You might also like
- African American Slave MedicineDocument217 pagesAfrican American Slave MedicineSah Ara SAnkh Sanu-t100% (19)
- 03 PsoriasisDocument28 pages03 PsoriasisGlen Lester ChiongNo ratings yet
- Investigating Asphyxial DeathsDocument51 pagesInvestigating Asphyxial DeathsVincentius Novian Romilio50% (2)
- ACLS For TachycardiaDocument31 pagesACLS For TachycardiaTausif HaqueNo ratings yet
- Hypertrophic CardiomyopathyDocument37 pagesHypertrophic CardiomyopathyMarko Vukovic100% (1)
- Jalt13i1p63 PDFDocument3 pagesJalt13i1p63 PDFBoţu AlexandruNo ratings yet
- Time To Synergize Mental Health With Brain Health: CommentDocument3 pagesTime To Synergize Mental Health With Brain Health: Commentsoliveira_149796No ratings yet
- KP 2.3.1.6Document42 pagesKP 2.3.1.6Taufiqurrahman HabibNo ratings yet
- K7 - Penyakit Jantung Katub-ANNDocument38 pagesK7 - Penyakit Jantung Katub-ANNXeniel AlastairNo ratings yet
- Valvular heart disease diagnosis and treatmentDocument38 pagesValvular heart disease diagnosis and treatmentDumora FatmaNo ratings yet
- Mitral Stenosis and Regurgitation: Etiology, Symptoms, Exam, and ManagementDocument85 pagesMitral Stenosis and Regurgitation: Etiology, Symptoms, Exam, and ManagementWilliam Lie100% (2)
- Congenital Heart Disease-2Document57 pagesCongenital Heart Disease-2Deepika LamichhaneNo ratings yet
- VHD Inter FinalDocument84 pagesVHD Inter Finalfitrah fajrianiNo ratings yet
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Document51 pagesDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Valvular Heart Disease: Hakim AlkatiriDocument84 pagesValvular Heart Disease: Hakim AlkatiriFNo ratings yet
- Mitral Stenosis Etiology and TreatmentDocument19 pagesMitral Stenosis Etiology and TreatmentAdi TrisnoNo ratings yet
- Mitral Regurgitation: MedicineDocument7 pagesMitral Regurgitation: Medicineapi-3829364No ratings yet
- ECG Arrhythmia Classification GuideDocument6 pagesECG Arrhythmia Classification GuideEzzat SalemNo ratings yet
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Aortic StenosisDocument8 pagesAortic Stenosisdr.moni.co.ukNo ratings yet
- Wk7 PLP Cardiovascular Disorder Part 1,2,3,4Document210 pagesWk7 PLP Cardiovascular Disorder Part 1,2,3,4claire yowsNo ratings yet
- Valvular Heart Diseases: Causes, Symptoms, and TreatmentDocument32 pagesValvular Heart Diseases: Causes, Symptoms, and TreatmentChrystel Mae PañaresNo ratings yet
- Mitral Stenosis For Beginners: Pratap Sagar TiwariDocument23 pagesMitral Stenosis For Beginners: Pratap Sagar TiwariMituran IshwarNo ratings yet
- Aortic Stenosis and Regurgitation GuideDocument3 pagesAortic Stenosis and Regurgitation GuideAndrassy Twinkle AlineaNo ratings yet
- Aortic StenosisDocument70 pagesAortic Stenosisroseneels9No ratings yet
- Pericardial Disease: Adel Hasanin Ahmed 1Document5 pagesPericardial Disease: Adel Hasanin Ahmed 1Shaz ChindhyNo ratings yet
- Valvular UpdateDocument44 pagesValvular UpdateUlmi FadillahNo ratings yet
- Rheumatic Heart DiseaseDocument35 pagesRheumatic Heart DiseaseSAYMABANUNo ratings yet
