You might also like
- Arches of FootDocument75 pagesArches of Footvaibhav gowdaNo ratings yet
- Anterior Knee Pain Syndrome ReferatDocument28 pagesAnterior Knee Pain Syndrome ReferatnurulNo ratings yet
- Lecture 13 Bone, Joint, Tendon, and Soft Tissue Injury in Lower Limb (Knee)Document143 pagesLecture 13 Bone, Joint, Tendon, and Soft Tissue Injury in Lower Limb (Knee)Wilson HalimNo ratings yet
- Running Injury: Hui-Ting Lin, PT, PHDDocument36 pagesRunning Injury: Hui-Ting Lin, PT, PHDMandy NgNo ratings yet
- Femur Shaft FractureDocument33 pagesFemur Shaft FractureAkash KoulNo ratings yet
- Pediatric Orthopaedics: Dr. Andreas Siagian SpotDocument66 pagesPediatric Orthopaedics: Dr. Andreas Siagian SpotFirdausi RiskiviawinandaNo ratings yet
- Group 7 LMRDocument32 pagesGroup 7 LMRQamar AhmedNo ratings yet
- Footdropkevinja 141118013605 Conversion Gate01 2Document26 pagesFootdropkevinja 141118013605 Conversion Gate01 2Musa LandeNo ratings yet
- Ankle Foot Final EBRDocument7 pagesAnkle Foot Final EBRdrurfiNo ratings yet
- lecture_2_Unit_VIDocument53 pageslecture_2_Unit_VIRiya AdhangleNo ratings yet
- Pes Planus and Pes Valgus DR BijayDocument60 pagesPes Planus and Pes Valgus DR BijayBijay MehtaNo ratings yet
- Foot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDDocument55 pagesFoot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDrizwan.mughal1997No ratings yet
- FracturePPT UpdatedDocument108 pagesFracturePPT Updatedgaile pattugalanNo ratings yet
- Approach To Pes CavusDocument52 pagesApproach To Pes CavusSubarna PaudelNo ratings yet
- Sport Traumatology-III Foot and Ankle Joint-15Document47 pagesSport Traumatology-III Foot and Ankle Joint-15kamran aliNo ratings yet
- LL AmputationDocument119 pagesLL AmputationMpt SportsNo ratings yet
- Foot and Ankle BiomechanicsDocument25 pagesFoot and Ankle BiomechanicsSanh NguyễnNo ratings yet
- Pediatric OrthopaedicDocument66 pagesPediatric OrthopaedicDhito RodriguezNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- ClubfootDocument5 pagesClubfootcreyannc0% (1)
- Anatomy Biomechanics of AnkleDocument82 pagesAnatomy Biomechanics of AnklelypiheNo ratings yet
- Cavus Foot Deformity Evaluation and Surgical TechniquesDocument13 pagesCavus Foot Deformity Evaluation and Surgical TechniquesRadu StoenescuNo ratings yet
- Chapter 5 Pediatric PodiatryDocument88 pagesChapter 5 Pediatric Podiatrypodmmgf100% (1)
- Cad wk9-10 QsDocument10 pagesCad wk9-10 Qsapi-468597987No ratings yet
- Recurrent Patella DislocationDocument10 pagesRecurrent Patella DislocationArko duttaNo ratings yet
- MCHT Leading and Managing Your Organisation Musculoskeletal Education IC3Document49 pagesMCHT Leading and Managing Your Organisation Musculoskeletal Education IC3nickmirad2No ratings yet
- Physiological Variables in Children-2nd JulyDocument57 pagesPhysiological Variables in Children-2nd JulyShobhit VermaNo ratings yet
- Prosthetic Management of Lower Limb Amputations' NotesDocument5 pagesProsthetic Management of Lower Limb Amputations' NotesAnu YadavNo ratings yet
- Dr. Muh. Sakti SpotDocument25 pagesDr. Muh. Sakti SpotTiti Afrida SariNo ratings yet
- Bow Legs, Knock Knees and Other Normal Variants: DR David Bade Director of Orthopaedics Lady Cilento Children's HospitalDocument56 pagesBow Legs, Knock Knees and Other Normal Variants: DR David Bade Director of Orthopaedics Lady Cilento Children's HospitalvameldaNo ratings yet
- Osteoarthritis: Dr. C. C. VisserDocument85 pagesOsteoarthritis: Dr. C. C. VisserAhmad Fathira FitraNo ratings yet
- 30.ankle & Foot DiseasesDocument46 pages30.ankle & Foot DiseasesDuha HamidNo ratings yet
- Genu Valgus Genu VarusDocument35 pagesGenu Valgus Genu VarusRatu FaniaNo ratings yet
