You might also like
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Accounting I ModuleDocument92 pagesAccounting I ModuleJay Githuku100% (1)
- DPP 1-7 Gravitation JA Nurture LiveDocument44 pagesDPP 1-7 Gravitation JA Nurture LiveTejaswi JhaNo ratings yet
- Epidemiology in A Nutshell NCI BenchmarksDocument8 pagesEpidemiology in A Nutshell NCI BenchmarksThe Nutrition CoalitionNo ratings yet
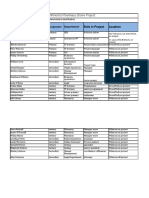
- Project Stakeholder register-DroneTechDocument4 pagesProject Stakeholder register-DroneTechfrank100% (2)
- Health Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central JavaDocument11 pagesHealth Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central Javaadilla kusumaNo ratings yet
- Day 33 Practice TestsDocument16 pagesDay 33 Practice TestsTUYẾN KIMTUYẾN0% (6)
- Syphilis in Pregnancy: Clinical Expert SeriesDocument15 pagesSyphilis in Pregnancy: Clinical Expert SeriesWindy MuldianiNo ratings yet
- Syphilis in PregnancyDocument17 pagesSyphilis in PregnancyKevin Stanley HalimNo ratings yet
- Assessment of Risk Factors in Antenatal Women at Ishaka Adventist Hospital, UgandaDocument9 pagesAssessment of Risk Factors in Antenatal Women at Ishaka Adventist Hospital, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- SphilisDocument17 pagesSphilisKharisma AstiNo ratings yet
- BMC Pregnancy Childbirth 2019Document8 pagesBMC Pregnancy Childbirth 2019cdsaludNo ratings yet
- Cervical Cancer - An Overview of Pathophysiology and ManagementDocument9 pagesCervical Cancer - An Overview of Pathophysiology and ManagementIndah 15No ratings yet
- Prevalence and Determinants of Anemia in Pregnancy, Sana'a, YemenDocument8 pagesPrevalence and Determinants of Anemia in Pregnancy, Sana'a, YemenIJPHSNo ratings yet
- 17 Listeriosis in PregnancyA ReviewDocument7 pages17 Listeriosis in PregnancyA ReviewRaul A UrbinaNo ratings yet
- Abel Man 2020Document6 pagesAbel Man 2020Redouane idrissiNo ratings yet
- Ped Infect Disease Jr. 2023Document4 pagesPed Infect Disease Jr. 2023cdsaludNo ratings yet
- Hiv Sul InglesDocument7 pagesHiv Sul Inglesandrea azevedoNo ratings yet
- Seminars in Oncology NursingDocument9 pagesSeminars in Oncology NursingangelitostorresitosNo ratings yet
- Costa de Macedo, 2017 - Risk Factors For Syphilis in WomenDocument12 pagesCosta de Macedo, 2017 - Risk Factors For Syphilis in WomenRima Carolina Bahsas ZakyNo ratings yet
- Syphilis During Pregnancy A Preventable Threat To Maternal-Fetal Health.Document12 pagesSyphilis During Pregnancy A Preventable Threat To Maternal-Fetal Health.Andrés Felipe Jaramillo TorresNo ratings yet
- Rethinking Mandatory HIV Testing During Pregnancy in Areas With High HIV Prevalence Rates: Ethical and Policy IssuesDocument5 pagesRethinking Mandatory HIV Testing During Pregnancy in Areas With High HIV Prevalence Rates: Ethical and Policy IssuesChristie ChungNo ratings yet
- E20201433 FullDocument15 pagesE20201433 FullcdsaludNo ratings yet
- Eff Ectiveness of Interventions To Improve Screening For Syphilis in Pregnancy: A Systematic Review and Meta-AnalysisDocument8 pagesEff Ectiveness of Interventions To Improve Screening For Syphilis in Pregnancy: A Systematic Review and Meta-AnalysisRocky.84No ratings yet
- Fonc 14 1386167Document6 pagesFonc 14 1386167epidemiojsmhNo ratings yet
- Original Article Vaginal Discharge: Perceptions and Health Seeking Behavior Among Nepalese WomenDocument5 pagesOriginal Article Vaginal Discharge: Perceptions and Health Seeking Behavior Among Nepalese WomennovywardanaNo ratings yet
- Predicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelDocument10 pagesPredicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelRiska Resty WasitaNo ratings yet
- Management of Newly Diagnosed HIV InfectionDocument16 pagesManagement of Newly Diagnosed HIV InfectionRoberto López MataNo ratings yet
- Contraception Counseling and Use Among AdolescentDocument6 pagesContraception Counseling and Use Among AdolescentAbdulrahman Al-otaibiNo ratings yet
- HIV and Pregnancy: How To Manage Conflicting Recommendations From Evidence-Based GuidelinesDocument6 pagesHIV and Pregnancy: How To Manage Conflicting Recommendations From Evidence-Based GuidelinesIsmaelJoséGonzálezGuzmánNo ratings yet
- Inborn Errors of Metabolism - Feb2011Document54 pagesInborn Errors of Metabolism - Feb2011Manuel Alvarado100% (1)
- Journal Pone 0253373Document17 pagesJournal Pone 0253373ElormNo ratings yet
- Cervical Cancer Research 1Document9 pagesCervical Cancer Research 1tivaNo ratings yet
- Recommendations For Human Immunodeficiency Virus Screening, Prophylaxis, and Treatment For Pregnant Women in The United StatesDocument14 pagesRecommendations For Human Immunodeficiency Virus Screening, Prophylaxis, and Treatment For Pregnant Women in The United StateselaNo ratings yet
- SOFA ObstetricoDocument14 pagesSOFA ObstetricoKarla DominguezNo ratings yet
- Maternal & Perinatal Outcome of Fever in Pregnancy in The Context of DengueDocument5 pagesMaternal & Perinatal Outcome of Fever in Pregnancy in The Context of DengueLola del carmen RojasNo ratings yet
- 43 FullDocument9 pages43 Fullnayeta levi syahdanaNo ratings yet
- HPV ObsosDocument5 pagesHPV ObsosRyan SadonoNo ratings yet
- Efecto de Hiv1 en Mujeres Embarazadas de RwandaDocument8 pagesEfecto de Hiv1 en Mujeres Embarazadas de RwandaIsmaelJoséGonzálezGuzmánNo ratings yet
- Syphilis in PregnancyDocument38 pagesSyphilis in PregnancydrirrazabalNo ratings yet
- Ajol File Journals - 394 - Articles - 168216 - Submission - Proof - 168216 4693 432812 1 10 20180314Document6 pagesAjol File Journals - 394 - Articles - 168216 - Submission - Proof - 168216 4693 432812 1 10 20180314God'stime OgeNo ratings yet
- PresusDocument6 pagesPresusFrishia DidaNo ratings yet
- Vulvovaginal Candidiasis - Prevalence and Analysis of Associated Risk Factors Among Women of Reproductive Age Group in Vindhya RegionDocument8 pagesVulvovaginal Candidiasis - Prevalence and Analysis of Associated Risk Factors Among Women of Reproductive Age Group in Vindhya RegionIJAR JOURNALNo ratings yet
- The Burden of HIV Infection Among Women Attending Antenatal Clinic in A Semi-Urban Nigerian TownDocument6 pagesThe Burden of HIV Infection Among Women Attending Antenatal Clinic in A Semi-Urban Nigerian TownDavid MorgNo ratings yet
- Syphilis in Pregnancy - UpToDateDocument33 pagesSyphilis in Pregnancy - UpToDateGiuliana FloresNo ratings yet
- Risk Factors For Cervical Cancer: Results From A Hospital-Based Case-Control StudyDocument7 pagesRisk Factors For Cervical Cancer: Results From A Hospital-Based Case-Control StudyIntania RosatiNo ratings yet
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNo ratings yet
- Cervical Cancer Awareness, Screening and Vaccination Among Female Nursing Students of University of GhanaDocument7 pagesCervical Cancer Awareness, Screening and Vaccination Among Female Nursing Students of University of GhanaIJAR JOURNALNo ratings yet
- Management of Vaginal Discharge Syndrome: How Effective Is Our Strategy?Document4 pagesManagement of Vaginal Discharge Syndrome: How Effective Is Our Strategy?Epi PanjaitanNo ratings yet
