo ratings yet
- L 51 R Hypercvad R MaDocument7 pagesL 51 R Hypercvad R MaMohamed MahmoudNo ratings yet
- JDH Pocket Pain GuideDocument2 pagesJDH Pocket Pain Guidesgod34100% (1)
- SMILEPEG HEM TCell ADocument5 pagesSMILEPEG HEM TCell Aphillip.chung89No ratings yet
- Aminoglycoside Dosage Adjustment - Group 4Document27 pagesAminoglycoside Dosage Adjustment - Group 4katrinNo ratings yet
- Abstract and IntroductionDocument6 pagesAbstract and IntroductionIngrid94HannaNo ratings yet
- Ivermectin (For COVID) V21July2021 (AHS) (Jarir at Thobari) PAKAIDocument30 pagesIvermectin (For COVID) V21July2021 (AHS) (Jarir at Thobari) PAKAItasialalalaNo ratings yet
- LPD - Magnocef (Final)Document38 pagesLPD - Magnocef (Final)NARESH JANDIALNo ratings yet
- Premedication: Presenter-Dr - Srishti Moderator-Dr.R.Pal (Professor) Dr.P. Jain (Associate Professor)Document34 pagesPremedication: Presenter-Dr - Srishti Moderator-Dr.R.Pal (Professor) Dr.P. Jain (Associate Professor)Viresh Upase Roll No 130. / 8th termNo ratings yet
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument11 pagesSummary of Product Characteristics: 4.1 Therapeutic IndicationsAninditaSahaNo ratings yet
- Optimizing Aminoglycosideuse: William A. CraigDocument15 pagesOptimizing Aminoglycosideuse: William A. CraigSurya BhupatirajuNo ratings yet
- DetoxDocument4 pagesDetoxShahrul Nizan HashimNo ratings yet
- Vancomycin: Group 5 R.M 2Document31 pagesVancomycin: Group 5 R.M 2vi_wiviaNo ratings yet
- McCormack Et Al-1997-Pharmacotherapy - The Journal of Human Pharmacology and Drug TherapyDocument3 pagesMcCormack Et Al-1997-Pharmacotherapy - The Journal of Human Pharmacology and Drug TherapyilexdeciduaNo ratings yet
- 05 IV Induction Agents PDFDocument0 pages05 IV Induction Agents PDFjuniorebinda100% (1)
- Cisplatin-Pemetrexed (NSCLC)Document5 pagesCisplatin-Pemetrexed (NSCLC)Sindu SankarNo ratings yet
- Drug Food InteractionsDocument2 pagesDrug Food Interactionsbala murugan100% (1)
- Drug-Food Interactions 2008Document6 pagesDrug-Food Interactions 2008bala muruganNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
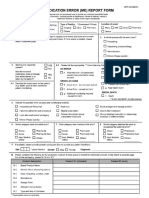
- Medication Error Report FormDocument2 pagesMedication Error Report Formbala muruganNo ratings yet
- FOLLOW UP FORM Pharmacy StudentsDocument2 pagesFOLLOW UP FORM Pharmacy Studentsbala muruganNo ratings yet
- Cefepime Protocol Detail June 2016 UpdateDocument6 pagesCefepime Protocol Detail June 2016 UpdateSuvrankar DattaNo ratings yet
- Pharmaceutical Care Patient Record Kmchcopnew PDFDocument18 pagesPharmaceutical Care Patient Record Kmchcopnew PDFbala muruganNo ratings yet
- Pharmaceutical Care Patient Record Kmchcopnew PDFDocument18 pagesPharmaceutical Care Patient Record Kmchcopnew PDFbala muruganNo ratings yet
- Pharmaceutical Care Patient RecordDocument17 pagesPharmaceutical Care Patient Recordbala muruganNo ratings yet
- Nutriflex Lipid Peri PDFDocument2 pagesNutriflex Lipid Peri PDFSanjaya FaisalNo ratings yet
- First Year Health Guide Acetaminophen Chart PDFDocument1 pageFirst Year Health Guide Acetaminophen Chart PDFnobeauNo ratings yet