- Congenitalpseudoarthrosistibianew 140111101614 PhpappDocument66 pagesCongenitalpseudoarthrosistibianew 140111101614 PhpappKrunal PatelNo ratings yet
- Ankle FracturesDocument41 pagesAnkle Fracturesshammasbm100% (12)
- Hip Joint DislocationDocument59 pagesHip Joint DislocationAnonymous P5FDn81yNo ratings yet
- The Hip: Therapeutic Exercise 2 Lino Linford BangayanDocument91 pagesThe Hip: Therapeutic Exercise 2 Lino Linford BangayanLino Linford Yu Bangayan100% (1)
- New Introduction To Ortho 1 Jan 20016Document67 pagesNew Introduction To Ortho 1 Jan 20016BIOLOGY BY ISMAIL ANSARINo ratings yet
- Foot and Ankle Injuries Kylee Phillips - 0Document74 pagesFoot and Ankle Injuries Kylee Phillips - 0Charlez OhanuNo ratings yet
- Orthopedic RSUD Panembahan Senopati BantulDocument28 pagesOrthopedic RSUD Panembahan Senopati Bantulwinda alviraNo ratings yet
- SPONDYLOLISTHESISDocument27 pagesSPONDYLOLISTHESISJulioYoko100% (1)
- CTEVDocument46 pagesCTEVjhogie afitnandriNo ratings yet
- Knee&Foot Part2Document26 pagesKnee&Foot Part2SarkawtNo ratings yet
- Introduction of MSK ImagingDocument63 pagesIntroduction of MSK ImagingyeabsraNo ratings yet
- Differential DiagnosisDocument14 pagesDifferential DiagnosisnurulNo ratings yet
- Hip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDDocument97 pagesHip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDLassie LazyNo ratings yet
- Patella Fracture: Mahmoud Ashour Orthopedic ResidentDocument23 pagesPatella Fracture: Mahmoud Ashour Orthopedic ResidentMohammed ahmedNo ratings yet
- Group 7th SURGERY Finl-1Document17 pagesGroup 7th SURGERY Finl-1Ayesha ShafiqNo ratings yet
- Tuberculosis of Knee: Presented By: DR Dipendra Maharjan 2 Yr Resident, MS Orthopaedics NAMS, Bir HospitalDocument25 pagesTuberculosis of Knee: Presented By: DR Dipendra Maharjan 2 Yr Resident, MS Orthopaedics NAMS, Bir HospitalshravaniNo ratings yet
- Common Pediatric FracturesDocument42 pagesCommon Pediatric FracturesyanNo ratings yet
- Ankle D.DDocument16 pagesAnkle D.Dمحمد عقلNo ratings yet
- Clubfoot Guide: Causes, Symptoms & TreatmentDocument17 pagesClubfoot Guide: Causes, Symptoms & TreatmentMulya ImansyahNo ratings yet
- Amputation Rehabilitation in 40 CharactersDocument25 pagesAmputation Rehabilitation in 40 CharactersHillaryNo ratings yet
- Hip DislocDocument67 pagesHip DislocAli TawbeNo ratings yet
- Footdrop 160909012734Document62 pagesFootdrop 160909012734Jesmick GarryNo ratings yet
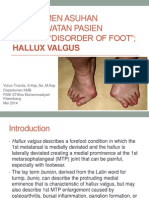
- Manajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREEDocument29 pagesManajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREENovita DamaiyantiNo ratings yet
- Posterior Tibial Tendon Dysfunction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPosterior Tibial Tendon Dysfunction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Plantar Heel Pain, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPlantar Heel Pain, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Improving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsFrom EverandImproving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsNo ratings yet
- Flat Foot (Pes Planus), A Simple Guide to The Condition, Treatment And Related ConditionsFrom EverandFlat Foot (Pes Planus), A Simple Guide to The Condition, Treatment And Related ConditionsRating: 1 out of 5 stars1/5 (1)
- Ankle Arthodesis: DR - Mohammed Alotaibi Tutor: DR - Nader AlkenaniDocument44 pagesAnkle Arthodesis: DR - Mohammed Alotaibi Tutor: DR - Nader AlkenaniNajeeb BsoulNo ratings yet
- Adult-Acquired Flatfoot DeformityDocument27 pagesAdult-Acquired Flatfoot DeformityNajeeb BsoulNo ratings yet
- Vitamine C, Foot & AnkleDocument13 pagesVitamine C, Foot & AnkleNajeeb BsoulNo ratings yet
