You might also like
- Neil Strauss - The Annihilation Method - Style's Archives - Volume 1 - The Origin of Style - How To Transform From Chump To Champ in No TimeDocument132 pagesNeil Strauss - The Annihilation Method - Style's Archives - Volume 1 - The Origin of Style - How To Transform From Chump To Champ in No TimeDaniel Nii Armah Tetteh100% (2)
- Orthopedic Study GuideDocument17 pagesOrthopedic Study GuideD'Arby Janelle SmithNo ratings yet
- Understanding Income Statements EPS CalculationsDocument39 pagesUnderstanding Income Statements EPS CalculationsKeshav KaplushNo ratings yet
- C42135AA Beckman Coulter ClearLLab 10C Casebook PDFDocument586 pagesC42135AA Beckman Coulter ClearLLab 10C Casebook PDFHam Bone100% (1)
- Chapter-7-Orthopedic EmergenciesDocument24 pagesChapter-7-Orthopedic EmergenciesALAY DRUSSNo ratings yet
- Humeral Intracondylar Fissure PresentationDocument17 pagesHumeral Intracondylar Fissure PresentationNancy MorsiNo ratings yet
- Update A1 OsceDocument120 pagesUpdate A1 OsceIndra SetyaNo ratings yet
- Thesis On Inguinal HerniaDocument7 pagesThesis On Inguinal Herniaambermooreeverett100% (3)
- Femoral Neck FractureDocument28 pagesFemoral Neck FractureayuegpNo ratings yet
- Principles Fracture ManagementDocument88 pagesPrinciples Fracture ManagementYauffa Hanna Elt MisykahNo ratings yet
- New Introduction To Ortho 1 Jan 20016Document67 pagesNew Introduction To Ortho 1 Jan 20016BIOLOGY BY ISMAIL ANSARINo ratings yet
- Colles FractureDocument89 pagesColles Fracturenur syafiqah kamaruzaman100% (1)
- Trauma - Intertrochanteric Fracture - RustiniDocument7 pagesTrauma - Intertrochanteric Fracture - Rustinidedyalkarni08No ratings yet
- Slipped Capital Femoral Epiphysis: MSC Otho, MRCS Assistant Lecturer of Orthopaedic at Ain Shams UniversityDocument30 pagesSlipped Capital Femoral Epiphysis: MSC Otho, MRCS Assistant Lecturer of Orthopaedic at Ain Shams UniversityBell Swan100% (1)
- Spinal Injury Management GuideDocument60 pagesSpinal Injury Management GuideRheselle LacuataNo ratings yet
- Slipped Capital Femoral EpiphysisDocument40 pagesSlipped Capital Femoral EpiphysisDrAshesh Desai100% (2)
- Case Report (Ola)Document44 pagesCase Report (Ola)amel015No ratings yet
- Case Report Indri-Noha FIXDocument5 pagesCase Report Indri-Noha FIXIndri Pratiwi TobingNo ratings yet
- Tibial PlateauDocument43 pagesTibial Plateauamal.fathullahNo ratings yet
- STFM Trauma Curriculum Pelvic FractureDocument25 pagesSTFM Trauma Curriculum Pelvic FractureDanang Firman Last BreathNo ratings yet
- Femur Shaft FractureDocument33 pagesFemur Shaft FractureAkash KoulNo ratings yet
- Spinal Deformities NewDocument79 pagesSpinal Deformities Newapi-26159412100% (3)
- Closed reduction and internal fixation of humerus shaft fractures with Ender nailsDocument56 pagesClosed reduction and internal fixation of humerus shaft fractures with Ender nailsRakesh KumarNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- Amputation RehabilitationDocument59 pagesAmputation RehabilitationAnushree DatarNo ratings yet
- LL AmputationDocument119 pagesLL AmputationMpt SportsNo ratings yet
- SkeliosisDocument55 pagesSkeliosisevelynNo ratings yet
- Tuberculosis of SpineDocument19 pagesTuberculosis of SpinemelittaaNo ratings yet
- CBT Orthopaedics Fractures - TutorDocument30 pagesCBT Orthopaedics Fractures - Tutoramoody95No ratings yet
- Physiological Variables in Children-2nd JulyDocument57 pagesPhysiological Variables in Children-2nd JulyShobhit VermaNo ratings yet
- Pathological FractureDocument92 pagesPathological FractureSeptyAuliaNo ratings yet
- Coxa PlanaDocument9 pagesCoxa PlanaRegine BlanzaNo ratings yet
