You might also like
- Badovinac 2013Document8 pagesBadovinac 2013Naji Z. ArandiNo ratings yet
- 1694 4169 1 PBDocument7 pages1694 4169 1 PBNaji Z. ArandiNo ratings yet
- MTA and BiodentineDocument12 pagesMTA and BiodentineNaji Z. ArandiNo ratings yet
- YemenDocument9 pagesYemenNaji Z. ArandiNo ratings yet
- Hybridization Quality and Bond Strength of Adhesive Systems According To Interaction With DentinDocument12 pagesHybridization Quality and Bond Strength of Adhesive Systems According To Interaction With DentinNaji Z. ArandiNo ratings yet
- Research Article: Marginal Sealing Durability of Two Contemporary Self-Etch AdhesivesDocument9 pagesResearch Article: Marginal Sealing Durability of Two Contemporary Self-Etch AdhesivesNaji Z. ArandiNo ratings yet
- Important Compositional Characteristics in The Clinical Use of Adhesive SystemsDocument9 pagesImportant Compositional Characteristics in The Clinical Use of Adhesive SystemsNaji Z. ArandiNo ratings yet
- Dentists' treatment preferences for deep caries lesionsDocument6 pagesDentists' treatment preferences for deep caries lesionsNaji Z. ArandiNo ratings yet
- Ce (Ek) F (Ak) PF1 (Ekak) Pfa (Ak) PF2 (Pag)Document6 pagesCe (Ek) F (Ak) PF1 (Ekak) Pfa (Ak) PF2 (Pag)Naji Z. ArandiNo ratings yet
- 8662755-Article Text-102421-1-10-20210611Document11 pages8662755-Article Text-102421-1-10-20210611Naji Z. ArandiNo ratings yet
- Diagnosis and Treatment of Anterior Cracked Tooth: A Case ReportDocument10 pagesDiagnosis and Treatment of Anterior Cracked Tooth: A Case ReportNaji Z. ArandiNo ratings yet
- Hyperdontia Review: Exploring Supernumerary Teeth DevelopmentDocument6 pagesHyperdontia Review: Exploring Supernumerary Teeth DevelopmentNaji Z. ArandiNo ratings yet
- Ejd - Ejd 397 17Document5 pagesEjd - Ejd 397 17Naji Z. ArandiNo ratings yet
- Attitudes and Behaviour Regarding Deep Dentin Caries Removal: A Survey Among German DentistsDocument9 pagesAttitudes and Behaviour Regarding Deep Dentin Caries Removal: A Survey Among German DentistsNaji Z. ArandiNo ratings yet
- Applicability of Autotransplantation in Cases of Missing UpperDocument12 pagesApplicability of Autotransplantation in Cases of Missing UpperNaji Z. ArandiNo ratings yet
- Direct Composite Resin Restorations in Posterior TeethDocument10 pagesDirect Composite Resin Restorations in Posterior TeethNaji Z. ArandiNo ratings yet
- Three - Drug Combination ofDocument5 pagesThree - Drug Combination ofNaji Z. ArandiNo ratings yet
- Mossaz 2014Document11 pagesMossaz 2014Naji Z. ArandiNo ratings yet
- Supernumerary Teeth: A Review On A Critical Endodontic ChallengeDocument6 pagesSupernumerary Teeth: A Review On A Critical Endodontic ChallengeNaji Z. ArandiNo ratings yet
- CCIDEN 42044 Posterior Composite Restoration Update Focus On Factors Inf - 051413Document10 pagesCCIDEN 42044 Posterior Composite Restoration Update Focus On Factors Inf - 051413Naji Z. ArandiNo ratings yet
- Jced 6 E116Document5 pagesJced 6 E116Naji Z. ArandiNo ratings yet
- DEVELOPMENTAL ANOMALIESDocument6 pagesDEVELOPMENTAL ANOMALIESNaji Z. ArandiNo ratings yet
- A Case With Bilateral Paired Maxillary Supernumerary IncisorDocument4 pagesA Case With Bilateral Paired Maxillary Supernumerary IncisorNaji Z. ArandiNo ratings yet
- Auto Transplant Replacement A Geminated Incisor A Supplemental IncisorDocument4 pagesAuto Transplant Replacement A Geminated Incisor A Supplemental IncisorNaji Z. ArandiNo ratings yet
- Prevalence and Distribution of Anomalies of Permanent Dentition in 9584 Japanese High School StudentsDocument10 pagesPrevalence and Distribution of Anomalies of Permanent Dentition in 9584 Japanese High School StudentsNaji Z. ArandiNo ratings yet
- Oral Health Attitudes, Knowledge, and Behavior Among School Children in North JordanDocument9 pagesOral Health Attitudes, Knowledge, and Behavior Among School Children in North JordanNaji Z. ArandiNo ratings yet
