You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- (Hydraulic & Pneumatic) Quiz #4Document3 pages(Hydraulic & Pneumatic) Quiz #4mellon3duwenNo ratings yet
- CAT 01 Hydraulic Fundamental Student GuideDocument106 pagesCAT 01 Hydraulic Fundamental Student Guidewarshipvn100% (6)
- 8 - Kaplan Turbines PDFDocument28 pages8 - Kaplan Turbines PDFMuhammad FirdausNo ratings yet
- Ch17 - Heat Transfer by ConvectionDocument32 pagesCh17 - Heat Transfer by ConvectionSyed Hasif Sy MohamadNo ratings yet
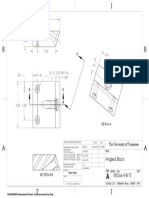
- Angled Block ME366-HW15: The University of TennesseeDocument1 pageAngled Block ME366-HW15: The University of TennesseekinleyNo ratings yet
- Tuned Track and Locomotion For Midterm 1 - Not Due: BME 473 Applied BiomechanicsDocument3 pagesTuned Track and Locomotion For Midterm 1 - Not Due: BME 473 Applied BiomechanicskinleyNo ratings yet
- Project #2 Topology OptimizationDocument24 pagesProject #2 Topology OptimizationkinleyNo ratings yet
- BME 449 Fall 2021 Experiement ProposalDocument1 pageBME 449 Fall 2021 Experiement ProposalkinleyNo ratings yet
- Fluid Mechanics Assignment Topic: - Laminar and Turbulent Flow Through Pipes:stress and Velocity DistributionDocument9 pagesFluid Mechanics Assignment Topic: - Laminar and Turbulent Flow Through Pipes:stress and Velocity DistributionJatin kuharNo ratings yet
- Tutorial 1: Introduction To Fluid PowerDocument2 pagesTutorial 1: Introduction To Fluid Powerzul hilmiNo ratings yet
- LM 5000D - Hydraulic System - 150000Document32 pagesLM 5000D - Hydraulic System - 150000bruno rafael Rafael100% (1)
- 4 - Hydraulics-1 PDFDocument3 pages4 - Hydraulics-1 PDFMohamed MahmoudNo ratings yet
- Pump Report 11402 Felix TamezDocument1 pagePump Report 11402 Felix TamezRodolfo Santiago EsquitinNo ratings yet
- B+V ELEVATOR SIDE DOOR Collar Type VS09 A4Document19 pagesB+V ELEVATOR SIDE DOOR Collar Type VS09 A4Игорь ШиренинNo ratings yet
- CP-533E / CS-533E Vibratory Compactor Hydraulic System: Lines GP - PropelDocument2 pagesCP-533E / CS-533E Vibratory Compactor Hydraulic System: Lines GP - PropelMayumi Lizarme BuezoNo ratings yet
- Boundary Layer Flow Over A Flat Plate PDFDocument6 pagesBoundary Layer Flow Over A Flat Plate PDFKelvin liewNo ratings yet
- Pitot Tube Fluids EssayDocument12 pagesPitot Tube Fluids EssaysceroxNo ratings yet
- Fire Systems Hydro Uni NB NKDocument24 pagesFire Systems Hydro Uni NB NKquoc khanh NgoNo ratings yet
- Hydraulic MachinesDocument43 pagesHydraulic MachinesRajesh MeppayilNo ratings yet
- Assignment No.2Document5 pagesAssignment No.2Nonsikelelo GobozaNo ratings yet
- تجربة 3Document3 pagesتجربة 3Aymen AbdulrahmanNo ratings yet
- CFD DafDocument10 pagesCFD DafSong Nguyen NguyenNo ratings yet
- 13A01408 Mechanics of FluidsDocument2 pages13A01408 Mechanics of FluidsarunNo ratings yet
- Apco Air Valve GuideDocument12 pagesApco Air Valve Guideanon_711152122No ratings yet
- Cai XuanDocument147 pagesCai Xuanbu7amudNo ratings yet
- Flare KO Drum Rev 2Document11 pagesFlare KO Drum Rev 2soufienNo ratings yet
- ME2134E/TME2134 Fluid Mechanics IDocument13 pagesME2134E/TME2134 Fluid Mechanics IChen WanyingNo ratings yet
- Laboratory of BuildingDocument22 pagesLaboratory of BuildingAddeArifinNo ratings yet
- Flow MeasurementsDocument1 pageFlow MeasurementsSUPAPORN KLABKLAYDEENo ratings yet
- Membranes and SailsDocument27 pagesMembranes and SailsgoharmahmoodkhokharNo ratings yet
- Centrifugal Pump SystemsDocument92 pagesCentrifugal Pump Systemsvijay kumarNo ratings yet
- 2 LaminarFlowPipes&Annuli NewtonianDocument24 pages2 LaminarFlowPipes&Annuli NewtoniankelrzNo ratings yet
- Experiment BernoulliDocument17 pagesExperiment BernoulliHafiniHambali94% (33)
- 17th International Conference On Multiphase Technology 2015: Cannes, France 10 - 12 June 2015Document6 pages17th International Conference On Multiphase Technology 2015: Cannes, France 10 - 12 June 2015kglorstadNo ratings yet