- Cardiology Notes by Wasim AhmadDocument28 pagesCardiology Notes by Wasim AhmadAshna moeenNo ratings yet
- ECG AbnormalDocument60 pagesECG Abnormalvidishmalaviya300No ratings yet
- PE of Common CVSDocument105 pagesPE of Common CVSKaushal RudaniNo ratings yet
- Kelompok 14 Skenario 2Document11 pagesKelompok 14 Skenario 2Rachmad SammuliaNo ratings yet
- Valvular Heart Disease: Joko AnggoroDocument53 pagesValvular Heart Disease: Joko AnggoroReza SatriaNo ratings yet
- Penyakit Jantung KatupDocument35 pagesPenyakit Jantung Katupdwi ariskaNo ratings yet
- Pemicu 6 Eko Blok KGDDocument128 pagesPemicu 6 Eko Blok KGDEko SiswantoNo ratings yet
- Valvular Heart Disease and Anesthesia Considerations for Non-Cardiac SurgeryDocument44 pagesValvular Heart Disease and Anesthesia Considerations for Non-Cardiac SurgeryLakshmi YalavarthyNo ratings yet
- Valvular Heart DiseaseDocument5 pagesValvular Heart DiseaseElyas MehdarNo ratings yet
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminNo ratings yet
- HF Management GuideDocument49 pagesHF Management GuideJabraan Jamil100% (1)
- ECG Findings in Marathon Runner with AIVRDocument24 pagesECG Findings in Marathon Runner with AIVRmohamedsmnNo ratings yet
- 4 Valvular Heart Disease#36f7Document40 pages4 Valvular Heart Disease#36f7Natasha LiberisNo ratings yet
- Aortic Regurgitation: Causes, Symptoms, and TreatmentDocument12 pagesAortic Regurgitation: Causes, Symptoms, and TreatmentSanjeet SahNo ratings yet
- Cardiovascular Exam: Examination Includes The FollowingDocument37 pagesCardiovascular Exam: Examination Includes The FollowingyayayanizaNo ratings yet
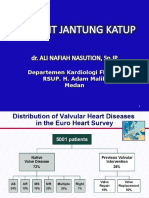
- DR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanDocument46 pagesDR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanAziz DjohariNo ratings yet
- Systolic Dysfunction:: Types of Heart FailureDocument13 pagesSystolic Dysfunction:: Types of Heart FailureElisabeth F. OjhaNo ratings yet
- CHF and CardiomyopathiesDocument8 pagesCHF and CardiomyopathiesDan HoNo ratings yet
- RHEUMATIC HEART DISEASE GUIDEDocument30 pagesRHEUMATIC HEART DISEASE GUIDEDhiraj PantNo ratings yet
- Valvular Heart DiseaseDocument73 pagesValvular Heart Diseaseindia2puppy100% (4)
- Heart NewDocument27 pagesHeart NewGomathi ShankarNo ratings yet
- Congestive Heart Failure: 10 July 2013Document8 pagesCongestive Heart Failure: 10 July 2013Michelle Vera GabunNo ratings yet
- Pericardial Diseases 3rd Yr BMTDocument38 pagesPericardial Diseases 3rd Yr BMT211941103014100% (1)
- Valvular Heart Disease. KulDocument67 pagesValvular Heart Disease. KulDebyAntatifaniRitongaNo ratings yet
- Abnormal Pulse FindingsDocument43 pagesAbnormal Pulse FindingsAngelo LacisteNo ratings yet
- Cardiomyopathy Dilated CardiomyopathyDocument5 pagesCardiomyopathy Dilated Cardiomyopathym3d1k100% (1)
- Valvular Heart Disease: Mitral Stenosis, Mitral Regurgitation, Aortic StenosisDocument79 pagesValvular Heart Disease: Mitral Stenosis, Mitral Regurgitation, Aortic StenosisDumora FatmaNo ratings yet
- (K7) Valvular Heart DiseaseDocument79 pages(K7) Valvular Heart DiseaseXeniel AlastairNo ratings yet
