You might also like
- Biomaterials (BIOL 1120) Professor Beth Zielinski Professor Jeffrey R. Scott Jacqueline Chang Timothy ChouDocument12 pagesBiomaterials (BIOL 1120) Professor Beth Zielinski Professor Jeffrey R. Scott Jacqueline Chang Timothy Choukuy thanNo ratings yet
- Knee Replacement Surgery, A Simple Guide To The Procedure And Related ConditionsFrom EverandKnee Replacement Surgery, A Simple Guide To The Procedure And Related ConditionsNo ratings yet
- Presentation OsteotomyDocument20 pagesPresentation OsteotomyArijit ChowdhuryNo ratings yet
- Esophageal CancerDocument23 pagesEsophageal Cancerabhandlung100% (3)
- NeonatalresuscitationDocument67 pagesNeonatalresuscitationfidaNo ratings yet
- Visual PathwayDocument39 pagesVisual Pathwayhuman anatomyNo ratings yet
- Fracture Shaft FemurDocument39 pagesFracture Shaft FemurDwityaOktinaDewi100% (1)
- Rigid Internal FixationDocument72 pagesRigid Internal FixationDR NASIMNo ratings yet
- ATLS Practice Test 3 Answers & ExplanationsDocument10 pagesATLS Practice Test 3 Answers & ExplanationsCarl Sars50% (2)
- Surgical OrthodonticsDocument4 pagesSurgical OrthodonticsFernaz Behlim100% (2)
- Clinical Cases in Restorative and Reconstructive DentistryFrom EverandClinical Cases in Restorative and Reconstructive DentistryRating: 5 out of 5 stars5/5 (1)
- Exstrophy-Epispadias Complex: Current Management: Journal ReadingDocument64 pagesExstrophy-Epispadias Complex: Current Management: Journal ReadingAnonymous ce3S6XFdwU100% (1)
- Seminar 1 Sutures and TechniquesDocument71 pagesSeminar 1 Sutures and TechniquesAnoop John100% (1)
- A Restorative Approach To Glaucoma: Helping The World See ClearlyDocument12 pagesA Restorative Approach To Glaucoma: Helping The World See ClearlyHaag-Streit UK (HS-UK)No ratings yet
- Limb Salvage Surgery in Bone MalignanciesDocument56 pagesLimb Salvage Surgery in Bone MalignanciesKyaw SwaNo ratings yet
- Early Experience of Femoral Neck Fractures Treated Surgically With Femoral Neck System'Document38 pagesEarly Experience of Femoral Neck Fractures Treated Surgically With Femoral Neck System'Amit SinhaNo ratings yet
- Kaoa Nov 2023Document10 pagesKaoa Nov 2023manan shroffNo ratings yet
- Arvin Noscal Pediatric FemurDocument84 pagesArvin Noscal Pediatric FemuranoscalNo ratings yet
- Lower Extremity Fracture CasesDocument82 pagesLower Extremity Fracture CasesradtechbeeNo ratings yet
- My Experience in Paediatric Orthopaedics at Sanchetti Institute For Orthopaedics and RehabilitationDocument48 pagesMy Experience in Paediatric Orthopaedics at Sanchetti Institute For Orthopaedics and RehabilitationMd Ahsanuzzaman PinkuNo ratings yet
- Discuss Tension Band Principles: by DR Kabiru SALISU 11 Aug. 2017Document40 pagesDiscuss Tension Band Principles: by DR Kabiru SALISU 11 Aug. 2017Azmi FarhadiNo ratings yet
- Developmental Orthopedic Disease - EQDocument33 pagesDevelopmental Orthopedic Disease - EQCaitlinNo ratings yet
- TKR Physical TherapyDocument29 pagesTKR Physical TherapyHUZAIFA YAMAANNo ratings yet
- Basic Periodontal Surgeries II Applications V2Document51 pagesBasic Periodontal Surgeries II Applications V2pvsmj5kdk4No ratings yet
- Lower Limb Trauma: Cast Application For Common FracturesDocument58 pagesLower Limb Trauma: Cast Application For Common FracturesdrusmanjamilhcmdNo ratings yet
- ProsthesisDocument42 pagesProsthesissmrutiptNo ratings yet
- Therapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.17Document45 pagesTherapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.17Mustafa ,GhulamNo ratings yet
- Total Knee Arthroplasty PrinciplesDocument40 pagesTotal Knee Arthroplasty PrinciplesMitri NassarNo ratings yet
- ClubfootDocument52 pagesClubfootArianto PrabowoNo ratings yet
- Clubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)Document87 pagesClubfoot - The Ponseti Method: Dale Elizabeth Jarka, MD, CM, FRCS (C)muthia saniNo ratings yet
- Workshop ACHILLES - Tendon Repair and DebridementDocument21 pagesWorkshop ACHILLES - Tendon Repair and Debridementfctn deltaNo ratings yet