- Piis258953702200061x PDFDocument11 pagesPiis258953702200061x PDFRong LiuNo ratings yet
- 1 Infants HIV ArticleDocument14 pages1 Infants HIV ArticleSarah MoffattNo ratings yet
- HIV Retesting of HIV-Negative Pregnant Women in The Context of Prevention of Mother-to-Child Transmission of HIV in Primary Health Centers in Rural Zambia: What Did We Learn?Document6 pagesHIV Retesting of HIV-Negative Pregnant Women in The Context of Prevention of Mother-to-Child Transmission of HIV in Primary Health Centers in Rural Zambia: What Did We Learn?nabilahbilqisNo ratings yet
- 718-1519-1-SM 2Document6 pages718-1519-1-SM 2NicoleNo ratings yet
- Breast Cancer Awareness Among Health ProfessionalsDocument3 pagesBreast Cancer Awareness Among Health ProfessionalsWac GunarathnaNo ratings yet
- Cervical CA Proposal Jan152010Document21 pagesCervical CA Proposal Jan152010redblade_88100% (2)
- Nursing Open - 2022 - Mukosha - Knowledge Attitude and Practice Towards Cervical Cancer Screening Among Women Living WithDocument10 pagesNursing Open - 2022 - Mukosha - Knowledge Attitude and Practice Towards Cervical Cancer Screening Among Women Living Withluwi mwanguNo ratings yet
- Predictores Tempranos Del Síndrome de Guillain-Barré en El Curso de La Vida de Las MujeresDocument9 pagesPredictores Tempranos Del Síndrome de Guillain-Barré en El Curso de La Vida de Las Mujeresfrancisco bacaNo ratings yet
- Effect of Interventions in Reducing The Rate of Infection After Cesarean DeliveryDocument6 pagesEffect of Interventions in Reducing The Rate of Infection After Cesarean DeliveryEdwin mudumiNo ratings yet
- Obstetric Infections and Clinical Characteristics of Maternal Sepsis: A Hospital Based Retrospective Cohort StudyDocument12 pagesObstetric Infections and Clinical Characteristics of Maternal Sepsis: A Hospital Based Retrospective Cohort StudyblanquishemNo ratings yet
- Bronquiolite Amam.Document13 pagesBronquiolite Amam.gabibarbozaNo ratings yet
- Gynecologic Cancer Types Causes and Therapeutic ApproachesDocument4 pagesGynecologic Cancer Types Causes and Therapeutic ApproachesVuong Xuan Hong QuangNo ratings yet
- Routine Screening in A California Jail: Effect of Local Policy On Identification of Syphilis in A High-Incidence Area, 2016-2017Document8 pagesRoutine Screening in A California Jail: Effect of Local Policy On Identification of Syphilis in A High-Incidence Area, 2016-2017Siti Mediana ShakilaNo ratings yet
- Neonatal Sepsis in S Asia - A Huge Burden and Spiralling AMRDocument5 pagesNeonatal Sepsis in S Asia - A Huge Burden and Spiralling AMRdrdrNo ratings yet
- Vaccines 08 00124 PDFDocument21 pagesVaccines 08 00124 PDFSaúl Alberto Kohan BocNo ratings yet
- YogaDocument13 pagesYogaKarina NathaniaNo ratings yet
- Interpersonal Trauma and Aging-Related Genitourinary Dysfunction in A National Sample of Older WomenDocument7 pagesInterpersonal Trauma and Aging-Related Genitourinary Dysfunction in A National Sample of Older WomenKarina NathaniaNo ratings yet
- Influenza and Pregnancy No Time For Complacency.5Document4 pagesInfluenza and Pregnancy No Time For Complacency.5Karina NathaniaNo ratings yet
- Five Year Contraceptive Efficacy and Safety of A.11Document8 pagesFive Year Contraceptive Efficacy and Safety of A.11Karina NathaniaNo ratings yet
- Correlation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliDocument3 pagesCorrelation Between Body Mass Index and Intraocular Pressure at Eye Clinic Mangusada Hospital, BaliKarina NathaniaNo ratings yet