- Aortic Stenosis - LecturioDocument13 pagesAortic Stenosis - Lecturiokujtimepira2No ratings yet
- ECG - Dilated HypertrophiedDocument19 pagesECG - Dilated Hypertrophiedyusuf fathoniNo ratings yet
- 5 Pericarditis and Its Complications ICMPDDocument22 pages5 Pericarditis and Its Complications ICMPDmus zaharaNo ratings yet
- Understanding Congenital Heart DiseaseDocument54 pagesUnderstanding Congenital Heart DiseaseYemata HailuNo ratings yet
- Right Ventricular Myocardial InfarctionDocument43 pagesRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- Kuliah MITRAL STENOSISDocument19 pagesKuliah MITRAL STENOSISekaseptiani312No ratings yet
- Aortic Regurgitation by DR DilmoDocument37 pagesAortic Regurgitation by DR Dilmosinan kNo ratings yet
- Fitz Cardiology Paces NotesDocument26 pagesFitz Cardiology Paces NotesMuhammad BilalNo ratings yet
- CH 13Document22 pagesCH 13Boţu AlexandruNo ratings yet
- CH 7Document30 pagesCH 7Boţu AlexandruNo ratings yet
- PrefaceDocument2 pagesPrefaceBoţu AlexandruNo ratings yet
- BiologyDocument1 pageBiologyMaria StancuNo ratings yet
- CH 9Document18 pagesCH 9Boţu AlexandruNo ratings yet
- CH 5Document18 pagesCH 5Boţu AlexandruNo ratings yet
- Spanzurare PDFDocument7 pagesSpanzurare PDFBoţu AlexandruNo ratings yet
- Simpson's ForensicDocument264 pagesSimpson's ForensicEllagEsz100% (3)
- Promotional Booklet - Text Book - With Front and Back Cover - Corrected PDFDocument35 pagesPromotional Booklet - Text Book - With Front and Back Cover - Corrected PDFBoţu AlexandruNo ratings yet
- A Rareposition in Partial Hanging - A Case ReportDocument4 pagesA Rareposition in Partial Hanging - A Case ReportBoţu AlexandruNo ratings yet
- CH 6Document16 pagesCH 6Boţu AlexandruNo ratings yet
- CH 4Document22 pagesCH 4Boţu AlexandruNo ratings yet
- Ligature Strangulation - StudentsDocument28 pagesLigature Strangulation - StudentsBoţu Alexandru100% (1)
- Curs 5 Urgente in Cardiologie Anul VI Seriile A B C DDocument23 pagesCurs 5 Urgente in Cardiologie Anul VI Seriile A B C DBoţu AlexandruNo ratings yet
- Prof 2819 PDFDocument6 pagesProf 2819 PDFBoţu AlexandruNo ratings yet
- Strangulation Assessment Evidence Collection and Documentation PDFDocument36 pagesStrangulation Assessment Evidence Collection and Documentation PDFBoţu AlexandruNo ratings yet
- Jbct14i1p32 PDFDocument4 pagesJbct14i1p32 PDFBoţu AlexandruNo ratings yet
- Ecr2011 C-1846 PDFDocument17 pagesEcr2011 C-1846 PDFBoţu AlexandruNo ratings yet
- Delayed Death in Hanging 2157 7145.S1 001Document2 pagesDelayed Death in Hanging 2157 7145.S1 001Aray Al-AfiqahNo ratings yet
- B9 PP PDFDocument46 pagesB9 PP PDFBoţu AlexandruNo ratings yet
- DeathbyStrangulation DR - DeanhawleyDocument9 pagesDeathbyStrangulation DR - DeanhawleybaetyNo ratings yet
- 0bdc PDFDocument4 pages0bdc PDFBoţu AlexandruNo ratings yet
- Introduction To Forensic Science Lecture 5 Forensic PathologyDocument89 pagesIntroduction To Forensic Science Lecture 5 Forensic PathologyBoţu Alexandru100% (4)
- Article1393596338 - Dhiab Et Al PDFDocument5 pagesArticle1393596338 - Dhiab Et Al PDFBoţu AlexandruNo ratings yet
- 1 PB PDFDocument3 pages1 PB PDFBoţu AlexandruNo ratings yet