- Neglected Femoral Neck Fractures in AdultsDocument21 pagesNeglected Femoral Neck Fractures in AdultsJauharil Wafi MuhammadNo ratings yet
- Case Study - Intertrochanteric Hip FractureDocument13 pagesCase Study - Intertrochanteric Hip FractureLei Ortega100% (6)
- Tibial Plateau Fractures: Yasser AlwabliDocument35 pagesTibial Plateau Fractures: Yasser AlwabliPin Han NaNo ratings yet
- Developmental Dysplasia of Hip: Diagnosis and TreatmentDocument68 pagesDevelopmental Dysplasia of Hip: Diagnosis and TreatmentwildanmalikNo ratings yet
- Case Presentation: HistoryDocument45 pagesCase Presentation: HistorySaya MenangNo ratings yet
- Subspec EssentialsDocument343 pagesSubspec EssentialsLavern GwynetteNo ratings yet
- REVISION TKR DR Hamad DammamDocument108 pagesREVISION TKR DR Hamad DammamFahad MNo ratings yet
- Hip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDDocument97 pagesHip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDLassie LazyNo ratings yet
- Examination AAOS 2009 SpineDocument56 pagesExamination AAOS 2009 SpineJulieta PereyraNo ratings yet
- Department of Orthopaedics: Alluri Sitarama Raju Academy of Medical SciencesDocument18 pagesDepartment of Orthopaedics: Alluri Sitarama Raju Academy of Medical SciencesVivek ChNo ratings yet
- Amputation Rehabilitation in 40 CharactersDocument25 pagesAmputation Rehabilitation in 40 CharactersHillaryNo ratings yet
- Prolapse Lumbar DiscDocument40 pagesProlapse Lumbar DiscAlfred BantigueNo ratings yet
- Hip DislocDocument67 pagesHip DislocAli TawbeNo ratings yet
- My Experience in Paediatric Orthopaedics at Sanchetti Institute For Orthopaedics and RehabilitationDocument48 pagesMy Experience in Paediatric Orthopaedics at Sanchetti Institute For Orthopaedics and RehabilitationMd Ahsanuzzaman PinkuNo ratings yet
- Journal Reading: Nonunion of Fracture ClavicleDocument14 pagesJournal Reading: Nonunion of Fracture ClavicleKhafid Asy' AriNo ratings yet
- 13 - Musculoskeletal System AssessmentDocument53 pages13 - Musculoskeletal System Assessmente.mb275No ratings yet
- HerniaSurge Guidelines 2Document28 pagesHerniaSurge Guidelines 2ROUNAK MEHROTRANo ratings yet
- OU Shoulder Elbow Review: Nonsurgical Greater Tuberosity Fracture TreatmentDocument159 pagesOU Shoulder Elbow Review: Nonsurgical Greater Tuberosity Fracture TreatmentJayNo ratings yet
- Foot and Ankle Injuries Kylee Phillips - 0Document74 pagesFoot and Ankle Injuries Kylee Phillips - 0rizwan.mughal1997No ratings yet
- Amputee RehabDocument89 pagesAmputee RehabAli FahesNo ratings yet
- Adult-Acquired Flatfoot DeformityDocument27 pagesAdult-Acquired Flatfoot DeformityNajeeb BsoulNo ratings yet
- Therapeutic Management of Distal Radius Fractures Slide ShowDocument38 pagesTherapeutic Management of Distal Radius Fractures Slide ShowMochammad Syarief HidayatNo ratings yet
- Abdominal injury management guideDocument113 pagesAbdominal injury management guideDrArnab MohantyNo ratings yet
- Oite 2006Document823 pagesOite 2006dastroh100% (1)
- Gait Abnormalities Following Slipped CapitalDocument8 pagesGait Abnormalities Following Slipped Capitalyarimar hoyosNo ratings yet
- Amputee RehabDocument153 pagesAmputee RehabNancy GuptaNo ratings yet
- C2 Chordoma A Case Report: Dr. M. Ashok Kumar Consultant Spine Surgeon, SNHRC, VelloreDocument38 pagesC2 Chordoma A Case Report: Dr. M. Ashok Kumar Consultant Spine Surgeon, SNHRC, VellorevarshneyNo ratings yet
- Handbook of Lower Extremity Reconstruction: Clinical Case-Based Review and Flap AtlasFrom EverandHandbook of Lower Extremity Reconstruction: Clinical Case-Based Review and Flap AtlasScott T. HollenbeckNo ratings yet