- IndianJDentSci93141-465093 125509Document7 pagesIndianJDentSci93141-465093 125509Naji Z. ArandiNo ratings yet
- Review Article: A Review of Supernumerary Teeth in The Premolar RegionDocument7 pagesReview Article: A Review of Supernumerary Teeth in The Premolar RegionNaji Z. ArandiNo ratings yet
- Managing cracked teeth with conservative treatmentDocument10 pagesManaging cracked teeth with conservative treatmentNaji Z. ArandiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cse Reviewer - MathDocument58 pagesCse Reviewer - MathLyne LerinNo ratings yet
- Pantheon-Katalog Eng WebDocument16 pagesPantheon-Katalog Eng WebJoe DoeNo ratings yet
- B Ed 3 Sem Physics Teaching Group C Science 1 Paper 1 Summer 2018Document3 pagesB Ed 3 Sem Physics Teaching Group C Science 1 Paper 1 Summer 2018Rrr KkkNo ratings yet
- Recycle ProgramDocument2 pagesRecycle ProgramKaps BlazeNo ratings yet
- CaseStudy AmtrakDocument14 pagesCaseStudy Amtraksnob_kNo ratings yet
- Life Time Prediction of GRP Piping SystemsDocument15 pagesLife Time Prediction of GRP Piping SystemsRamon FrenchNo ratings yet
- Image Forgery DetectionDocument17 pagesImage Forgery DetectionanlemacoNo ratings yet
- Topic 7.1 - Discrete Energy and Radioactivity Formative Assessment NAMEDocument2 pagesTopic 7.1 - Discrete Energy and Radioactivity Formative Assessment NAMEGajendraNo ratings yet
- MD R2 Nastran Release GuideDocument276 pagesMD R2 Nastran Release GuideMSC Nastran BeginnerNo ratings yet
- Philips HF C-Arm BrochureDocument2 pagesPhilips HF C-Arm Brochuregarysov50% (2)
- S2 Papers FinalizedDocument149 pagesS2 Papers FinalizedRaffles HolmesNo ratings yet
- Sampling and Field Testing at Wastewater Treatment FacilitiesDocument11 pagesSampling and Field Testing at Wastewater Treatment FacilitiesSundarapandiyan SundaramoorthyNo ratings yet
- A Review: HPLC Method Development and Validation: November 2015Document7 pagesA Review: HPLC Method Development and Validation: November 2015R Abdillah AkbarNo ratings yet
- 4jj1tybw01 Spec Sheet PDFDocument10 pages4jj1tybw01 Spec Sheet PDFcpaolinodNo ratings yet
- Computations on a waiters bill pad and conversations in the mistDocument3 pagesComputations on a waiters bill pad and conversations in the mistRavishu NagarwalNo ratings yet
- Top 21 Largest EMS Companies in WorldDocument22 pagesTop 21 Largest EMS Companies in WorldjackNo ratings yet
- Fit For WashingDocument85 pagesFit For WashingIyaka YoeNo ratings yet
- Collaboration Processes: Looking Inside the Black BoxDocument13 pagesCollaboration Processes: Looking Inside the Black Boxเข้าใจว่า น่าจะชื่อตุ้นNo ratings yet
- Astm A 182-2021Document17 pagesAstm A 182-2021Mohammed AliNo ratings yet
- Basics of Scientific Writing, Scientific Research, and Elementary Data AnalysisDocument12 pagesBasics of Scientific Writing, Scientific Research, and Elementary Data Analysisburhan sabirNo ratings yet
- Seminar Application of Nitrous Oxide in AutomobilesDocument20 pagesSeminar Application of Nitrous Oxide in AutomobilesSaikat BadyakarNo ratings yet
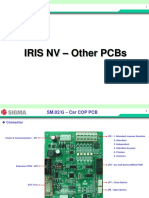
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet
- Saej401v002 PDFDocument6 pagesSaej401v002 PDFLuis LujanoNo ratings yet
- Computer Engineering SyllabusDocument47 pagesComputer Engineering SyllabusLily ChanNo ratings yet
- FT Aeroterme GEADocument15 pagesFT Aeroterme GEACrisTimNo ratings yet
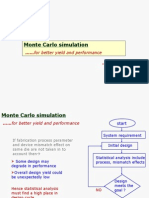
- Cadence Monte Carlo Simulation TutorialDocument51 pagesCadence Monte Carlo Simulation Tutorialkuomatt100% (1)
- Circuits Review P2Document44 pagesCircuits Review P2José CastilloNo ratings yet
- SFM Issue Repor 15-4-2023Document3 pagesSFM Issue Repor 15-4-2023Esdras Fransua CisnerosNo ratings yet
- Detecting Oil Spills from Remote SensorsDocument7 pagesDetecting Oil Spills from Remote SensorsFikri Adji Wiranto100% (1)
- Lista de Precios Tones y Staleks 01.04Document3 pagesLista de Precios Tones y Staleks 01.04Maria T. OliverosNo ratings yet