- NCM 106 - Pharmacology Principles of Medication AdministrationDocument10 pagesNCM 106 - Pharmacology Principles of Medication AdministrationEarl BenedictNo ratings yet
- Angiogenesis in CancerDocument4 pagesAngiogenesis in CanceranonymousNo ratings yet
- Echelon Revision Casestudies 71380632Document16 pagesEchelon Revision Casestudies 71380632Dipen ShahNo ratings yet
- Artificial HeartDocument17 pagesArtificial HeartRAKESHKANNAN100% (1)
- PharmNotesDocument210 pagesPharmNoteschiragvetsNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaDeasy Arindi PutriNo ratings yet
- Annotated BibDocument19 pagesAnnotated Bibapi-252208553No ratings yet
- MH Case Study Fall 2021Document10 pagesMH Case Study Fall 2021api-593123385No ratings yet
- Drug Study 7th Floor Ucmed RotationDocument6 pagesDrug Study 7th Floor Ucmed RotationVinz OñoNo ratings yet
- IDAO - TYPOLOGY 1st & 2nd ASSESSMENTDocument2 pagesIDAO - TYPOLOGY 1st & 2nd ASSESSMENTJingjing BelanoNo ratings yet
- Lingkar Pinggang-Pinggul Dengan PJKDocument10 pagesLingkar Pinggang-Pinggul Dengan PJKDjoko SutopoNo ratings yet
- Tumors of The Jaw and Oral MucosaDocument18 pagesTumors of The Jaw and Oral MucosaDaniela LeonteNo ratings yet
- NURS FPX 5003 Assessment 3 Intervention and Health Promotion Plan for Diverse PopulationDocument6 pagesNURS FPX 5003 Assessment 3 Intervention and Health Promotion Plan for Diverse PopulationCarolyn HarkerNo ratings yet
- Obstetrics AclsDocument6 pagesObstetrics AclsPedro BurgosNo ratings yet
- Dialogue Unit 8: Example of A DialogueDocument4 pagesDialogue Unit 8: Example of A DialogueIsfaNo ratings yet
- Sun 800 RoidRage Innovative Trends Treatment Male HypogonadismDocument19 pagesSun 800 RoidRage Innovative Trends Treatment Male HypogonadismM. Sz.No ratings yet
- MID Bacteria Charts JkuoDocument17 pagesMID Bacteria Charts Jkuotsukino143100% (2)
- Explaining StrokeDocument16 pagesExplaining StrokeAhmed GaberNo ratings yet
- The Montgomery Borgatta Caregiver Burden ScaleDocument22 pagesThe Montgomery Borgatta Caregiver Burden ScalehjhjkNo ratings yet
- Renal PhysiologyDocument5 pagesRenal PhysiologyJayricDepalobosNo ratings yet
- Clinical Trial Using A Silver-Coated Screw-Rod System and One-Year Follow-Up of The First 50 PatientsDocument12 pagesClinical Trial Using A Silver-Coated Screw-Rod System and One-Year Follow-Up of The First 50 Patientsguugle gogleNo ratings yet
- NCM 107 Vital SignsDocument5 pagesNCM 107 Vital SignsVillanueva, Alwyn Shem T.No ratings yet
- Donna Eveline Prisca Panduu 1061050030 Pembimbing: Dr. Karyadi Prayanangga, SP - AnDocument20 pagesDonna Eveline Prisca Panduu 1061050030 Pembimbing: Dr. Karyadi Prayanangga, SP - AndonnaevelineNo ratings yet
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- Intake AssessmentDocument2 pagesIntake Assessmentyourzxtruly0% (1)
- Fogsi ChecklistDocument131 pagesFogsi ChecklistParimi VinodNo ratings yet
- Shigella SPP, Vibrio SPPDocument6 pagesShigella SPP, Vibrio SPPtomal7811islamNo ratings yet
- Chapter22 PregnancyDocument38 pagesChapter22 PregnancyAnnie Grace VillanuevaNo ratings yet