- Tips and Tricks for Problem Fractures, Volume I: The Upper ExtremityFrom EverandTips and Tricks for Problem Fractures, Volume I: The Upper ExtremityDaniel S. HorwitzNo ratings yet
- Surgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesFrom EverandSurgical Principles in Inguinal Hernia Repair: A Comprehensive Guide to Anatomy and Operative TechniquesMelissa Phillips LaPinskaNo ratings yet
- The Inverted Orthotic Technique: A Process of Foot Stabilization for Pronated FeetFrom EverandThe Inverted Orthotic Technique: A Process of Foot Stabilization for Pronated FeetNo ratings yet
- Aling Presing ChichacornDocument2 pagesAling Presing ChichacornMhel Joshua Bautista HermitanioNo ratings yet
- INTELLISPEC SERIE V-Páginas-31-46Document16 pagesINTELLISPEC SERIE V-Páginas-31-46Antonio Valencia VillejoNo ratings yet
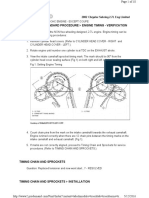
- 02+sebring+2.7+timing+chainDocument10 pages02+sebring+2.7+timing+chainMaushil Salman MarkNo ratings yet
- Bartending and Catering: Agenda: Basics of Bartending Bar Tools and EquipmentDocument146 pagesBartending and Catering: Agenda: Basics of Bartending Bar Tools and EquipmentMars Mar100% (1)
- Belotero Intense LidocaineDocument7 pagesBelotero Intense LidocaineAnnaNo ratings yet
- Analisis Hasil Led Pada Jam Pertama Dan Jam KeduaDocument11 pagesAnalisis Hasil Led Pada Jam Pertama Dan Jam KeduavirafutmainnarNo ratings yet
- List of Blade MaterialsDocument19 pagesList of Blade MaterialsAnie Ummu Alif & SyifaNo ratings yet
- 337 686 1 SMDocument8 pages337 686 1 SMK61 ĐOÀN HỒ GIA HUYNo ratings yet
- 01 - Narmada M PhilDocument200 pages01 - Narmada M PhilafaceanNo ratings yet
- Proposal On Online Examination For BE EntranceDocument21 pagesProposal On Online Examination For BE Entrancesubhash22110360% (5)
- Remove Fuel Sub TankDocument9 pagesRemove Fuel Sub Tankthierry.fifieldoutlook.comNo ratings yet
- WholeDocument397 pagesWholedelbot01No ratings yet
- Roof Beam Layout - r1Document1 pageRoof Beam Layout - r1Niraj ShindeNo ratings yet
- Sample Resume For HRDocument2 pagesSample Resume For HRnapinnvoNo ratings yet
- Orphanage Cum Old Age Home: Amruta Prakash BedmuthaDocument2 pagesOrphanage Cum Old Age Home: Amruta Prakash BedmuthaNamrata Bhandari100% (1)
- CEO Corner New Products Powerful Pocket SimulatorDocument23 pagesCEO Corner New Products Powerful Pocket SimulatorMOHAMMA MUSANo ratings yet
- Pavements ConstructedDocument16 pagesPavements ConstructedjoryNo ratings yet
- Solution SellingDocument18 pagesSolution Sellingvikramgulati13090% (1)
- Gauss Jordan MethodDocument6 pagesGauss Jordan MethodnNo ratings yet
- Australian Institute For Teaching and School Leadership - AITSLDocument5 pagesAustralian Institute For Teaching and School Leadership - AITSLYu LiNo ratings yet
- SAP ABAP Interview Questions and AnswersDocument8 pagesSAP ABAP Interview Questions and AnswersKarthi ThirumalaisamyNo ratings yet
- F5 GTM Concepts Guide v11Document209 pagesF5 GTM Concepts Guide v11Majnu SmNo ratings yet
- Pradeep Kumaresan Resume - Software Testing ExperienceDocument3 pagesPradeep Kumaresan Resume - Software Testing ExperienceSANTANo ratings yet
- Collective BargainingDocument18 pagesCollective Bargainingchandni kundel100% (3)
- PIRA - 2022 - ESTIMATED FMV As of October 2022Document48 pagesPIRA - 2022 - ESTIMATED FMV As of October 2022Aggy ReynadoNo ratings yet
- Studentwise Final Placement DetailsLast 3 YearsDocument18 pagesStudentwise Final Placement DetailsLast 3 YearsAmitNo ratings yet
- Clinical Presentation of Ectopic Pregnancy Turned Out to Be Ectopic PregnancyDocument33 pagesClinical Presentation of Ectopic Pregnancy Turned Out to Be Ectopic PregnancyRosiNo ratings yet