- Dr. PHilip Chancellors Handbook of Bach Flower RemediesDocument256 pagesDr. PHilip Chancellors Handbook of Bach Flower Remediesamishcar100% (11)
- Evrenzo-Spc enDocument51 pagesEvrenzo-Spc enlamprinilNo ratings yet
- POWDERSDocument26 pagesPOWDERSALIMAH MOSARWANo ratings yet
- Ministry of Public Health - News DetailsDocument1 pageMinistry of Public Health - News DetailsQatar Pride 2022No ratings yet
- Mag NMM022009Document60 pagesMag NMM022009DanceportugalNo ratings yet
- CHEG332 Kinetics PBPK Oct27 F16 SakaiDocument49 pagesCHEG332 Kinetics PBPK Oct27 F16 SakaiCyrus CaoNo ratings yet
- Aefi Cek ListDocument2 pagesAefi Cek ListteukuthaibNo ratings yet
- PCNE Classification Scheme For Drug-Related Problems V8.02 - Page 1Document5 pagesPCNE Classification Scheme For Drug-Related Problems V8.02 - Page 1Divaa Amadea NabillaNo ratings yet
- Guidelines On Seventh Day Automatic Stop OrderDocument3 pagesGuidelines On Seventh Day Automatic Stop OrderJohnny Dee100% (2)
- DR 100e (English - Brochure)Document5 pagesDR 100e (English - Brochure)1994mjncNo ratings yet
- WHO Guidelines On Clinical Evaluation of Vaccines (Clinical - Changes - IK - Final)Document92 pagesWHO Guidelines On Clinical Evaluation of Vaccines (Clinical - Changes - IK - Final)Slim JimNo ratings yet
- Glossary of Terms and Symbols Used in PharmacologyDocument55 pagesGlossary of Terms and Symbols Used in Pharmacologykriss WongNo ratings yet
- Alberts Principles and Practice of Ophthalmology - Volume II PDFDocument1,373 pagesAlberts Principles and Practice of Ophthalmology - Volume II PDFPrep Neet PG100% (3)
- Pelvis Lab 1 1Document13 pagesPelvis Lab 1 1api-632146706No ratings yet
- Metronidazole AFTinfDocument8 pagesMetronidazole AFTinfSmartishag BediakoNo ratings yet
- Vichinsky Et Al.2019Document11 pagesVichinsky Et Al.2019Kuliah Semester 4No ratings yet
- Cleaning Validation and Its Importance in Pharmaceutical IndustryDocument6 pagesCleaning Validation and Its Importance in Pharmaceutical IndustryRakeshNo ratings yet
- Pharmaco KineticsDocument427 pagesPharmaco KineticsMehrdad AvestaNo ratings yet
- Formulation and Evaluation of Domperidone Candy LozengesDocument9 pagesFormulation and Evaluation of Domperidone Candy LozengeskbnarkhedeNo ratings yet
- Fistula THDocument3 pagesFistula THKatarina SimicicNo ratings yet
- Baste RRL Research VetDocument6 pagesBaste RRL Research VetSebastian Carlo CabiadesNo ratings yet
- NovorapidDocument16 pagesNovorapidRADITA MAULASARINo ratings yet
- FAQCo WINforcitizensDocument5 pagesFAQCo WINforcitizensRaj AgrawalNo ratings yet
- Low Molecular Weight Heparins Summary Prescribing Guide Version 1.3Document14 pagesLow Molecular Weight Heparins Summary Prescribing Guide Version 1.3sharief145No ratings yet
- Basic Principles Practice QuestionsDocument10 pagesBasic Principles Practice QuestionsLayo Fatola100% (1)
- Pharma CaluculationsDocument5 pagesPharma CaluculationsAnish Kumar ANo ratings yet
- 5 Benefits and Uses of FrankincenseDocument2 pages5 Benefits and Uses of FrankincenseABDULKARIM HAJI YOUSUFNo ratings yet
- Cyanocobalamin Injection Clinical Pharmacology Drug MonographDocument36 pagesCyanocobalamin Injection Clinical Pharmacology Drug MonographLaureyNo ratings yet