- Research Article: Diagnostic Performance of A Novel Noninvasive Workup in The Setting of Dry Eye DiseaseDocument6 pagesResearch Article: Diagnostic Performance of A Novel Noninvasive Workup in The Setting of Dry Eye DiseaseKarina NathaniaNo ratings yet
- Research Article: Retinal Structural and Microvascular Alterations in Different Acute Ischemic Stroke SubtypesDocument10 pagesResearch Article: Retinal Structural and Microvascular Alterations in Different Acute Ischemic Stroke SubtypesKarina NathaniaNo ratings yet
- Heat Treatment Training ManualDocument118 pagesHeat Treatment Training ManualPravin VisputeNo ratings yet
- Bergeron - Process 12345Document3 pagesBergeron - Process 12345SOUTH HINDI DOUBBED NEW MOVIESNo ratings yet
- 3D Numerical Modeling of A Landslide in SwitzerlandDocument6 pages3D Numerical Modeling of A Landslide in Switzerlandadela2012No ratings yet
- DAA ProfileDocument50 pagesDAA ProfileFarixxa AszNo ratings yet
- A Brief Study On Market Sructure and Demand Analysis of Hindustan Unilever LimitedDocument65 pagesA Brief Study On Market Sructure and Demand Analysis of Hindustan Unilever LimitedShivangi AgrawalNo ratings yet
- Lesson Plan MiraDocument5 pagesLesson Plan Miraika pratamaNo ratings yet
- A Step by Step Guide To Creating A Media StrategyDocument8 pagesA Step by Step Guide To Creating A Media StrategyAaron LifordNo ratings yet
- 03 - Baritone Saxophone (E Flat) - UntitledDocument3 pages03 - Baritone Saxophone (E Flat) - UntitledFuNo ratings yet
- What Is Hologram Technology?Document4 pagesWhat Is Hologram Technology?Fathi Elrahman AgilNo ratings yet
- Chapter 10 - Work Measurements and StandardsDocument72 pagesChapter 10 - Work Measurements and StandardsTGTrindadeNo ratings yet
- A Study On Applications of Wavelets To Data MiningDocument11 pagesA Study On Applications of Wavelets To Data MiningAziz Ur RehmanNo ratings yet
- Synthesis Essay - DluceDocument3 pagesSynthesis Essay - Dluceapi-550300197No ratings yet
- Fringe Finds Focus - Developments and Strategies in Aboriginal Writing in En... - EBSCOhostDocument11 pagesFringe Finds Focus - Developments and Strategies in Aboriginal Writing in En... - EBSCOhostKarima AssaslaNo ratings yet
- Gunn-The and The Individual: Ross ScientistDocument7 pagesGunn-The and The Individual: Ross ScientistDoor URNo ratings yet
- ClassVI - EPA SummaryDocument14 pagesClassVI - EPA SummarySakshi SinghNo ratings yet
- Topographic Map of Higgins SouthDocument1 pageTopographic Map of Higgins SouthHistoricalMapsNo ratings yet
- Meeting 1: A Past Time To RememberDocument12 pagesMeeting 1: A Past Time To RememberAmyunJun CottonNo ratings yet
- TMobile Call Center PlansDocument16 pagesTMobile Call Center PlansNews10NBCNo ratings yet
- Palm Oil-External Analysis, Competitive & Strategic Group MapDocument4 pagesPalm Oil-External Analysis, Competitive & Strategic Group Mapfaatin880% (1)
- Java Technology Concept MapDocument1 pageJava Technology Concept Mapkostas.karis100% (2)
- Segno Ceramics Glaze Line G.VT Extension LayoutDocument1 pageSegno Ceramics Glaze Line G.VT Extension LayoutNarsing Ramesh BabuNo ratings yet
- Sep 1314-1990Document1 pageSep 1314-1990amit gajbhiyeNo ratings yet
- Literature Review of Pension FundDocument8 pagesLiterature Review of Pension Funddhjiiorif100% (1)
- Java Crud CodeDocument26 pagesJava Crud CodeleinadmofficialNo ratings yet
- HP Care Services Definitions: GuideDocument2 pagesHP Care Services Definitions: Guideamxrpm1570No ratings yet
- ASTM B179-11 Standard Specification For Aluminum Alloys IngotsDocument12 pagesASTM B179-11 Standard Specification For Aluminum Alloys IngotsDemian LópezNo ratings yet