- Presentation 1Document16 pagesPresentation 1Moiz AliNo ratings yet
- Management of Genital ProlapseDocument39 pagesManagement of Genital Prolapsecool_ice2t6No ratings yet
- Journal Reading: Nonunion of Fracture ClavicleDocument14 pagesJournal Reading: Nonunion of Fracture ClavicleKhafid Asy' AriNo ratings yet
- Review Journal: Ceramic-On-Ceramic Bearings Total Hip Arthroplasty in Young PatientsDocument11 pagesReview Journal: Ceramic-On-Ceramic Bearings Total Hip Arthroplasty in Young PatientsAficena HimdaniNo ratings yet
- FX of Distal HumerusDocument76 pagesFX of Distal HumerusGrace NazarenoNo ratings yet
- Developmental Dysplasia of HipDocument68 pagesDevelopmental Dysplasia of HipwildanmalikNo ratings yet
- Principles Casting Lower LimbDocument56 pagesPrinciples Casting Lower LimbDiana Veroshini GengatharanNo ratings yet
- Paper Presentation Supracutaneous Locking Compression PlateDocument21 pagesPaper Presentation Supracutaneous Locking Compression PlateSourabh AlawaNo ratings yet
- Implant OlogyDocument76 pagesImplant OlogyTaher RupawalaNo ratings yet
- Indian Dental Academy: Leader in Continuing Dental EducationDocument13 pagesIndian Dental Academy: Leader in Continuing Dental Educationindian dental academyNo ratings yet
- ACL InjuryDocument42 pagesACL InjuryRishabh VermaNo ratings yet
- Management of Fracture Acetabulum in Geriatric Age Group Saturday 12 15Document44 pagesManagement of Fracture Acetabulum in Geriatric Age Group Saturday 12 15tarikeopsNo ratings yet
- Femeroacetabular Impingement (FAI) A Precursor of Hip OsteoarthritisDocument69 pagesFemeroacetabular Impingement (FAI) A Precursor of Hip OsteoarthritistarikeopsNo ratings yet
- Ender Nailing in HumerusDocument56 pagesEnder Nailing in HumerusRakesh KumarNo ratings yet
- ZR Implnt Semi FinalDocument40 pagesZR Implnt Semi FinalVinceEjorangoCabigaoNo ratings yet
- Artificial Urinary Sphincter Case ReportDocument12 pagesArtificial Urinary Sphincter Case ReportAaron DesaiNo ratings yet
- Post-Op Shoulder 1Document49 pagesPost-Op Shoulder 1api-557944670No ratings yet
- Denture ConversionDocument11 pagesDenture Conversionaastha dogra100% (1)
- Ins and Outs of Total Hip ReplacementsDocument40 pagesIns and Outs of Total Hip ReplacementsAntonia ChenNo ratings yet
- Advanced Endoscopy Techniques: Jayant P.Talreja, M.D. Gastrointestinal Specialists, Inc. Bon Secours St. Mary's HospitalDocument25 pagesAdvanced Endoscopy Techniques: Jayant P.Talreja, M.D. Gastrointestinal Specialists, Inc. Bon Secours St. Mary's HospitaldrelvNo ratings yet
- Arthroscopic Bankart Repair: T. Andrew Israel, MDDocument32 pagesArthroscopic Bankart Repair: T. Andrew Israel, MDRamakrishna JakkulaNo ratings yet
- Post Op Ankle Arthroscopy Lateral Ligament Repair July 2020Document1 pagePost Op Ankle Arthroscopy Lateral Ligament Repair July 2020Tomas DominguezNo ratings yet
- Spineinstrumentation 220325073013Document98 pagesSpineinstrumentation 220325073013Anwer YahyaNo ratings yet
- Total Hip Arthroplasty 243Document40 pagesTotal Hip Arthroplasty 243jefferyNo ratings yet
- 1 Handout Fedorka Ostrander Ortho Trauma 5.11.18Document52 pages1 Handout Fedorka Ostrander Ortho Trauma 5.11.18Kris ChenNo ratings yet
- Principles of Orofacial ReconstructionDocument29 pagesPrinciples of Orofacial ReconstructionMohd ZahiNo ratings yet
- Closed Reduction, Traction, and Casting Techniques: David Hak, MDDocument57 pagesClosed Reduction, Traction, and Casting Techniques: David Hak, MDDeep Katyan DeepNo ratings yet
- High Tibial OsteotomiesDocument24 pagesHigh Tibial OsteotomiesMuhamad Izwan Bin HanafiNo ratings yet
- Elbow Fractures AND DislocationsDocument45 pagesElbow Fractures AND DislocationsErrory RamadiansyahNo ratings yet
- Neglected Femoral Neck Fractures in AdultsDocument21 pagesNeglected Femoral Neck Fractures in AdultsJauharil Wafi MuhammadNo ratings yet
- Pre-Operative Conference: Trauma 4 Service Jafer Terrence Lim, M.DDocument22 pagesPre-Operative Conference: Trauma 4 Service Jafer Terrence Lim, M.DjcreynesNo ratings yet