- Minimally Invasive Surgical Management of Diabetic FootDocument31 pagesMinimally Invasive Surgical Management of Diabetic FootNajeeb BsoulNo ratings yet
- Charcot Joint & Methods of ArthrodesisDocument59 pagesCharcot Joint & Methods of ArthrodesisNajeeb BsoulNo ratings yet
- Ankle Arthodesis: DR - Mohammed Alotaibi Tutor: DR - Nader AlkenaniDocument44 pagesAnkle Arthodesis: DR - Mohammed Alotaibi Tutor: DR - Nader AlkenaniNajeeb BsoulNo ratings yet
- Final 718Document9 pagesFinal 718Hardik KhariwalNo ratings yet
- Richard Harris CVDocument2 pagesRichard Harris CVbombz4No ratings yet
- Chapter 13 Designing and Delivering Business Presentations 1Document39 pagesChapter 13 Designing and Delivering Business Presentations 1Kathryn Krystal R LanuzaNo ratings yet
- Bais-Ia 101Document2 pagesBais-Ia 101Emir NatividadNo ratings yet
- Dylan Regan ResumeDocument1 pageDylan Regan Resumeapi-380370571No ratings yet
- The power of a teacher's personal qualitiesDocument3 pagesThe power of a teacher's personal qualitiesPrincess LopezNo ratings yet
- University of North Texas 2Document4 pagesUniversity of North Texas 2SEED ProjectNo ratings yet
- INT2-004 - Comparative MGT - Admin.Document7 pagesINT2-004 - Comparative MGT - Admin.Tega NesirosanNo ratings yet
- Oral-Comm Q2W1Document6 pagesOral-Comm Q2W1Elmerito MelindoNo ratings yet
- Ignatavicius: Medical-Surgical Nursing, 6th Edition Chapter 5 Test BankDocument19 pagesIgnatavicius: Medical-Surgical Nursing, 6th Edition Chapter 5 Test BankTracy Bartell80% (10)
- Lack of Learning MaterialDocument2 pagesLack of Learning MaterialJenifer Languido CalautitNo ratings yet
- Languages of SingaporeDocument20 pagesLanguages of SingaporeLemuel SoNo ratings yet
- Woman Centred Care: A Concept AnalysisDocument37 pagesWoman Centred Care: A Concept AnalysisArdin MunrekNo ratings yet
- What Are Learning DisabilitiesDocument4 pagesWhat Are Learning DisabilitiesSiyad SiddiqueNo ratings yet
- Drout Way With WordsDocument82 pagesDrout Way With Wordssamanera2100% (3)
- Text 1 - ElementaryDocument4 pagesText 1 - ElementaryCátia Almeida100% (5)
- Mathematics 8 Lesson Plan On Finding The Equation of A Line: Republika NG PilipinasDocument2 pagesMathematics 8 Lesson Plan On Finding The Equation of A Line: Republika NG PilipinasCaren Pogoy ManiquezNo ratings yet
- BBC Earth Magazine January 2017 Adventure HackersDocument4 pagesBBC Earth Magazine January 2017 Adventure HackersThames Discovery ProgrammeNo ratings yet
- Regional Schedule of School-Based Management Online VALIDATION of Level 3 Schools in SDODocument50 pagesRegional Schedule of School-Based Management Online VALIDATION of Level 3 Schools in SDOhogmc mediaNo ratings yet
- Bhagwati Products Apprenticeship Notification 2021Document3 pagesBhagwati Products Apprenticeship Notification 202118 - 442 RajuNo ratings yet
- Iitjammu Comp PDFDocument2 pagesIitjammu Comp PDFRahul VermaNo ratings yet
- Diagnostic Test Oral CommDocument3 pagesDiagnostic Test Oral CommGeneve GarzonNo ratings yet
- RW Reviewer UPDATEDDocument4 pagesRW Reviewer UPDATEDShane CanoNo ratings yet
- Five Models of Curriculum PlanningDocument12 pagesFive Models of Curriculum PlanningSol100% (1)
- Apply Quality StandardsDocument87 pagesApply Quality StandardsMat Domdom V. SansanoNo ratings yet
- Educational Technology 1 Course OutlineDocument4 pagesEducational Technology 1 Course Outlinecha ricohNo ratings yet
- Mark Sta Maria RESUME3Document3 pagesMark Sta Maria RESUME3mak_stamaiaNo ratings yet
- Module 1 - Special Education in The PhilippinesDocument9 pagesModule 1 - Special Education in The PhilippinesAj Comon Tabamo100% (2)
- Redcliffe Primary School Maths MEMODocument2 pagesRedcliffe Primary School Maths MEMOThula NkosiNo ratings yet
- DeathDocument31 pagesDeathsara marie bariaNo ratings yet