- LL AmputationDocument119 pagesLL AmputationMpt SportsNo ratings yet
- Ventral Hernia CaseDocument63 pagesVentral Hernia CaseROUNAK MEHROTRANo ratings yet
- Benign Positional Vertigo: Taleb Mohammed Mansoor Khaleil Ebrahem Al-MatroushiDocument27 pagesBenign Positional Vertigo: Taleb Mohammed Mansoor Khaleil Ebrahem Al-MatroushiSheila CantikNo ratings yet
- BPPVDocument27 pagesBPPVheavyrainNo ratings yet
- Biomechanical Comparison of Dynamic Hip Screw, ProximalDocument24 pagesBiomechanical Comparison of Dynamic Hip Screw, ProximalPriscilla PriscillaNo ratings yet
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenFrom EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenNo ratings yet
- CHP 11. Human Resource Information System-Ppt12Document44 pagesCHP 11. Human Resource Information System-Ppt12Dipen ShahNo ratings yet
- Prin. L.N.Welingkar Institute of Management Development & ResearchDocument15 pagesPrin. L.N.Welingkar Institute of Management Development & ResearchDipen ShahNo ratings yet
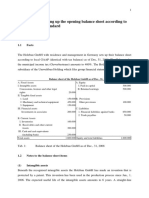
- Case Study 1: Setting Up The Opening Balance Sheet According To The IFRS-SME-StandardDocument4 pagesCase Study 1: Setting Up The Opening Balance Sheet According To The IFRS-SME-StandardDipen ShahNo ratings yet
- We Like Project: by Prakhar Jain HPGD/JL15/2321Document44 pagesWe Like Project: by Prakhar Jain HPGD/JL15/2321Dipen ShahNo ratings yet
- Circulatory System Answer SheetDocument4 pagesCirculatory System Answer SheetMarlie TobiseNo ratings yet
- Aorn Position Statement On Perioperative Care of Patients With Do-Not-Resucitate or Allow-natural-Death OrdersDocument5 pagesAorn Position Statement On Perioperative Care of Patients With Do-Not-Resucitate or Allow-natural-Death OrdersRudy DuterteNo ratings yet
- The Hybrid Ring Fixator: Surgical TechniqueDocument32 pagesThe Hybrid Ring Fixator: Surgical TechniqueMohamad RamadanNo ratings yet
- Coma and Brain DeathDocument24 pagesComa and Brain DeathDean AccountNo ratings yet
- Chapter 036Document9 pagesChapter 036Neverends201160% (5)
- PrefixDocument8 pagesPrefixleian28No ratings yet
- Chest: Perioperative Management of Antithrombotic TherapyDocument25 pagesChest: Perioperative Management of Antithrombotic TherapyMahtheerNo ratings yet
- Bariatric Surgery As An Efficient Treatment For Non-Alcoholic Fatty Liver Disease in A Prospective Study With 1-Year Follow-UpDocument9 pagesBariatric Surgery As An Efficient Treatment For Non-Alcoholic Fatty Liver Disease in A Prospective Study With 1-Year Follow-UpTony Miguel Saba SabaNo ratings yet
- Development of MandibleDocument14 pagesDevelopment of MandibleMahesh kumarNo ratings yet
- Medical ImagingDocument2 pagesMedical Imagingsiva kumaarNo ratings yet
- BVCCT-304 EchocardiographyDocument71 pagesBVCCT-304 EchocardiographyManisha khanNo ratings yet
- Gastric Cancer in The East and West What Should We LearnDocument1 pageGastric Cancer in The East and West What Should We LearnBrahim OuyabaNo ratings yet
- Emergency Obstetric Care in The Prevention of Maternal MortalityDocument9 pagesEmergency Obstetric Care in The Prevention of Maternal Mortalityapi-3705046No ratings yet
- DAFTAR PUSTAKA YuniiiDocument3 pagesDAFTAR PUSTAKA Yuniiiule kenziNo ratings yet
- Renal TraumaDocument30 pagesRenal TraumaBernardNo ratings yet
- AOMSI MC2022 ScheduleDocument10 pagesAOMSI MC2022 ScheduleDarain ShahidNo ratings yet
- New Microsoft Office PowerPoint PresentationDocument33 pagesNew Microsoft Office PowerPoint PresentationVasuda Devi MalepatiNo ratings yet
- Incise Drape CatalogueDocument10 pagesIncise Drape CatalogueShadreck MabvoroNo ratings yet
- CLP Surgical GuideDocument3 pagesCLP Surgical GuideAmit SadhwaniNo ratings yet
- Neuroanesthesia Updates 2020Document174 pagesNeuroanesthesia Updates 2020Rasika ChandrasekaraNo ratings yet
- Maxillofacial Reconstruction 2013Document237 pagesMaxillofacial Reconstruction 2013Mohammed Qasim Al-WataryNo ratings yet
- Se Soigner en France en BDDocument28 pagesSe Soigner en France en BDAnthony CôteNo ratings yet